
Abstract
Background:
Evaluating shoulder proprioception provides functional data that supplement imaging for the diagnosis/rehabilitation of rotator cuff injuries. There is a need for a system capable of establishing normal ranges for proprioceptive accuracy in healthy shoulders during unrestricted 3-dimensional motion.
Purpose:
To conduct passive joint position sense (JPS) testing in men and women with no history of shoulder injury using a novel testing system, identifying differences in proprioceptive accuracy based on sex, shoulder elevation, and crossbody position.
Study Design:
Controlled laboratory study.
Methods:
We recruited 20 (10 male and 10 female) healthy participants aged between 18 and 25 years for JPS testing. Participants used a single wrist-worn sensor, and our primary outcome was errors in position matching (first guiding a participant's dominant arm from a neutral starting position to a target position and then having participants independently return from the start position to the same target) across 12 targets comprised of all possible combinations of shoulder elevation angles (EAs) (30°, 60°, 90°, and 120°) and crossbody angles (CAs) (0°, 45°, and 90°). A linear mixed model was employed to evaluate sex- and position-based differences in JPS accuracy.
Results:
Position-matching accuracy increased in both males and females as target EAs increased from 30° to 120° (P < .001). The greatest EA position-matching accuracy in both sexes was observed at EAs of 90° and 120° (P < .0001). A change in the direction of error was observed in both males and females as target EAs increased from 90° to 120°, transitioning from positive (overshooting) to negative (undershooting) error (P < .005). A sex-based difference was observed at EAs of 60°, 90°, and 120° in the 90° CA plane, where females exhibited more negative CA matching error compared with males (P < .01).
Conclusion:
Proprioceptive accuracy increased in both sexes at higher shoulder elevations. In the 90° CA plane, females demonstrated greater CA undershoot than males.
Clinical Relevance:
While magnetic resonance imaging and ultrasound are effective tools for determining the size/age of rotator cuff tears, they do not provide functional prognostic insight for pain or mobility. Proprioceptive testing, as a functional metric based on free shoulder motion, may assist in clinically characterizing a patient's shoulder injury and rehabilitative success at multiple time points.
Proprioception—a term coined by Charles Sherrington 2 in 1906—refers to one's ability to sense body position and movement at both conscious and unconscious levels.38,41 This “sixth sense” is achieved through mechanoreceptors and other sensory complexes located in the skin, muscles, tendons, and ligaments, which relay spatial information about one's limbs to the cerebral cortex through clusters of afferent nerve fibers.7,31 Proprioception is essential for movement coordination, body posture control, motor learning, and stability in both static and dynamic activities.13,20,22 A continuous proprioceptive feedback loop enables humans to perform daily tasks that require spatial awareness without relying solely on visual input. As a basic example, the unconscious coordination required for ambulation relies in part on proprioceptive signaling.
Proprioception plays a particularly important role in the shoulder, where it helps mediate synchronization between the passive and active structures stabilizing the highly mobile glenohumeral joint.2,6,45 Studies suggest that glenohumeral musculoskeletal disorders, such as shoulder instability, are associated with impaired proprioception14,25 and that correction of shoulder injuries via interventions like arthroscopy can result in a postoperative improvement in proprioception. 45 Surgeries restoring tension in capsuloligamentous structures can improve proprioception by returning mechanoreceptors to a loaded state in which they can sense deformation.4,33 The well-established link between functional shoulder stability and unimpaired proprioception has led to increased interest in quantitative assessment of the sense, potentially as a benchmark for rehabilitative success. 9
A notable challenge in measuring proprioception is selecting the appropriate testing technique and apparatus. Various methods have been employed—including joint position reproduction, threshold to detection of passive motion, path of joint motion replication, and active movement extent discrimination apparatus tests—which can assess both active and passive, as well as path-dependent and path-independent forms of proprioception.2,20 The instrumentation used in proprioception studies encompasses motion analysis systems, 37 electronic goniometers, 25 isokinetic dynamometers, 19 and a range of custom laboratory-designed systems.24,32 The diversity of tools and methodologies used has raised concerns regarding the validity and reliability of testing protocols. 2 In addition, it has been observed that kinesthetic tests, which record movement, and position matching tests, which record static positions, do not correlate. This makes it challenging to compare studies assessing different forms of proprioception. 17
