
Abstract
Background:
Concussions have previously been shown to have persistent neurological changes represented by altered reaction time and postural stability in high-level athletes. The effects of concussions on professional basketball players’ performance and subsequent injuries during the 90 days after return to play (RTP) have not been investigated.
Purpose/Hypothesis:
the purpose of this study was to evaluate player statistical performance and risk of musculoskeletal (MSK) injury within 90 days of RTP from a diagnosed concussion. It was hypothesized that within the 90 days after RTP from a concussion, players would be at a greater risk for MSK injury with an associated decrease in player statistical performance.
Study Design:
Descriptive epidemiology study.
Methods:
Concussions sustained by National Basketball Association (NBA) players between the 2015-2016 and 2021-2022 seasons, excluding the 2019-2020 season, were evaluated using a publicly available database. The database was queried to identify any MSK injury in the 90-day post-RTP period after a concussion, along with time loss after subsequent injury. Performance statistics were obtained from each player’s preindex season and postindex season, as well as defined time points within the 90-day post-RTP period. Each concussed player was matched 1 to 1 with a nonconcussed control using position, win shares, player efficiency rating, and points per game. MSK injury incidence and player statistics in the concussion group were compared with controls using unpaired Student t tests.
Results:
A total of 70 concussions were identified in 70 professional basketball players and included in this analysis. A total of 49 players sustained an MSK injury in the 90-day post-RTP period (70%). Compared with controls, the odds of sustaining an MSK injury in the concussed cohort were 11.3 times greater (95% CI, 5.04-25.2; P < .001). Games missed after subsequent MSK injury were similar between the concussed and control groups (P = .687). Comparisons over the 90-day post-RTP period did not reveal any significant changes in points per game, minutes per game, or true shooting percentage (P > .05). When compared with controls, no changes in performance statistics were significantly different (P > .05).
Conclusion:
Our analysis demonstrates that basketball players who sustain concussions are at a significantly increased risk for subsequent MSK injury within the 90-day post-RTP period but not player performance. Knowledge of this increased risk of MSK injury in concussed athletes can help guide concussion management for proper RTP and targeted rehabilitation in professional basketball players.
Keywords
In recent years, concussions have garnered significant attention in sports medicine. While concussions are more common in high-contact sports—such as football, ice hockey, rugby, and boxing 21 —they also occur in other sports like basketball, with a reported rate of 3.9 to 5.5 concussions per 10,000 athlete-exposures in high school athletes. 26 Another epidemiological study discovered concussion rates occurring in basketball to be higher among collegiate athletes compared with high school athletes (5.30 vs 1.55 per 1000 athlete-exposures). 8 Patel et al 33 demonstrated that approximately 9.7 concussions occurred per season in the National Basketball Association (NBA) over 20 years from 1999 to 2018. The incidence rates mentioned may be underestimated, as approximately one-third of athletes have sustained concussions that were not formally diagnosed. 30 While concussions in professional basketball athletes may be less common than those in other contact-forward sports, basketball players engage in demanding activities requiring rapid movement and decision-making, which may accentuate any neurologic compromise. Concussions have been shown to slow reaction times10,11 and compromise postural stability,6,13,14 which are both critical in a sport like basketball. In addition, concussions can lead to detrimental changes in gait patterns, which are significant predictors of injury in professional basketball.16-18,27
A recent systematic review found a 58% greater risk of lower extremity injury in college athletes after concussion compared with those without a history of concussion. 28 Similar findings are seen in NBA players as well; a 4.69 times greater risk of lower extremity injury in concussed players compared with control players has previously been shown. 20 However, there is sparse literature on the incidence of all musculoskeletal (MSK) injuries—including the upper extremity—after concussion. One study showed that collegiate football players are at a 2.36 times higher risk of upper extremity injury after concussion. 12 Although the exact mechanism contributing to this elevated injury risk in the upper extremity is unknown, previous studies have postulated it to be related to impaired upper extremity movements 25 or increased fall risk onto the upper extremity due to compromised gait and landing mechanics.24,27 The 90-day period immediately after concussion has been suggested as a period of heightened neurological deficit. 29 Other research demonstrating increased risk of lower extremity MSK injury used a 90-day period after return to play (RTP) to ensure athletes analyzed were participating in sporting events.5,15 Further, in professional basketball, 9 hockey, 22 and baseball, 7 the effects of concussion do not significantly impact player performance when compared with controls.
