
Abstract
Background:
Patients routinely undergo computed tomography (CT) before arthroscopy for femoroacetabular impingement as part of preoperative planning. These scans include the lower lumbar spine, entire pelvis, proximal femur, knees, and ankles, raising questions about the prevalence and clinical impact of incidental findings (IFs) from these images.
Purpose:
To evaluate factors associated with IFs, as well as their prevalence, management, and impact on patient outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a retrospective review of preoperative pelvic CT scans from a single surgeon’s hip outcomes registry. Additional details regarding specific participants were obtained through electronic medical records. Logistic regression analysis was used to compare the effects of predictors of interest on the likelihood of having an IF on CT imaging. Repeated-measures mixed modeling was utilized to examine the effect of IFs on patient-reported outcomes obtained at 6 weeks, 3 months, 6 months, 1 year, and 2 years postoperatively.
Results:
A total of 714 preoperative CT reports in 596 patients were reviewed; IFs were present in 306 of the scans (42.9%). Most IFs were of skeletal pathology (78.1%), followed by soft tissue (7.8%), reproductive (6.9%), abdominal (4.2%), and urologic (2.9%). Of the 306 IFs, 10 (3.3%) required further medical workup. Multivariate analysis indicated that patient factors associated with an IF included age (P < .0001). Presence of an IF on preoperative imaging was associated with lower values both pre- and postoperatively on the Hip Outcome Score activities of daily living (P = .04) and sports-specific subscale (P = .03), the 12-item International Hip Outcome Tool (P = .02), and the Patient-Reported Outcomes Measurement Information System–Mobility measure (P = .03). Although statistically significant, these findings did not exceed the minimal clinical important difference (MCID) for these scores.
Conclusion:
The presence of IFs on CT imaging was associated with significant decreases across multiple outcome scores; however, the differences in scores did not exceed the MCID for any outcome. The high prevalence of IFs necessitates implementation of a reliable standardized follow-up protocol. This could improve overall patient care by reassuring patients of benign findings or providing treatment for potentially harmful ones.
Hip arthroscopy has become an increasingly common procedure in the treatment of hip disease over the past decade. A recent retrospective comparative study of over 400 hospitals participating in the National Surgical Quality Improvement Program in the United States showed a 25-fold increase in hip arthroscopy from 2006 to 2013. 9 As the field of hip preservation continues to advance, the prevalence of imaging for surgical planning is expected to rise. Preoperative computed tomography (CT) scans include the lower lumbar spine, entire pelvis, proximal femur, knees, and ankles. The use of CT for femoroacetabular impingement has been linked to decreased rates of revision hip arthroscopy, 3 and CT imaging can better characterize morphologic bony abnormalities to be addressed by hip arthroscopy.5,12,14,25,30 The osseous anatomy and localization of impingement lesions provided by CT scanning helps to avoid inadequate resections during hip arthroscopy and improve overall patient satisfaction.3,12,20,31 Additionally, CT allows for more accurate control of patient position when assessing femoral version and acetabular version when compared with plain radiographs. 14 However, as the use of CT before planned hip arthroscopy continues to expand, incidental findings (IFs) may become an impedance to patient care and satisfaction.
The rate of IFs on preoperative CT imaging has increased in the past several decades 28 and has been reported to be as high as 39.8% on all imaging modalities. 27 Despite this finding, a paucity of literature about IFs exists. Most studies have focused on IFs on CT chest imaging before planned total shoulder arthroplasty.8,23 Additional studies in the field of orthopaedics have been limited to plain radiographs34,41 and staging radiographic studies obtained in the setting of soft tissue sarcomas. 24 Several studies have examined IFs found on preoperative CT before elective hip and knee arthroplasty.13,40 Hassebrock et al 13 found a higher incidence of musculoskeletal and nonmusculoskeletal IFs on CTs before elective total hip arthroplasty (THA) when compared with preoperative imaging obtained before total knee arthroplasty. Additionally, the authors found that >45.7% of patients had ≥1 IF identified at the time of preoperative imaging. In a study by Tran et al, 40 significant IFs requiring further treatment were more likely to be identified on CTs before THA, with a delay or cancellation in surgery more likely to occur in these patients. These delays and/or cancellations can cause significant patient anxiety and can lead to “cascades of care” that cause significant harm. 10
Several known IFs that have been studied in patients undergoing hip arthroscopy include sacroiliac joint arthritis, 15 lumbosacral spine pathology, 39 and symphysis pubis abnormalities. 19 By understanding the risk factors and common IFs found in this patient population, surgeons may better counsel their patients and provide more effective triaging to required medical services. Insight into IFs in a younger patient population will bring attention to a growing problem in orthopaedics.
