
Abstract
Background:
Exercise therapy is the cornerstone of patellofemoral (PF) pain management. However, whether squat exercises are therapeutic or detrimental depends on their technique and the resulting load on the PF joint.
Purpose/Hypothesis:
The purpose of this study was to investigate whether real-time feedback to position the center-of-pressure (COP) anteriorly could reduce the PF joint reaction force and stress during bodyweight double-leg squatting. It was hypothesized that an anterior COP position would decrease the PF joint reaction force and stress without changing the trunk flexion angle, whereas a posterior COP position would increase the PF joint reaction force and stress.
Study Design:
Controlled laboratory study.
Methods:
Sixteen men (age, 22.9 ± 1.5 years; height, 173.6 ± 5.2 cm; and body mass, 63 ± 6.8 kg) performed double-leg squatting under 4 conditions—natural, anterior, middle, and posterior COP. Kinematic and kinetic data were obtained via standard 3-dimensional motion analysis and force plate data. The PF joint reaction force and stress were calculated via a musculoskeletal modeling approach.
Results:
PF joint loading was significantly reduced in the anterior and middle COP conditions compared with the natural condition. At 90° of knee flexion, the PF joint reaction force decreased by 11% and 9% in the anterior and middle COP conditions, respectively, compared with that in the natural condition (anterior: P < .001, 95% CI −0.996 to −0.277 bodyweight; middle: P = .011, 95% CI −0.795 to −0.087 bodyweight). Moreover, the peak PF joint stress decreased by 9% and 7% in the anterior and middle COP conditions, respectively, compared with the natural condition (anterior: P = .001, 95% CI −0.659 to −0.146 MPa; middle: P = .023, 95% CI −0.600 to −0.036 MPa). Compared with those under the natural condition, the trunk forward inclination angles did not increase under anterior or middle COP conditions.
Conclusions:
Real-time feedback for anterior COP positioning is an effective strategy for reducing the PF joint reaction force and stress during double-leg squatting without increasing trunk forward lean.
Clinical Relevance:
The incorporation of real-time feedback regarding the anteroposterior COP position is useful for reducing PF joint loading during double-leg squatting, which may be helpful in the rehabilitation of PF pain patients. Instructions to position the COP anteriorly may also be useful in reducing PF joint loading during double-leg squatting.
Patellofemoral pain (PFP) is a common knee disorder, and its prevalence is estimated to be >20% in adolescents and adults. 33 Exercise therapy is the cornerstone of PFP management, 25 and strengthening the quadriceps is one of its goals. 5 Squat exercises are commonly incorporated into exercise therapy for patients with PFP 23 and may be more effective than open kinetic chain exercises such as straight leg raises. 2 In addition, squatting has an advantage in simulating eccentric loading during functional activities. 5 However, improper squatting techniques may worsen or cause symptoms.12,20,35 Patients with PFP demonstrate greater patellofemoral (PF) joint force during weightbearing activities—such as squatting, stair climbing, and running 37,40—and a large PF joint reaction force represents a possible mechanism causing pain.15,31 Therefore, whether squatting is therapeutic or detrimental depends on its technique and associated PF loading. Knowledge of the factors influencing PF loading during squatting is informative for rehabilitation and modifications of daily activities for patients with PFP.1,12,15
PF joint reaction force and PF joint stress during weightbearing activities are estimated via musculoskeletal modeling and are associated with the quadriceps force and knee extension moment.1,36 The instructions to position the knee behind the toes are often used to reduce the PF joint reaction force and knee extension moment.4,14,20,27,35 However, the strict restriction of forward knee movement simultaneously increases forward trunk inclination and lumbar lordosis, which is a concern because of the increased load on the lower back.14,26 Real-time feedback regarding PF joint reaction force also reduces the PF joint reaction force for patients with PFP during bodyweight squatting, 21 whereas its clinical use is limited. Recent studies have reported that an anterior center-of-pressure (COP) position is associated with a smaller knee extension moment during double-leg squatting.16,17 Interlimb asymmetry in the anteroposterior (AP) COP position is also associated with asymmetry in the knee extension moment during double-leg squatting after anterior cruciate ligament reconstruction. 7 The feedback on the COP position can be provided via a force plate and may not increase the trunk flexion angle during squatting. 16 However, evidence regarding the effects of the AP-COP position on the PF joint reaction force and stress is very limited; 1 study showed that a difference in the AP-COP position of 9.1% of the foot length led to a difference of 6% in the knee extension moment during double-leg squatting. 16 Another study reported that a difference in the AP-COP position of approximately 30% of the foot length led to a difference in 60% of the vastus medialis electromyographic activity during squatting. 22 Therefore, a large change in the AP-COP position may control the PF joint load during squatting.