Studies evaluating shoulder proprioception are less common than those assessing other joints, primarily because of the complexity of the glenohumeral joint, which boasts 3 degrees of freedom (flexion/extension, abduction/adduction, and medial/lateral rotation). Unlike the more constrained hip joint, the shoulder's ball-and-socket structure prioritizes motion over stability, making it the most mobile joint in the body. Many studies on shoulder proprioception are confined to 2-dimensional planes of motion, characterizing shoulder movement by changes in a single angle.4,12,25,44 Research assessing shoulder proprioception in 3 dimensions with unrestricted movement remains relatively scarce,1,11,37 and validated testing systems that cover the full range of shoulder motion are only now beginning to emerge. Some of these systems incorporate virtual reality, 8 wearable exoskeletons, 15 and motion capture equipment. 27 A review of devices and methods used to measure shoulder proprioception showed that a passive testing protocol employing an isokinetic dynamometer remains the most reliable, 2 despite recent progress in the development of portable and low-cost setups. A gold-standard Biodex isokinetic dynamometer can cost upwards of US$40,000 while weighing several hundred pounds and requiring costly annual calibration. 35
The present study aimed to compare the shoulder proprioception of healthy men and women at different positions using a new testing system composed of a single wrist-worn sensor. Position-matching data were collected across 12 targets, covering a large portion of the shoulder's functional range of motion. Matching error—defined as the 2-angle difference between a subject's match attempt and original target position—was measured and evaluated for differences based on sex and target position, with the hypotheses that proprioceptive accuracy would improve at elevations exceeding 90° of flexion 37 and that no significant difference in matching error would be observed between both sexes.5,10 Ultimately, this study will advance our understanding of healthy shoulder proprioception in 3 dimensions and establish a new testing system offering portability, ease of use, and accessibility. Findings may be applied to future studies looking at injured shoulders and their potential proprioceptive impairment.
Methods
Study Participants
The study protocol received approval from our institution's internal review board and was conducted in full compliance with its guidelines; all study participants provided voluntary informed consent after receiving an explanation of the study's objectives and protocols. A total of 20 participants (10 males and 10 females aged 18-25 years; mean age, 21.4 ± 1.4 years) were recruited from a university campus. The participants had no known history of shoulder pain or injury.
Materials
A system for measuring shoulder position was developed using a package by Ambulatory Parkinson’s Disease Monitoring (APDM) Wearable Technologies paired with an in-house Matlab (MathWorks) script. An APDM Opal Version 1 sensor (dimensions, 54.9 × 40 × 14.3–mm; with a built-in accelerometer, gyroscope, magnetometer, and barometer; 128 Hz sampling rate) placed on the distal forearm transmitted orientation information in the form of quaternions to the APDM Motion Studio software. Real-time sensor orientation data were streamed into Matlab, where it was used to create a testing interface for live visual presentation of subject and target positions. This interface enabled the entry of target position coordinates, the careful guidance of the subject's arm to the target, and the recording of a subject's arm position during matching attempts. Quaternion values were employed to determine the shoulder position of study participants in 3 dimensions and calculate the position-matching error. To enhance the interpretability of shoulder position coordinate data, 3-dimensional positions were transformed into a combination of 2 angles—elevation angle (EA) and crossbody angle (CA) (Figure 1).

Shoulder position was described using a combination of elevation angle and crossbody angle, shown here for the right shoulder.
The accuracy of angle measurements recorded with the Opal sensor system was validated through optical motion capture testing using Qualisys Track Manager (QTM) software in conjunction with Qualisys Oqus cameras and reflective tracking markers. Twelve shoulder positions were synchronously recorded with both the Opal and QTM systems over 3 repeated trials, providing 36 data points for comparison (Table 1). The EA and CA values recorded simultaneously by both systems showed a mean absolute difference of 2.2°± 1.6° and 2.7°± 3.1°, respectively, remaining consistent between testing system reboots.
Comparison of CA and EA Values Recorded Synchronously by the Opal Sensor System Used in the Study and the Gold-Standard QTM Motion-Capture Testing System a

CA and EA values are shown for 36 positions (12 shoulder positions over 3 repeated trials). CA, crossbody angle; EA, elevation angle; QTM, Qualisys Track Manager.
Indicates the directional (positive/negative) difference in values (Opal – QTM).
Testing Procedure
Shoulder proprioception was assessed through passive joint position sense (JPS) matching tasks. Shoulder JPS testing measures a subject's accuracy in replicating glenohumeral angles. The testing protocol in this study involved guiding a participant's dominant arm from a neutral starting position to a target position and then asking the participant to independently return from the start position to the same target. All testing was conducted ipsilaterally on the participant's dominant arm.