The purpose of this study was to identify patient demographic characteristics that may lead to a higher risk of IF identification on pre-operative CT before elective hip arthroscopy. Secondary objectives included characterizing common IFs among this patient population, identifying the rate at which these IFs lead to a delay in surgery and describing the effects that IF identification has on patient outcomes. We hypothesized that patients with any IF on preoperative CT imaging would have inferior clinical outcomes when compared with patients with no identified IFs.
Methods
Study Design
We conducted a retrospective chart review via a prospectively collected hip preservation registry to identify patients who underwent elective hip arthroscopy by a single surgeon (A.M.S.) at a single institution between 2017 and 2022. Patients who had obtained preoperative CT imaging were prioritized. Exclusion criteria were patients who underwent revision hip arthroscopy as well as those who underwent hip arthroscopy for trauma, septic arthritis, or other nonelective etiologies. Patients who did not undergo preoperative CT imaging before their procedure were also excluded. Demographic, preoperative, and postoperative follow-up data were obtained from the patients’ electronic medical record. This study was determined to be exempt from human participants' research approval by our institutional review board.
CT Imaging
All CT imaging was performed using a low-dose CT protocol developed for evaluation of hip joint morphology and measurement of femoral and tibial torsion and to meet requirements for the Stryker HipMap 3D protocol. 37 CT scans were obtained of the pelvis, knees, and ankles at 120 kV and 150 mA (manual) using a large field of view. CT scans of the pelvis were obtained from the iliac crests to 6 cm below the lesser trochanters and reconstructed at a 0.625-mm slice thickness and 0.625 mm interval. CT scans of the knees were obtained from just above the femoral epicondyles to just inferior to the head of the fibula and reconstructed at a 2.5-mm slice thickness and 2.5-mm interval. CT of the ankles was obtained from just above the syndesmoses to the talar domes and reconstructed at a 2.5-mm slice thickness and 2.5-mm interval. Adaptive statistical iterative reconstruction techniques were used to improve image quality for soft tissue windows.
Data Collection
Demographic data including age at the time of surgery, sex assigned at birth, body mass index (BMI), smoking status, and comorbidities were recorded from the medical record for each patient. The final CT report as read by the attending musculoskeletal radiologist was reviewed in all patients for IFs, defined as any radiologist-reported CT finding other than those associated with pathology of femoroacetabular impingement being treated with hip arthroscopy. IFs were categorized based on their relation to specific organs within the body. Once categorized, these findings were grouped into common IFs unique to that specific section of the body. IFs that required further diagnostic evaluation or therapy were subclassified as “actionable.” Specifically, IFs were deemed actionable if they led to further imaging, laboratory workup, follow-up with another health care provider (physician or physician extender), or procedural intervention (biopsy or surgery). Actions that led to a delay in surgery were also recorded.