This study aimed to determine the effects of real-time feedback regarding the AP-COP position on the PF joint reaction force, PF joint stress, and knee extension moment during bodyweight double-leg squatting. We hypothesized that an anterior COP position would decrease the PF joint reaction force, knee extension moment, and quadriceps force without changing the trunk flexion angle, whereas a posterior COP position would increase the PF joint reaction force, knee extension moment, and quadriceps force.
Methods
Participants
This study was conducted as part of a research project investigating the effects of changing the COP position on lower extremity biomechanics during squatting. Data were collected in separate sessions from those used in the other studies. The sample size was determined based on a previous study. 16 We recruited 16 young male participants (age, 22.9 ± 1.5 years; height, 173.6 ± 5.2 cm; body mass, 63 ± 6.8 kg) who were familiar with squatting exercises because this study asked participants to control their COP position while squatting. The inclusion criteria were as follows: no pain during double-leg squatting, no history of musculoskeletal injury within the previous 6 months, and no lower extremity or trunk surgery. Written informed consent was obtained from each participant before participation. This study was approved by the institutional review board of the Faculty of Health Sciences, Hokkaido University (21-59).
Procedures and Data Collection
After providing a 5-minute warm-up to participants using a bicycle ergometer at a self-selected pace, we attached 38 markers to the iliac crest, anterior and posterior superior iliac spines, medial and lateral femoral epicondyles, medial and lateral malleoli, second metatarsal head and base, fifth metatarsal head and heel, and thigh and shank marker clusters on the lateral side. In addition, we placed 12 markers on the head, trunk, and upper extremity to build a full-body musculoskeletal model. First, we recorded a static standing trial to scale the musculoskeletal model of each participant. The participants then performed 5 consecutive squats under the following 4 conditions: (1) natural condition, without any specific instruction or feedback; (2) anterior COP condition; (3) middle COP condition; and (4) posterior COP condition. For all the conditions, the participants stood on 2 force plates, 1 for each foot, and aligned their toes at the predetermined line to measure the 3 target AP-COP positions within the foot for each participant. 16 The target AP-COP positions of the anterior, middle, and posterior COP conditions were adjusted at the first metatarsal head, first tarsometatarsal joint, and navicular tubercle of each participant, respectively. We instructed the participants to squat down until their thighs were parallel to the floor and then stand upright. No instructions were given regarding forward trunk inclination or the AP knee position. A metronome was used so that the participants could descend, ascend, and stand still for 2 seconds each.
First, the natural condition was recorded. Then, the anterior, middle, and posterior COP conditions were recorded in random order. Data were collected using a 3-dimensional motion analysis system (Cortex Version 5.0.1; Motion Analysis Corporation) with 7 synchronized cameras (Hawk cameras; Motion Analysis Corporation) and 2 force plates (Type 9286; Kistler AG). The sampling rates were set to 200 Hz for the marker coordinate data and 1000 Hz for the force plate data.
Real-time Feedback on the COP Position
Feedback on the AP-COP position was provided in real-time via a 27-inch monitor that was placed 1 m in front of the participants’ toes 16 (Figure 1). The AP-COP position was calculated as the percentage of foot length (% foot length) from the heel (0%) to the toe (100%) and displayed as bar graphs for each foot via a custom LabView program Version 21 (National Instruments Corp).7,16 Anterior and posterior movements of the COP position were indicated in real-time by an increase or a decrease in the height of the bar graphs. 16 In each condition, except the natural condition, a box indicating the target COP position, with a range of ±2.5% of foot length, was displayed with bar graphs 16 (Figure 2). The participants were instructed to maintain their AP-COP position within the target box throughout the squatting tasks. For the natural condition, the participants were instructed to look at the monitor, but nothing was displayed on the monitor. The screen was also replicated on the operating personal computer and the examiner checked the participant's COP position during the experiments.