The effects of concussions on player performance and subsequent MSK injury during the 90 days after RTP have not been extensively studied—particularly in professional basketball. The primary purpose of this study was to determine the incidence of MSK injuries in the 90 days after RTP from concussion and the time loss from MSK injury. The secondary aim included evaluating player performance statistics. The authors hypothesized that players would face a greater risk of MSK injury and associated performance decline after a concussion.
Methods
Data Collection
This study was a retrospective review of a public database and was deemed exempt from the institutional review board (No. 21-009369). The study period includes 5 NBA seasons from 2015-2016 to 2020-2021, excluding the 2019-2020 season because of the coronavirus disease 2019 hiatus. Injury data—including date of injury, description of injury, and player movement to and from the injured list—were retrieved from Pro Sports Transactions (prosportstransactions.com). These data were further verified using individual player and game logs on Basketball-Reference (basketball-reference.com), which tracks time missed and is officially sourced by the NBA’s stats partner, SportRadar (SportRadar). Multiple NBA-related studies have used these databases previously.20,23,31-33,36,37
All concussions within the study period were collected using public databases. Players were excluded if they had inadequate 30-day follow-up due to the concussion occurring at the end of the season. Each player identified at this step was matched with 1 control player using previously reported methods.3,31 Basketball-Reference provides a similarity score for each NBA player, which gauges players’ likeness based on position, career duration, and win shares, representing a player’s contribution to team wins. The control for each injured player was selected based on the highest similarity score, as long as the control player had sufficient data logged. If there were insufficient data, the player with the next highest similarity score was used. To further evaluate the comparison to control players, unpaired 2-tailed Student t tests were conducted to compare age, height, body mass index (BMI), preindex player efficiency rating (PER), and preindex career points per game (PPG) between the injured and control groups. The term “index” refers to the season of the concussion. Control group statistics were sourced from the same NBA season corresponding to the injured player’s year in the league. For instance, if an injured player’s year of concussion was their seventh season in the NBA, the control player performance statistics were taken from their seventh season as well.
For each concussion and control player, demographic characteristics were collected— including position, age, height, BMI, and position. Subsequent MSK injury data in the 90 days immediately after RTP were also collected along with the following characteristics: date of injury, location of injury, and date of RTP from MSK injury. The location of injury was categorized as follows: foot, ankle, lower leg, knee, upper leg, torso, arm/shoulder, hand/wrist, and head/neck.5,15,20,35 Injuries were also categorized by type, according to what was stated in the injury description—sprain, strain, fracture, tendon tear, contusion, soreness, or miscellaneous. Miscellaneous injuries are those that do not have a specific type of injury listed in the description. It was also noted whether players sustained multiple MSK injuries within the 90-day period. Those players who received concussions were separated into 2 cohorts for further subgroup analysis—those with MSK injury (MSKi) and those without MSK injury (woMSKi). The control players without concussion were also separated into the same subgroups—MSKi and woMSKi. The MSKi subgroup was then used to compare MSK injury characteristics between the concussion and control cohorts, while the woMSKi subgroup was used to compare player performance between the concussion and control cohorts. The separation of analyses was done to minimize confounding variables, as having a subsequent MSK injury would alter performance statistics. Figure 1 outlines the complete methodology for player selection.

A flow chart demonstrating patient inclusion methodology and process of making a control cohort. MSK, musculoskeletal; MSKi, with a musculoskeletal injury; NBA, National Basketball Association; RTP, return to play; woMSKi, without a musculoskeletal injury.
Figure 2 outlines the subgroup analysis for both groups—MSKi and woMSKi. Those in the MSKi subgroup underwent analysis for RTP after an MSK injury. This included the characterization of the MSK injury using the number of injuries sustained, the location of the injury, time missed due to the injury, and the on-court position of the player. The control cohort was used to compare the odds of sustaining an MSK injury in the corresponding 90-day period of the matched concussed player. The controls were also used to compare the MSK injury characterization and time missed due to injury. The players in the control cohort who sustained an MSK injury were not included in the analysis for performance statistics.

A flow chart demonstrating 2 separate subgroup analyses: (A) MSKi. (B) woMSKi. MSK, musculoskeletal; MSKi, with musculoskeletal injury; RTP, return to play; woMSKi, without musculoskeletal injury.