Patient-reported outcome measures (PROMs) were obtained via a prospectively collected hip preservation registry. Data were recorded from the patient’s initial preoperative clinical visit and at 6 weeks, 3 months, 6 months, 1 year, and 2 years postoperatively. PROMs of interest included the Hip Outcome Score (HOS) activities of daily living (ADL) and sport-specific subscale (SSS), the 12-item International Hip Outcome Tool (iHOT-12), and the Patient-Reported Outcomes Measurement Information System–Mobility measure (PROMIS–Mobility). In addition, we further evaluated whether the presence of an IF led to differences that exceeded the minimal clinically important difference (MCID) for the HOS, 16 iHOT-12, 26 and PROMIS. 2 The Patient Health Questionnaire–9 (PHQ-9) survey for depression and the Generalized Anxiety Disorder–7 (GAD-7) survey for anxiety were also completed by patients. Patients with missing values for PROMs completed during certain follow-up visits were included in the final analysis.
Statistical Analysis
Descriptive statistics were compiled in the form of frequencies and means. Logistic regression was used to compare the effects of different predictors of interest on the likelihood of having an IF. The chi-square test of association and t test were used to evaluate the relationships between each predictor and IF. Finally, repeated-measures mixed modeling was used to analyze the effect of IF presence on PROM scores preoperatively and over the 5 postoperative follow-up periods. For all statistical analysis, a P value of <.05 was considered statistically significant.
Results
Patient Characteristics
Included were 596 patients who underwent 714 hip arthroscopy procedures with preoperative CT imaging. In patients who underwent bilateral hip arthroscopy procedures, each hip was included as a separate data point. The mean time from preoperative CT scan to surgery was 79.0 ± 116.5 days. There were scans of 274 male (38.4%) and 440 (61.6%) female hips, with a mean age of 30.5 ± 11.1 years. Mean BMI was 25.3 ± 4.6 kg/m2. Complete demographic characteristics for the study cohort are displayed in Table 1.
Characteristics of the Study Population (N = 596 patients, 714 hip CT scans) a

Data are presented as mean ± SD or No. of hips (%) unless otherwise indicated. CT, computed tomography.
Data are presented as No. of hips (% of hips within the group).
IFs on CT Imaging
Of the 714 preoperative hip CT scans, 306 (42.9%) were found to have an IF, and 31 of 714 scans (4.3%) were found to have >1 IF. Skeletal IFs were the most common and accounted for 239 of 306 (78.1%) IFs. The most common skeletal IF was spinal pathology (degenerative disc disease, pars defects, disc herniations, etc), followed closely by sacroiliac osteoarthritis. Soft tissue IFs were found in 24 of 306 images (7.8%), the most common of which was muscular pathology such as atrophy, calcification, and enthesophytes. There were reproductive IFs on 21 of 306 images (6.9%); these primarily consisted of adnexal calcifications/cysts. A complete summary of the IFs can be found in Table 2.
Summary of IFs on CT Imaging (N = 306 IFs) a

Data are presented as No. of CT scans, with data in parentheses representing percentage of total IFs. CT, computed tomography; DDD, degenerative disc disease; IF, incidental finding; OA, osteoarthritis.
Further action (other than patient and primary care provider notification of the findings by the surgical team) was pursued on 10 of the 306 (3.3%) IFs found on preoperative CT scans. No delays in surgery were reported in IFs requiring further action. Many of the IFs that led to further action were reproductive findings; there were radiographic findings concerning for adnexal pathology in 5 of 10 (50.0%) actionable IFs.
Follow-up to further diagnose or treat IFs was completed by a patient’s primary care physician or other medical specialist. A total of 3 of 10 (30.0%) actionable IFs required follow-up with a personal care provider, and 3 of 10 (30.0%) required follow-up with an obstetrician/gynecologist. The most common diagnostic test ordered for actionable IFs was a dedicated ultrasound in 5 of 10 (50.0%) cases, followed by right femoral plain radiographs (10.0%) and lumbar magnetic resonance imaging (MRI; 10.0%). Two of the 10 (20.0%) patients with an actionable IF required a procedure, 1 for removal of an atypical positioning of an intrauterine device and the other for an L5-S1 bilateral facet injection.