Squatting with real-time feedback regarding the AP-COP position. AP-COP, anteroposterior center of pressure.

Real-time feedback on the AP-COP position. The participants were asked to maintain their AP-COP position within the target box (indicated by black arrows) while squatting under the anterior, middle, and posterior COP conditions. The box represents the target COP position, with a range of ±2.5% of the foot length. The left and right AP-COP positions are shown separately, ranging from 20% (bottom) to 80% (top) of the foot length. (A) Anterior COP condition (first metatarsal head). (B) Middle COP condition (first tarsometatarsal joint). (C) Posterior COP condition (navicular tubercle). AP-COP, anteroposterior center of pressure.
Data Processing and Reduction
The dominant leg—defined as the leg preferred for kicking a ball—was analyzed because the knee extension moment was greater on the dominant side than on the nondominant side. 17 Kinematic and ground-reaction force data were low-pass filtered via a zero-lag fourth-order Butterworth filter with a cutoff frequency of 6 Hz. The trajectory gaps in the anterior superior iliac spine marker during squatting were filled with the iliac crest and posterior superior iliac spine markers. 28 Musculoskeletal modeling was performed via OpenSim (Version 4.4; Stanford University). 9 We used a model customized for the squatting task 6 from a previously developed and validated full-body model 32 as the generic model to be scaled for each participant. This model had 37 degrees of freedom and 80 muscle-tendon units actuating the lower limbs. 32 Joint kinematics were calculated via the inverse kinematics tool. The single-degree-of-freedom tibiofemoral joint was modeled,32,41 and patellar motion was constrained relative to the knee flexion angle according to a previous study.32,38 These tibiofemoral and PF joint models were developed to better estimate the anatomic center of rotation and patellar force transmission. 32 The results of inverse kinematics were then used with ground-reaction force data to estimate the joint moment in the inverse dynamics tool and the muscle force/activation in the static optimization tool. The PF joint reaction force was calculated via the joint reaction analysis tool in OpenSim by applying the muscle forces from static optimization. Joint reaction analysis in OpenSim involves multibody dynamics calculations similar to inverse dynamics but with muscle forces. Quadriceps force applied PF compressive force by its force vectors.10,29 In this study, the PF joint reaction force was referred to as the sagittal plane resultant force applied to the femur and represented in the patellar coordinate system. In addition, the PF joint stress was estimated by dividing the PF joint reaction force by the PF joint contact area. The PF joint contact area was determined as a function of the knee flexion angle (x) via the following equation: 3,34

The PF joint reaction force and knee extension moment were derived at 60° and 90° of knee flexion. 35 In addition, the peak values of the PF joint reaction force, PF joint stress, and knee extension moment during the descent phase were derived. Moreover, the ankle dorsiflexion angle and trunk forward inclination angle were also determined because these variables can affect the PF joint reaction force and/or knee extension moment during squatting.14,17,20,27,35 For the AP-COP position, the mean positions were calculated 18 in the descent phases of knee flexion of >60°. 18 The PF joint reaction force was normalized to each participant's body weight (BW; product of body mass and gravity acceleration) and the knee extension moment was normalized to each participant's body mass. 11 All variables were averaged across the middle 3 of the 5 consecutive squats.
Statistical Analysis
One-way repeated-measures multivariate analysis of variance (MANOVA) was performed to compare the outcomes between the squatting conditions. Post hoc univariate repeated-measures analysis of variance (ANOVA) and the Bonferroni test were performed when the results of the MANOVA were significant. The statistical significance level was set at P < .05. Statistical analyses were performed via the IBM SPSS Statistics software Version 22 (IBM Corporation).