Those in the woMSKi subgroup underwent further analysis of player performance statistics within the 90-day post-RTP period, the season prior, and the season after injury. At this point, players were excluded if they did not have a complete 90-day period due to the injury occurring at the end of the season or due to intermittent time loss throughout that period. These mean statistics were compared with the mean of the individual 1 to 1 matched cohort statistics. Player characteristics and player statistics were queried using Basketball Reference. 2 Basic player statistics in this study included PPG and minutes per game (MPG). Advanced statistics investigated included the true shooting percentage (TS%). The TS% measures overall shooting efficiency, accounting for field goals, 3-point field goals, and free throws. All 4 of the statistic measures include both regular season and playoff games. These performance statistics were gathered at 4 time points within the 90 days immediately after the RTP date. This includes the 2-week mark, 4-week mark, 2-month mark, and 3-month mark. The means of each performance statistic over the respective periods were used for analysis. For example, for the 4-week mark, the means were calculated using the statistics from 0 to 4 weeks. Performance statistics in the season before injury and the season after injury were also gathered to assess the long-term impact of concussion.
Statistical Analysis
For categorical variables, univariate 2-group comparisons were performed using chi-square tests. Univariate comparisons of player statistics over the 90-day post-RTP period were conducted using paired 2-tailed Student t tests, with the comparison done between the 2-week statistics and the 3-month statistics. Univariate comparisons of player individual statistics between their preindex season to their postindex season were conducted using paired 2-tailed Student t tests. Unpaired 2-tailed Student t tests were used to evaluate the changes in player statistics between the concussed and control cohorts. Odds ratios, 95% CIs, and standard errors were reported, where appropriate. Statistically significant differences were noted if P < .05. All analyses were conducted using R Version 4.2.3 (R Core Team) and Excel 2024 (Microsoft).
Results
General Characteristics of Professional Basketball Players With Concussions
A total of 70 concussions were identified in 70 NBA athletes from 2015 to 2021, excluding the 2019-2020 season. All demographic characteristics for professional basketball players who sustained a concussion—including age, height, BMI, on-court position, and time loss after concussion—are shown in Table 1.
Characteristics of NBA Players With Concussions a

Data are presented as mean ± SD, n (%), or mean (range). BMI, body mass index; MSK, musculoskeletal; NBA, National Basketball Association; RTP, return to play.
MSK Injury Incidence, Characteristics, and RTP Data
Out of the 70 players with a concussion, 49 players sustained an MSK injury in the 90-day post-RTP period (70%). Out of the 70 players in the control cohort, 12 players sustained an MSK injury in a corresponding 90-day period (17%). Compared with controls, the odds of sustaining an MSK injury in the concussed cohort were 11.3 times greater (95% CI, 5.04-25.2; P < .001). With respect to the demographic characteristics of the 2 cohorts, no significant differences were noted in position distribution (P > .05) (Table 2). Also, 76% of the concussed players with an MSK injury sustained 1 singular injury in the 90-day period, while 75% of the nonconcussed control players with an MSK injury sustained 1 singular injury in the 90-day period (P = .971). No significant differences were noted between the percentage of players that sustained multiple injuries in the 90-day post-RTP period (P > .05). The location of injury was overall statistically similar between the concussed and control cohorts (P >.05). However, the control cohort had a statistically significant greater percentage of hand/wrist injuries (16%) compared with the concussed cohorts (2%) (P = .036). Ankle injuries were the most common injury for both the concussed and control cohorts (20% and 33%, respectively). In addition, no significant differences were noted between the injury types (P > .05). RTP after the MSK injury was similar between both cohorts, with respect to the mean number of games missed, days missed, and season-ending injuries (P > .05).