A position-determining sensor was securely attached to the wrist of each participant with a Velcro strap. To eliminate visual inputs and ensure the assessment of isolated shoulder proprioception, participants were blindfolded and seated upright in an armless chair, with their feet flat on the ground and their backs fully against the chair. Their elbows were immobilized using a Velcro-secured brace extending from the middle of the biceps to the middle of the forearm, restricting elbow flexion/extension and greatly limiting pronation/supination. Participants were instructed to avoid thoracic movement and keep their thumb pointing straight up at the ceiling to ensure consistent pronation/supination at the proximal radioulnar joint across all trials.
All individual testing was conducted during a single, 1-hour test session in which 12 targets were repeatedly tested over 3 identical trials. Target positions encompassed all 12 combinations of 4 EAs (30°, 60°, 90°, and 120°) and 3 CAs (0°, 45°, and 90°) (Figure 2). Each trial followed the same testing sequence: all EAs were assessed from low to high at CAs of 0°, 45°, and 90°, in that order. We adopted a nonrandom, sequential testing order to evaluate whether any learning effect appeared from trial to trial.

A 2-dimensional plot demonstrating the 12 targets used for position match testing. CA, crossbody angle; EA, elevation angle.
After being seated, participants were instructed to maintain their arms straight down by their sides, which served as their neutral starting position between the position memory and position matching steps. The arm of each participant was guided to the target positions using the real-time data stream provided by the testing system interface (Figure 3).

Screen capture of the custom testing interface while running testing. One dot represents the live subject position; another dot represents a selected target position. A “MATCH” icon appears when both align, allowing for subject arm alignment during the learning stage of testing.
Upon reaching a target position, participants were verbally informed that they would be required to return to the same position, and they were given 5 seconds to take in the position without interference once their arm was released. Verbal commands were used to prompt participants to return to the start position and then replicate the target position they were just shown independently. Once participants verbally indicated that they had completed their matching attempt, the shoulder position was recorded in the testing interface. Participants were asked to return to the same neutral starting position before moving to the learning stage of the next target; the sensor was recalibrated at this position to account for any unwanted movement between trials.
Data Analysis
The position-matching error in EAs and CAs was defined as the 2-component difference between the target angle and the subject match-attempt angle. The error was calculated by subtracting the target EA and CA from the participant's EA and CA, respectively. This difference (measured in deg) quantified error in matching accuracy; a positive value indicated overshooting the target angle, while a negative value indicated undershooting it (Figure 4). The error for each participant was analyzed in 2 ways—as a mean of the 3 identical trials and individually for each trial. The dual approach allowed us to look for any potential learning effects or changes in performance, appearing as changes in the spread of data distributions between trials, as participants repeated the sequential target positions.

Matching error convention from the perspective of a right-handed participant.
A linear mixed model (LMM) was used to (1) examine changes in the EA matching error and the CA matching error, with increases in target EAs and CAs, and (2) to examine the differences in the EA matching error and the CA matching error at each target between male and female participants. The LMM included the following: fixed effects for EA, CA, and sex; the 2-way interaction terms (sex × EA, sex × CA, and EA × CA); the 3-way interaction term (sex × EA × CA); and random intercepts for participants and random slopes for EAs and CAs nested within participants. The LMM was chosen for the analytic method, as it allows appropriate handling of data structures associated with repeated measurements and maximizes the information from specimens with missing observations.
The primary outcome of this study was the position-matching error (ie, EA error and CA error). The power was estimated with the intent to detect a 2-standard deviation difference in error (1) between target positions (hypothesis 1) and (2) between males and females at each target (hypothesis 2), with a total sample size of 20 participants (10 males and 10 females) while accommodating the Bonferroni adjusted per-comparison alpha (P < .0083 for objective 1 and P < .0042 for objective 2) necessary to maintain an overall 2-tailed alpha of .05 across the comparisons examined. A Bonferroni adjustment was chosen for the power analysis because it is highly conservative, and the Holm test, which was used in all analyses, is based on the empirical P value attained at the time of data analysis, which was unavailable during the study design phase. Given these parameters, the study maintained at least 95% power for hypothesis 1 and 86.2% power for hypothesis 2.
The outcome distribution and model residuals were examined to determine the distribution and link function to be applied to the model. Classical sandwich estimation was used to further protect against possible model misspecification. Pairwise comparisons were conducted within the model via orthogonal contrasts. The Holm test was used to correct for multiple comparisons, maintaining a 2-tailed familywise alpha at .05. Adjusted P values and model-based means and 95% CIs are reported. An adjusted P < .05 was used to determine statistical significance. All analyses were conducted in SAS Version 9.4 (SAS Institute).