Results
The target AP-COP positions were 74.3% (1.5), 53.3% (1.7), and 36.6% (1.1) of the foot length in the anterior, middle, and posterior COP conditions, respectively. The AP-COP positions were significantly different between the conditions, except between the natural and posterior COP conditions (Table 1). Although the mean values for all participants were almost within the target range (±2.5% of foot length), the COP position of 5 participants in the anterior COP condition was posterior to the target range by up to −7.2% of foot length. For the middle and posterior conditions, the AP-COP position was anterior to the target range for 4 and 8 participants, up to 5.1% and 5.7% of the foot length, respectively. No significant difference was found in the peak knee flexion angle among the 4 conditions (P = .147). MANOVA revealed a significant difference in the outcomes between the squatting conditions (Wilks lambda = 0.006; P < .001).
Comparisons of AP-COP Position and Knee Flexion Angles in the 4 Conditions of the Squat Descent Phase a

Data are presented as mean (SD) AP-COP, anteroposterior center of pressure; COP, center of pressure.
Indicates a significant difference from the natural condition (P < .05).
Indicates a significant difference from the anterior condition (P < .05).
Indicates a significant difference from the middle condition (P < .05).
The PF joint reaction force significantly differed between the squatting conditions at 60° and 90° of knee flexion and for the peak values (all, P < .001) and significantly lower in the anterior COP condition than in the natural (60°, P < .001, 95% CI −0.507 to −0.158 BW; 90°, P < .001, 95% CI −0.996 to −0.277 BW; peak, P < .001, 95% CI −0.678 to −0.096 BW) and posterior COP conditions (60°, P = .001, 95% CI −0.461 to −0.111 BW; 90°, P = .006, 95% CI −0.955 to −0.142 BW; and peak, P = .075, 95% CI −0.708 to −0.024 BW) (Figure 3). Moreover, the middle COP condition resulted in a significantly smaller PF joint reaction force than the natural (60°, P = .003, 95% CI −0.389 to −0.075 BW; 90°, P = .011, 95% CI −0.795 to −0.087 BW; peak, P = .041, 95% CI −0.680 to −0.011 BW) and posterior COP conditions (60°, P = .001, 95% CI −0.296 to −0.077 BW; 90°, P = .048, 95% CI −0.704 to −0.002 BW). No significant difference was found in the PF joint reaction force between the natural and posterior conditions (P > .999).
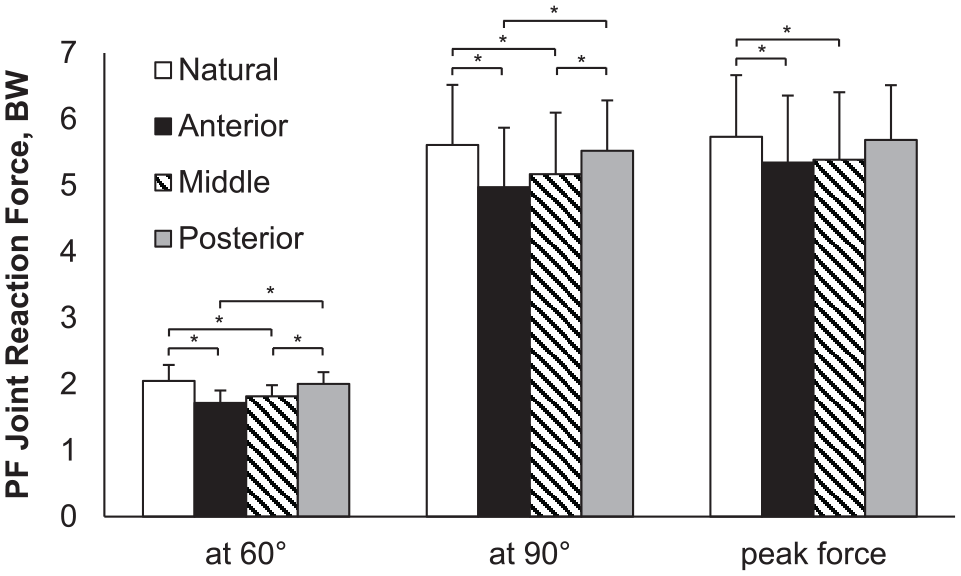
Comparisons of PF joint reaction force at 60° and 90° of knee flexion and for the peak joint reaction force. Error bars indicate SD. PF, patellofemoral; BW, bodyweight.