Results of Logistic Regression Analysis
On multivariate analysis, patient age was associated with a greater odds of identification of an IF on preoperative CT scan (odds ratio = 1.059; P < .0001). Unfortunately, pack-year data were unavailable in the patient record. Patient sex was not associated with odds of identification of an IF, nor was current or former smoking status. A complete summary of the results of the multivariate analysis can be found in Table 3.
Patient Characteristics Associated With Incidental Findings a
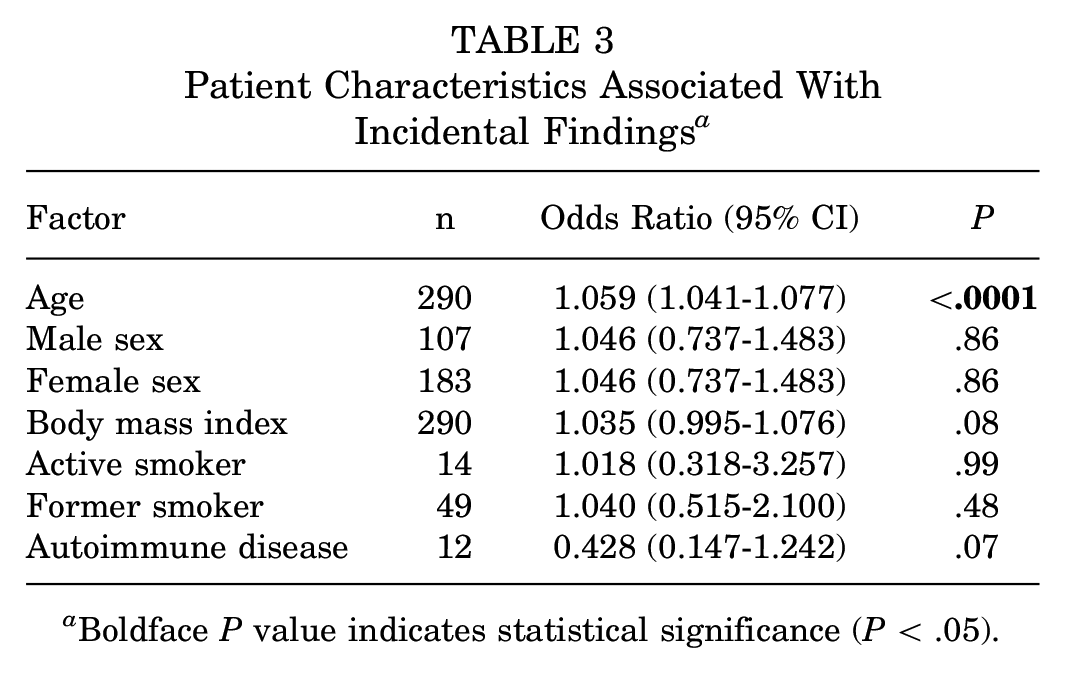
Boldface P value indicates statistical significance (P < .05).
Repeated-Measures Mixed Modeling
The least squares means method was used to create outcome estimates for PROM scores preoperatively and at 6 weeks, 3 months, 6 months, 1 year, and 2 years postoperatively, stratified by presence of an IF (Figure 1). Results showed that the presence of an IF on preoperative CT imaging was associated with lower values both pre- and postoperatively for HOS-ADL (P = .04), HOS-SSS (P = .03), iHOT-12 (P = .02) and PROMIS–Mobility (P = .03). However, these findings did not exceed the MCID for these scores. No association was found between positive identification of an IF and the PHQ-9 (for depression) or the GAD-7 (for anxiety) up to 2 years postoperatively. The results of these findings are summarized in Table 4.

Effect of IFs on patient-reported outcome scores. The least squares means method was used to create outcome estimates for preoperative through 2 years postoperative. ADL, activities of daily living; CT, computed tomography; HOS, Hip Outcome Score; IF, incidental finding; iHOT-12, 12-item International Hip Outcome Tool ; PROMIS–Mobility, Patient-Reported Outcomes Measurement Information System–Mobility measure; SSS, sport-specific subscale.