MSK Injury Characteristics for Concussed NBA Athletes and Matched Control NBA Athletes a
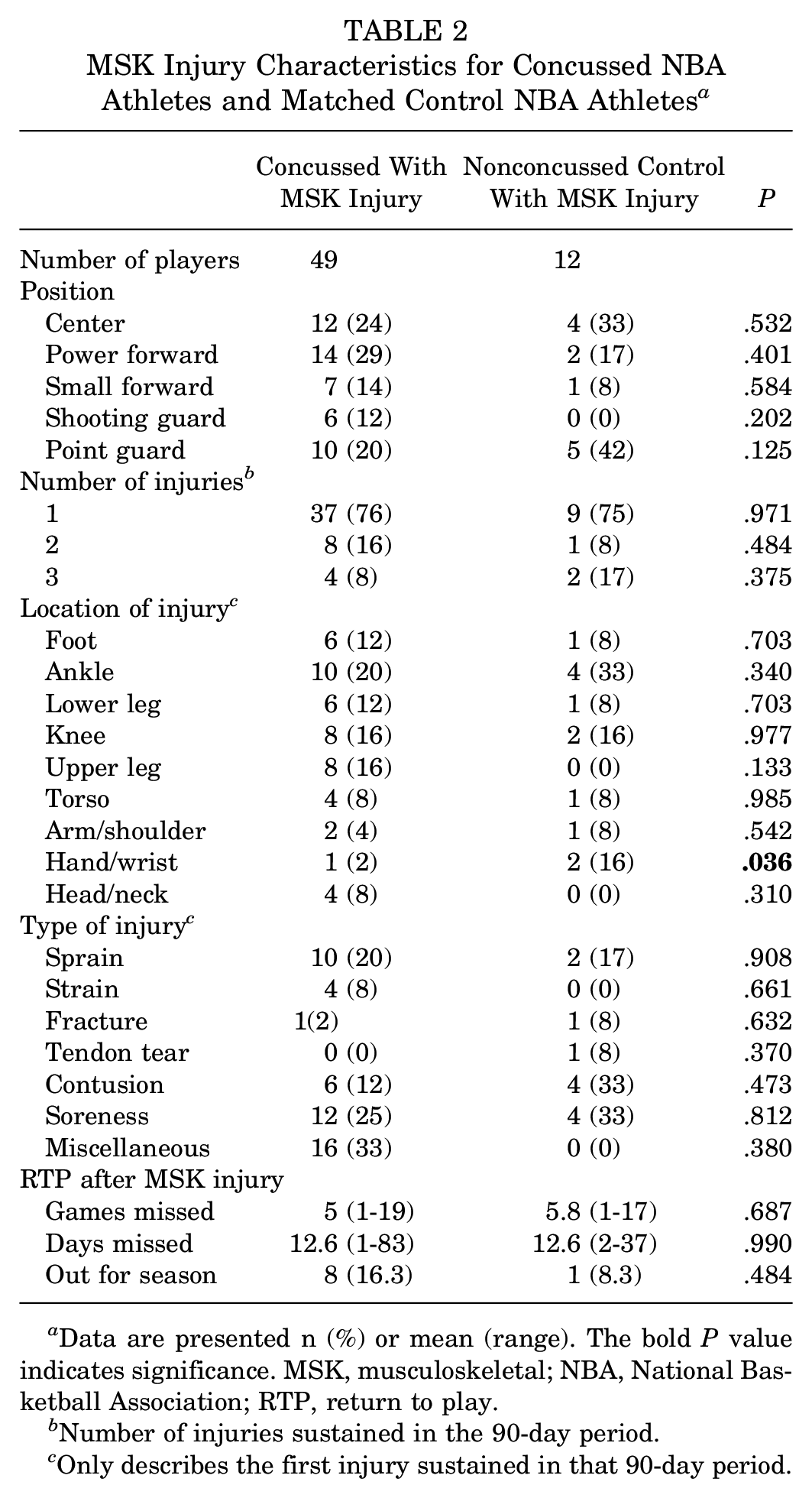
Data are presented n (%) or mean (range). The bold P value indicates significance. MSK, musculoskeletal; NBA, National Basketball Association; RTP, return to play.
Number of injuries sustained in the 90-day period.
Only describes the first injury sustained in that 90-day period.
Performance Statistic Analysis in Concussed Players Without MSK Injury
Table 3 demonstrates the analysis of performance statistics of concussed players in the woMSKi subgroup. In concussed players without a subsequent MSK injury, no significant differences were found in TS% between the preindex season and postindex season 1 (0.541 ± 0.0164 vs 0.567 ± 0.0118; P = .136) (Table 3). Similar results were seen for MPG, PPG, and TS% between preindex season and postindex season 1. Furthermore, no significant differences were found in TS% over the 90-day post-RTP period, at the 2-week point (0.962 ± 0.411), and the 3-month mark (0.569 ± 0.0173) (P = .358) after concussion (Table 4). No significant differences were noted for MPG and PPG across the 90-day period.