In terms of the peak PF joint stress, a significant difference was found between the squatting conditions (P < .001). The peak PF joint stress was significantly lower in the anterior COP condition than in the natural and posterior COP conditions (natural: P = .001, 95% CI −0.659 to −0.146 MPa; posterior: P = .020, 95% CI −0.661 to −0.046 MPa) (Figure 4). In addition, the middle COP condition resulted in a significantly lower peak PF joint stress than the natural condition (P = .023, 95% CI −0.600 to −0.036 MPa).

Comparisons of PF joint stress at 60° and 90° of knee flexion and for the peak stress. Error bars indicate SD. PF, patellofemoral.
The knee extension moment significantly differed among the squatting conditions at 60° and 90° of knee flexion, and for the peak moment (all, P < .001) and significantly smaller in the anterior COP condition than in the natural (all, P < .001), middle (all, P < .001), and posterior COP conditions (all, P < .001) (Figure 5). In addition, the middle COP condition resulted in a significantly smaller knee extension moment than the posterior COP condition (60°, P = .003; 90°, P = .033).

Comparisons of the knee extension moment at 60° and 90° of knee flexion and for the peak moment. Error bars indicate SD.
The ankle dorsiflexion and forward trunk inclination angles were also significantly different between the squatting conditions (Table 2). The ankle dorsiflexion angle was significantly greater in the anterior COP condition at 60° and 90° of knee flexion and for the peak angle than in the natural, middle, and posterior COP conditions (P≤ .018, P≤ .01, and P≤0.001, respectively). The middle COP condition also exhibited a significantly larger ankle dorsiflexion angle than the natural COP condition at 60° and 90° of knee flexion and posterior COP conditions at 60° and 90° of knee flexion and for the peak angle (P≤ .003 and P≤ .001, respectively). The forward trunk inclination was significantly greater in the natural condition than in the middle and posterior COP conditions (P≤ .006 and P = .001, respectively). No significant difference was found in the forward trunk inclination angle between the natural and anterior COP conditions.
Comparisons of Kinematic Variables in the 4 Conditions of the Squat Descent Phase a
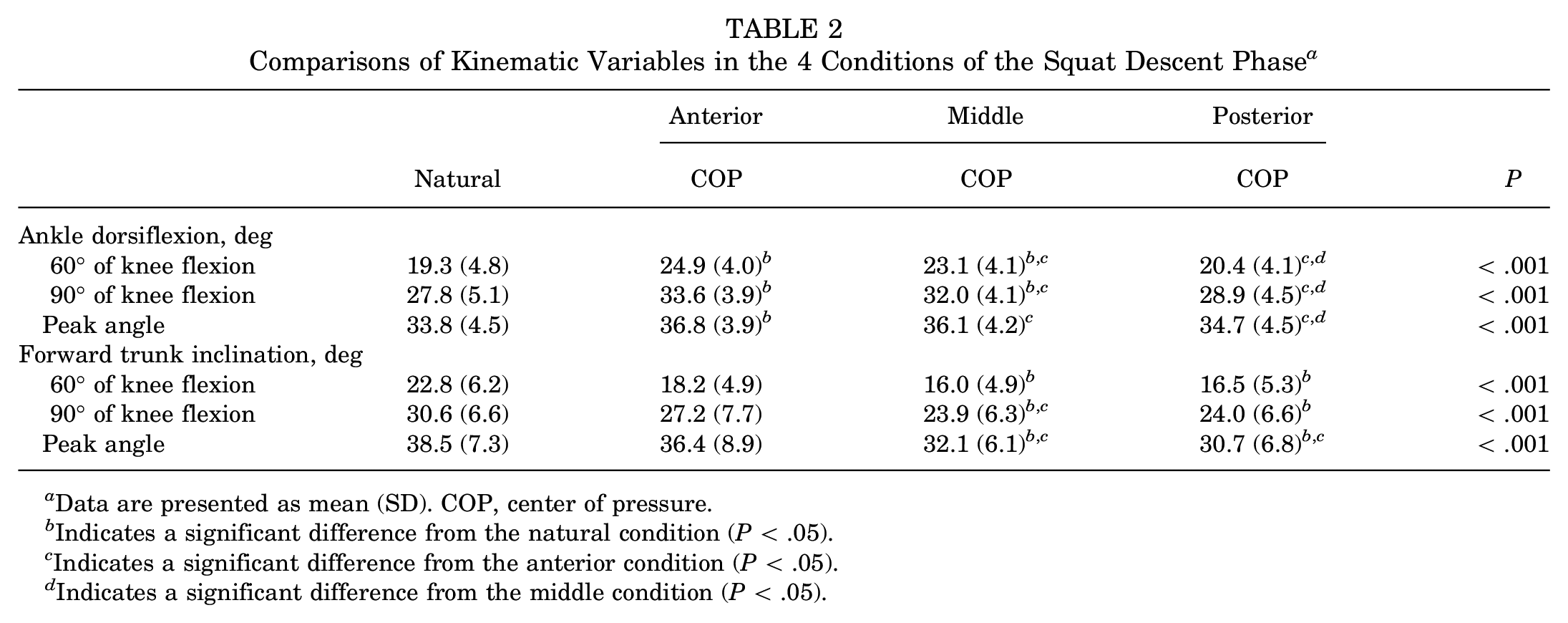
Data are presented as mean (SD). COP, center of pressure.