Results
Both male and female participants demonstrated an increase in EA position-matching accuracy on all CA planes as target EAs increased from 30° to 120° (Table 2). In both sexes, the EA position-matching error became decreasingly positive (reduction in overshoot) as target EAs increased from 30° to 90° and increasingly negative (increase in undershoot) as target EAs increased from 90° to 120° (Figure 5). In other words, at target EAs of <90°, participants tended to position their arms above the target position during matching attempts, and at target EAs of >90°, participants tended to position their arms below the target position during matching attempts. The observed effect of target EAs on the EA matching error did not differ according to sex (F (6, 5.88) = 1.76) (P = .105). Overall, the smallest EA matching error in both sexes occurred at targets with EAs of 90° and 120° (absolute error range, –2.9° to + 0.7°) across all CAs.
Estimated Marginal Means for EA Matching Error at Each Target for All Participants a

Data are presented as mean (95% CI). P values exclude sex. Bold P values indicate statistically significant differences (P < .05). CA, crossbody angle; EA, elevation angle.

EA matching error (averaged for each participant across 3 trials) associated with each target and stratified by sex. Box ranges are 75% quantile and 25% quantile of averaged data with the horizontal line within denoting the median, while whiskers are nonoutlier minimum and maximum values, with outliers defined as values outside of 1.5 times the interquartile range. The dashed horizontal line denotes zero error (exact EA match), while the vertical dashed lines