Player Performance Before and After Concussion in Those Without MSK Injury a

Values are presented as mean ± standard error of the mean. MPG, minutes per game; MSK, musculoskeletal; PPG, points per game, RTP, return to play; TS%, true shooting percentage.
Change from 2 weeks after RTP to 3 months after RTP.
Player Performance During 90 Days From Concussion After RTP in Those Without MSK Injury a

Values are reported as mean ± standard error of the mean. MPG, minutes per game; MSK, musculoskeletal; PPG, points per game, RTP, return to play; TS%, true shooting percentage.
Change from 2 weeks after RTP to 3 months after RTP.
Comparison of Performance Statistics between Concussed Players and Controls
Table 5 demonstrates the comparison of performance statistics between concussed and control players in the woMSKi cohort. Changes in player performance statistics of the concussed players without subsequent MSK injuries were compared with matched controls (Table 5). When comparing the changes in TS% across preindex season and postindex season 1, the concussed (0.026 ± 0.0185) and control groups (–0.0178 ± 0.0229) did not demonstrate statistically significant differences (P = .132). When comparing the changes in TS% across the 90-day post-RTP period, the concussed (–0.393 ± 0.412) and control groups (–0.0493 ± 0.0132) did not demonstrate statistically significant differences (P = .412). No significant differences between cohorts were identified for MPG and PPG for changes between seasons and changes over the 90-day period.
Player Performance After Concussion Compared With Matched Controls in Those Without MSK Injury a

Values are reported as mean ± standard error of the mean. MPG, minutes per game; MSK, musculoskeletal; PPG, points per game, RTP, return to play; TS%, true shooting percentage.
Change for the 90-day period: change from 2 weeks after RTP to 3 months after RTP.
Discussion
Main Findings
The primary finding of this study was that professional basketball players who sustained a concussion were 11.3 times more likely to sustain an MSK injury within the 90 days immediately after RTP compared with a control cohort (95% CI, 5.04-25.2; P < .001). Time missed after subsequent MSK injury was similar between the concussed (5 games) and control (5.8 games) cohorts (P = .687). Most of the concussed players sustained only 1 MSK injury in the 90-day period, and this was not statistically significantly different from the number of injuries seen in the control cohort (P = .971). Furthermore, there were no significant changes in the PPG, MPG, or TS% of concussed players without an MSK injury over the 90 days after RTP after concussion comparing their statistics or when compared with matched controls (P > .05).
Increased MSK Injury Risk
To our knowledge, this is the first study to examine the MSK injury risk of the entire body in a 90-day post-RTP from concussion period in NBA athletes. Of the 70 players who sustained a concussion, 70% of them experienced a subsequent MSK injury within this period. Previous studies have reported similar findings, such as Roach et al 35 who conducted a prospective study over 3 years in a military academy and followed each individual who sustained a concussion for 12 months. They found that those with concussions were 2.25 times more likely to sustain an upper extremity injury within the first year after a concussion, compared with controls. 35 Similarly, Baker et al 1 retrospectively reviewed National Football League injury reports from 2016 to 2020 and included all players with single concussions, multiple concussions, and a matched control group. They determined that the odds of sustaining a lower extremity injury in players with multiple or single concussions were significantly greater when compared with those without concussions (odds ratio, 2.92). Recently, similar research studies have been published using the NBA athlete population. Jildeh et al 20 found that concussed NBA players are 4.69 times more likely to sustain a lower extremity injury in the 90 days after a concussion compared with a matched cohort. In the present study, a separate analysis was completed to determine the rate of sustaining a lower extremity injury in concussed NBA athletes; there was a 9.2 times greater risk compared with controls (54% vs 11% [95% CI, 3.84-22]; P < .001). These results in the context of other literature suggest that regardless of the contact level of the sport, concussions put athletes at a higher risk for subsequent injuries.