Effect of Incidental Findings on Patient-Reported Outcome Measures a

Boldface P values indicate statistical significance (P < .05). ADL, activities of daily living; GAD, Generalized Anxiety Disorder; HOS, Hip Outcome Score; iHOT, 12-item International Hip Outcome Tool ; PHQ, Patient Health Questionnaire; PROMIS, Patient-Reported Outcomes Measurement Information System; SSS, sport-specific subscale.
1321 of 2520 total values missing.
1284 of 2520 total values missing.
1344 of 2520 total values missing.
1732 of 2520 total values missing.
1756 of 2520 total values missing.
1756 of 2520 total values missing.
Discussion
There are limited data regarding management and risk factors for IFs found in preoperative imaging before elective procedures and currently no studies examining IFs found before hip arthroscopy. Additionally, there are currently no studies within the orthopaedic literature examining the postoperative outcomes related to IFs. This study found that increased age was associated with positive identification of an IF preoperatively in multivariate analysis. In addition, significantly lower values in several patient-reported outcome tools (HOS-ADL, HOS-SSS, iHOT-13, PROMIS–Mobility) were found in patients with the presence of an IF on preoperative imaging, although the differences did not exceed the MCID. These findings begin to provide a better understanding of the risks associated with preoperative imaging as well as the consequences of IFs in the treatment of patients.
Increased age was found to be associated with positive identification of an IF preoperatively in this study. Prior studies within orthopaedic literature examining IFs focus primarily on those patients undergoing total joint replacement.8,13,23,41 Reported prevalence of IFs within these studies ranged from 22.8% to 51.7%, which is similar to the findings of this study with 42.9% of images confirmed to have ≥1 IF. However, the patient population of these studies differs greatly from the population examined presently. Additionally, the patient population in these studies likely had a smaller field imaged than those patients included in this study. Hassebrock et al 13 and Tran et al 40 specifically reviewed imaging results of those patients undergoing elective THA or total knee arthroplasty. The mean age of patients in the studies were 65.6 and 65 years, respectively, while the mean age at surgery of the patients in the current study was 30.5 years. Other studies have reported similar patient ages, with all studies having mean patient ages of >50 years.13,23,24,40 Although we found a similar prevalence of IFs in the observed patient population, the acuity of these findings differs from those found in the other studies. Only 10 of 306 IFs (3.3%) required action, and none of these resulted in surgical delays. In comparison, Tran et al reported 5.5% of all IFs identified within the study required further action with 8 of the 41 patients (19.5%) with significant findings requiring delay in surgery. Chen et al 8 found even higher rates of IFs requiring additional clinical work-up in patients undergoing preoperative CT before planned total shoulder arthroplasty with 11.4% of images containing potentially pathologic IFs. Other studies have found low rates of actionable IFs. However, one of the studies was limited to identification of pulmonary nodules only in chest CT imaging before total shoulder arthroplasty 23 and the other did not evaluate actions beyond further imaging. 13 These findings suggest that although the prevalence of IFs is similar among all ages undergoing preoperative CT imaging before elective procedures, the severity of IFs increases in an older patient population. Several studies published in trauma literature have also examined IFs found in whole-body CT scans obtained to evaluate for injury, and all have found age to be associated with a higher prevalence of Ifs.22,29,33 In addition, Liu et al 22 reported increased age to be predictive of identifying an IF that required further management. These findings suggest that older patients receiving preoperative imaging before elective hip arthroscopy should be further counseled or administered informational pamphlets regarding the possibility of IFs.