Indicates a significant difference from the natural condition (P < .05).
Indicates a significant difference from the anterior condition (P < .05).
Indicates a significant difference from the middle condition (P < .05).
Discussion
Our results revealed that changes in the AP-COP position were associated with changes in the PF joint reaction force and stress during double-leg squatting. Under the anterior and middle COP conditions, the PF joint reaction force and stress were significantly reduced compared with those under the natural condition without increasing forward trunk inclination. These findings support our a priori hypotheses and are informative for controlling the PF joint load during squatting.
The mean AP-COP positions were within the target range, and there was no significant difference in the peak knee flexion angles among the 4 experimental conditions. Therefore, the squatting tasks with real-time feedback were performed as intended. The PF joint reaction force during squatting has been reported with a wide range between ~1 and 18 BW. 15 The mean PF joint reaction force in our study was 5.61 BW at 90° of knee flexion under the natural condition, which is lower than that reported in a previous study on healthy young women (~7.5 BW) 43 and greater than that reported in another study on patients with PFP (4.64 BW). 21 The PF joint reaction force in our study is considered reasonable for comparing the 4 conditions.
The PF joint reaction force was greater at 90° of knee flexion than at 60° of knee flexion, which is consistent with previous studies.12,36 When PF joint pain is induced by squatting, decreasing the knee flexion angle is the first consideration for reducing PF joint pain and loading. 30 However, such instructions are not practical for returning to functional activities, including sports, and factors other than the knee flexion angle that influence PF joint loading should be considered in the course of rehabilitation. The PF joint reaction force at 90° of knee flexion was decreased by 11% and 9% in the anterior and middle COP conditions, respectively, compared with the natural condition, which is comparable with the 12% reduction induced by maintaining the knee position behind the toes 1 and the 15% reduction induced by training with real-time PF joint reaction force feedback. 21 In addition, the peak PF joint stress was reduced by 9% and 7% in the anterior and middle COP conditions, respectively, compared with that in the natural condition, which is comparable with the 14% reduction induced by maintaining the knee position behind the toes. 1 The present findings indicate that biofeedback about the AP-COP position can be an alternative training method to reduce PF joint loading during squatting.