Further, concussed players with a subsequent MSK injury had a mean interval of 41.39 days between concussion and MSK injury and a mean of 34.29 days between RTP and the MSK injury. These findings indicate that subsequent injuries are most likely to occur in the first half of the 90-day period. However, Jildeh et al 19 conducted a meta-analysis on 13 studies investigating lower extremity injury after RTP from a concussion and found that 4 of them demonstrated an increased risk within 90 days, while 6 of them demonstrated an increased risk within 1 year. Specific to upper extremity injury, Gardner et al 12 found that all postconcussion upper extremity injuries in collegiate football players occurred within 1 year of the concussion. Thus, there is not a strong consensus on how long the neurologic effects after concussion may affect injury risk. However, most recent literature seems to highlight the 90-day period as the most pronounced in terms of neurologic impact.4,5,15,29 For instance, a study by McCrea et al 29 conducted a prospective cohort study of 79 collegiate football players who sustained a concussion and followed them for 90 days. After 90 days, all postconcussive symptoms, cognitive functioning testing, and postural stability scores were normal. Another study by Howell et al 16 found that athletes with a history of concussions exhibited shorter stride lengths during dual-task assessments as well as decreased cognitive tasks; the assessments were performed 8.6 to 10.7 days after the concussion. These study time frames suggest that the 90-day period is the time interval where an MSK injury may be most influenced by the neurologic effects from a previous concussion such as postural instability, cognitive impairment, and compromised gait patterns. An injury may be more likely to be caused by other factors after 90 days. Ultimately, in a sport like professional basketball, where players rely on optimal stability and cognitive function, the 90-day effects from concussions can have serious impacts on player safety. In the present study, 8 out of the 49 concussed players sustained an MSK injury that ended their season.
No Change in Performance Statistics
To our knowledge, this is the first study that investigated performance statistics across the 90 days post-RTP from concussion. This study found no significant changes in concussed players’ performance statistics over the 90 days or across seasons. Also, no differences were seen in these changes when compared with control players. DeFroda et al 9 conducted a study of concussed NBA players to investigate PER, games started, games played, and minutes played in the season before the injury and the 2 seasons after. They found no significant changes in PER across seasons, which is consistent with the present study’s findings in a more acute period. However, as discussed earlier, the effects of concussion may be very minimal 1 to 2 years after the concussion. Therefore, the present study included the analysis of the 90-day period to assess any impact on performance that may be more attributable to the concussion itself, and no other factors. Patel et al 33 discovered no difference in NBA player performance statistics when investigating a shorter period of 10 days before compared with 10 days after the concussion, which is consistent with the present study’s findings as well. Similar results are demonstrated in other professional sports as well—such as hockey and soccer.7,22 Specifically with respect to professional football, previous research has shown no significant performance deficits upon RTP from concussion.34,38
Limitations
There are various limitations to note in this study. This was a retrospective chart review of injury data compiled from a public database and verified using various media sources. Although these methods were used in numerous other studies, there could be some inaccurate information, as the official medical records of these players were not accessed. Because these records could not be accessed, there was no additional information that could have been controlled for—including players’ concussion history, amount of time since the previous concussion, recent MSK injury information—and other variables that could have impacted subsequent time loss or risk of MSK injury. Nonetheless, the NBA requires that injury data for their players be reported each game day to the press releases and other media sources, which is where the data were queried from. The nonspecific nature of injury reporting to the public prevented specific diagnoses, such as meniscal or labral tears, from being analyzed in this study. These data could have allowed more descriptive epidemiological reporting of the resultant pathologies, a greater inclination to distinguish noncontact and contact injuries and a discussion of the prevalence of common injuries associated with neurological consequences after concussion. Furthermore, this study did not include any players who sustained a concussion at the end of the season due to the absence of off-season injury data. Any concussions that were sustained in practice, workouts, and offseason play were not recorded. Also, because concussions are partly diagnosed with self-reported symptoms from the players, there may have been players who did not mention symptoms to their medical staff, as this has historically occurred in all sports. These factors could have led to underreporting of concussions and subsequent risk of MSK injury.
Conclusion
Our analysis demonstrates that basketball players who sustain concussions are at a significantly increased risk for subsequent MSK injury within the 90-day post-RTP period but not player performance. Knowledge of this increased risk of MSK injury in concussed athletes can help guide concussion management for proper RTP and targeted rehabilitation in professional basketball players.
Footnotes
Final revision submitted August 8, 2024; accepted September 6, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.V.T. and J.H. have received support for education from ImpactOrtho and hospitality payments from Stryker Corp. A.C. has received consulting fees from Arthrex, Zimmer Biomet, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Mayo Clinic (ref No. 21-009369).