To our knowledge, this is the first study to examine the relationship between PROMs and IFs. We identified the HOS-ADL and HOS-SSS, the iHOT-12, and PROMIS–Mobility measure as being affected by positive identification of an IF. It is likely that our findings regarding increased age being associated with an IF are related to worse PROM scores. Wolfson et al 43 found age ≥40 years to be associated with lower rates of reaching the MCID and Patient Acceptable Symptom State after hip arthroscopy, while similar studies have found younger patients to more likely achieve positive outcomes after surgery. 36 Numerous studies have additionally shown older patients to be more likely to convert to THA after hip arthroscopy.1,17 Many IFs found within this study were related to osteoarthritis of neighboring joints including the pubic symphysis, sacroiliac, and facet joints of the spine. Krishnamoorthy et al 19 found in a matched-cohort analysis that degeneration of the sacroiliac joint was associated with lower PROM scores in patients undergoing hip arthroscopy. Additionally in a retrospective matched cohort study with minimum 24-month follow up, Horner et al 15 and Torabian et al 39 examined sacroiliac joint and lumbosacral pathology, respectively, in patients undergoing elective hip arthroscopy and found inferior PROM scores in patients with pathology. However, each study reported similar clinical benefits when compared with patients who underwent hip arthroscopy with no preoperative pathology. Although we did not specifically examine each IF individually, we found that identification of an IF had an effect on PROMs following hip arthroscopy, though these differences did not exceed the MCID. These studies highlight the need for further evaluation of the relationship between IFs and PROMs.
Surprisingly, we also found no relationship between identification of an IF and postoperative PHQ-9 and GAD-7 scores in patients. Previous literature has shown a negative effect of IFs on a patient’s overall anxiety after imaging.6,18,21,35,42 A cross-sectional study examining IFs after whole-body MRI screening found that 28.6% of patients with an IF reported moderate to severe distress after being alerted to the finding. 32 Bomhof et al 4 described similar results in an interview study on research participants receiving brain imaging who were found to have IFs. They went on to describe a larger impact of IFs on family members and a participant’s social environment. A key difference between our study and those presented previously is the severity of IFs found. Many of the IFs identified in this study were relatively benign, such as osteoarthritis of an adjacent joint. Comparatively, other studies in orthopaedic literature have found incidences of possible malignancies,8,13,23,26,40,41 vascular disease,6,23,40 and other pathology that may be life threatening. Although no direct relationship between mental health and IFs were found, both the iHOT-12 11 and the PROMIS 7 include a component of social and mental health. This highlights the need for further studies explicitly investigating the relationship between IFs and mental health.
Limitations
The present study is not without limitations. Although we found a statistically significant effect with positive identification of an IF on PROMs, the actual effect was small. Although this difference was statistically significant, the clinical effect is likely small. In addition, the patient population presented here was generally younger (<40 years) compared with similar studies in which patients received pelvic imaging before elective procedures.13,40 The nature of hip preservation surgery makes direct comparison of a young patient population with an elderly cohort difficult. Additionally, data analysis on the relationship between PROMs and positive identification of an IF may be confounded by other variables, such as age. We also acknowledge that not everyone receives a preoperative CT before elective surgery due to concern of increased radiation exposure. The CTs obtained at our facility utilize a low-dose radiation protocol, which has an advantage of obtaining femoral version and tibial torsion measurements. 38 However, this imaging protocol has a limited relevant field of volume when compared with traditional counterparts. In the current study, we did not differentiate between patients who received low-dose CT versus those who may have received traditional CT imaging at an outside institution and were referred. Last, this study included patients from a single surgeon at a tertiary-care facility in a specific geographic region, and the findings may not be generalizable to other hip preservation practices.
Conclusion
IFs on preoperative CT before elective hip arthroscopy were common in the current study. The IFs were associated with certain patient characteristics and statistically significant decreases across multiple PROMs. However, the clinical significance remains uncertain, as the differences in scores between those with IFs and those without did not exceed the MCID for any PROM. The high prevalence of IFs necessitates the implementation of a reliable, standardized follow-up protocol. This could improve overall patient care by reassuring patients of benign findings or providing treatment for potentially harmful ones.
Footnotes
Final revision submitted June 17, 2024; accepted June 24, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.M.S. has received consulting fees from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Wisconsin–Madison (reference No. 2022-0515).