In this study—compared with the natural condition—the anterior COP condition resulted in a larger ankle dorsiflexion angle, and the middle COP condition resulted in a larger ankle dorsiflexion angle and a smaller forward trunk inclination angle. A more anterior COP position in the anterior and middle COP conditions would be associated with a more anterior center-of-mass position and would be achieved mainly by an increase in the ankle dorsiflexion angle rather than a change in the trunk flexion angle. AP center-of-mass movement is associated with ankle dorsiflexion but not with forward trunk inclination during double-leg squatting. 19 Previous studies have also reported that the ankle plantarflexion moment is strongly related to changes in the AP-COP position during squatting.13,16,22
Forward trunk inclination and the ankle dorsiflexion angles can also affect the PF joint reaction force and knee extensor moment during squatting.14,17,20,27,35 A larger trunk flexion angle is associated with a smaller knee extension moment,17,35 but increasing low back loading is of concern.14,26 In the present study, the anterior and middle COP conditions decreased PF joint loading without increasing forward trunk inclination, which is an advantage of training with real-time feedback on the AP-COP position. With respect to the ankle dorsiflexion angle, previous studies have shown that a larger ankle dorsiflexion angle was associated with a larger PF joint reaction force and knee extension moment,14,17,27,35 whereas the present study revealed that the anterior and middle COP conditions demonstrated significantly smaller PF joint reaction forces and larger ankle dorsiflexion angles than the natural COP condition. PF joint loading and the knee extension moment during squatting are associated with the moment arm of the knee joint relative to the ground-reaction force. Large ankle dorsiflexion and small forward trunk inclination are thought to increase the knee joint moment arm relative to the ground-reaction force.14,27 In contrast, the anterior COP position is thought to decrease the moment arm of the knee joint,7,16 and the AP-COP position is associated with the knee extension moment during squatting, independent of ankle dorsiflexion and forward trunk inclination. 17 In the anterior and middle COP conditions, the decrease in the moment arm induced by the anterior COP position may outweigh the increase in the moment arm induced by the large ankle dorsiflexion and small trunk forward inclination. These results suggest the robustness of real-time feedback regarding the AP-COP position to control the PF joint reaction force during squatting. Modifications in both the AP-COP position and the ankle dorsiflexion angle may be considered to reduce PF joint loading more effectively.
Our findings regarding the changes in the knee extension moment are consistent with the results of previous studies showing that a more anterior COP position was associated with a smaller knee extension moment and less quadriceps activity during double-leg squatting.16,17,22 The reduction in the PF joint reaction force was 11% at 90° of knee flexion, while the reduction in the knee extension moment was 22%. These results suggest that the decrease in the knee extension moment involves not only a decrease in the quadriceps force, which induces a greater PF joint load but also an increase in the knee-flexor muscle force. The anterior COP position is also associated with a larger ankle plantarflexion moment and hamstring and gastrocnemius activities.16,22 When estimating changes in the PF joint reaction force from changes in the knee extension moment, care should be taken to avoid the possibility of overestimation. In addition, an anterior COP position decreases quadriceps loading. As symptoms improve, avoiding an excessive anterior COP position to strengthen the quadriceps muscles may be beneficial.
The AP-COP position in the natural condition was 34.8% of the foot length, which is similar to the previously reported AP-COP position in patients with PFP (35.9% of the foot length). 21 Instruction to position the COP anterior to the first metatarsal head (middle COP condition) may be useful in reducing PF joint reaction forces. The PF joint force is significantly lower during running with a forefoot strike pattern than during running with a rearfoot strike,24,39,42 which supports the present findings. PFP is also aggravated during stair ambulation and jump-landing. 8 Instruction regarding the COP position during such weightbearing activities may reduce the PF joint reaction force, thereby reducing pain. However, it is unclear how much symptom improvement can be achieved by reducing the PF joint reaction force with COP position feedback. Future studies are needed to examine the effects of the COP position instructions on PFP and PF joint load during weightbearing activities.
Some limitations of this study should be acknowledged. First, we included only healthy male participants. Patients with PFP and/or females may demonstrate different kinetics and kinematics when the AP-COP position is changed. Second, double-leg squatting was performed with only body weight. The results may differ for squats with loaded weights. Finally, the PF joint reaction force was not directly measured; instead, it was estimated via musculoskeletal modeling.
Conclusion
Our results showed that the anterior and middle COP conditions reduced the PF joint reaction force by 11% and 9%, respectively, at 90° of knee flexion compared with the natural condition of double-leg squatting. In addition, the peak PF joint stress was reduced by 9% and 7% in the anterior and middle COP conditions, respectively, compared with the natural condition. Forward trunk inclination under the anterior and middle COP conditions was not increased compared with the natural condition. Real-time feedback to position the COP anteriorly is useful for reducing the PF joint reaction force and stress during double-leg squatting.
Footnotes
Final revision submitted July 23, 2024; accepted September 10, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by JSPS KAKENHI (grant numbers: JP20K19477 and JP23K10553). Part of the funding for H.T.’s work was provided by ORGO Inc. R.U. is an employee of ORGO Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Institutional Review Board of the Faculty of Health Sciences, Hokkaido University (21-59).