indicate a change in target CA. Targets are listed in order of increasing EAs from 0° to 120° at CAs of 0°, 45°, and 90°. Note the consistent pattern of negative decrease in error as the EA increases for any given plane of the CA. CA, crossbody angle; EA, elevation angle.
No notable trend was observed in the CA position-matching error based on the target EA (Figure 6). In the individual targets where the CA matching error did differ based on the target EA, there were no sex-based differences (F(6, 5.88) = 0.73) (P = .625) (Table 3). The mean magnitude of the CA error was lower than the corresponding mean magnitude of the EA error at 6 of the 12 targets: EA30° CA0°, EA60° CA0°, EA30° CA45°, EA60° CA45°, EA30° CA90°, and EA60° CA90°. These targets are positioned below the plane of the 90° EA.
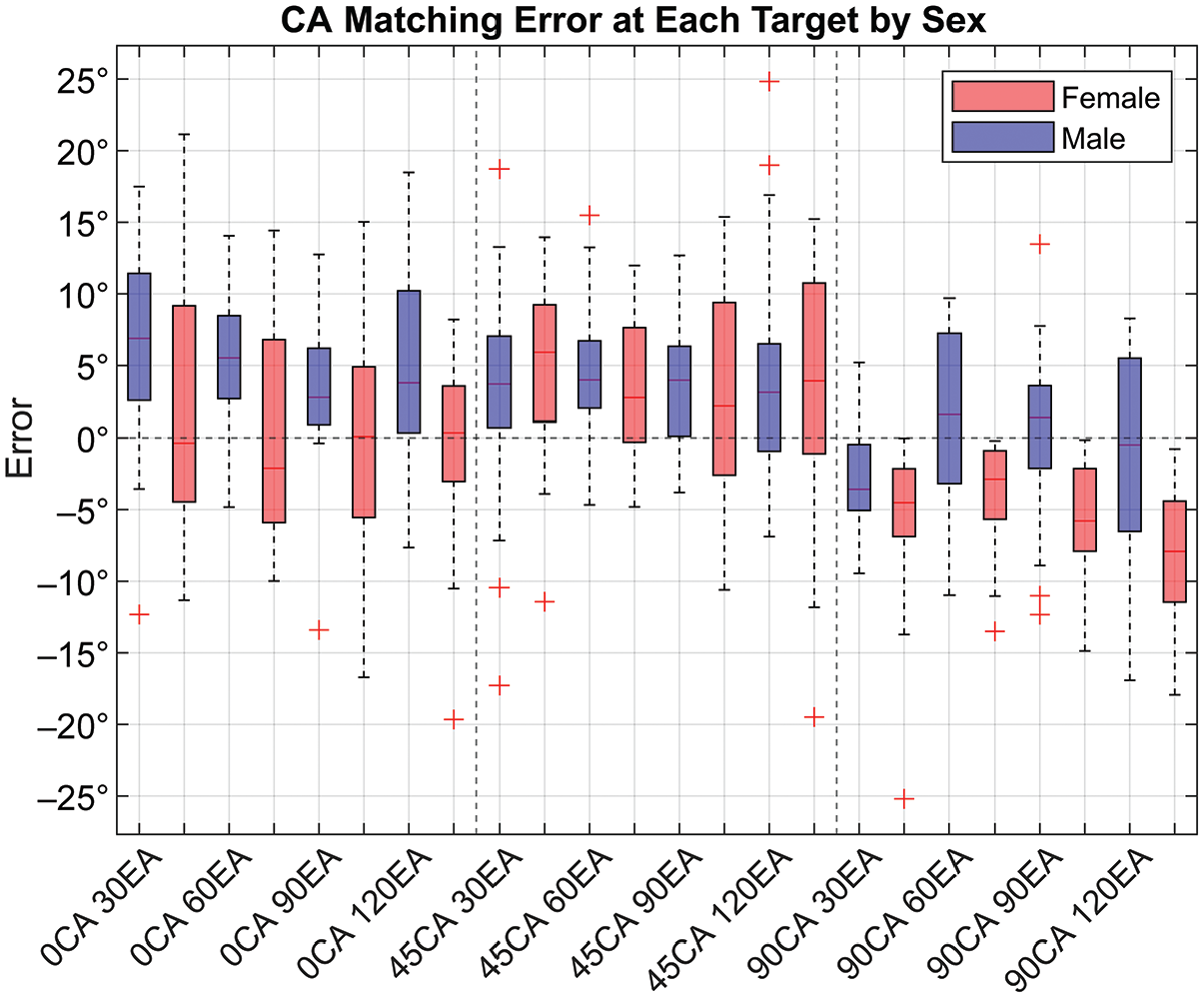
CA matching error (averaged for each participant across 3 trials) associated with each target and stratified by sex. Box ranges are 75% quantile and 25% quantile of averaged data with the horizontal line within denoting the median, while whiskers are nonoutlier minimum and maximum values, with outliers defined as values outside of 1.5 times the interquartile range. The dashed horizontal line denotes zero error (exact CA match), while the vertical dashed lines indicate a change in the target CA. Targets are listed in order of increasing EAs from 0° to 120° at CAs of 0°, 45°, and 90°. CA, crossbody angle; EA, elevation angle.
Estimated Marginal Means for CA Matching Error at Each Target for All Participants a
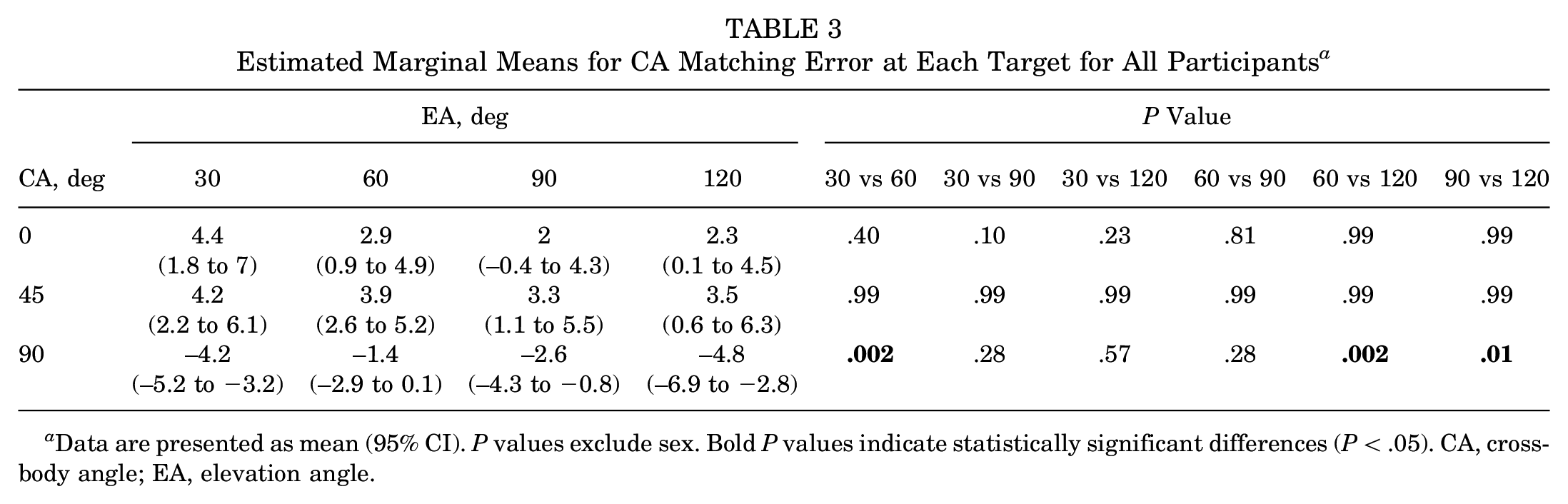
Data are presented as mean (95% CI). P values exclude sex. Bold P values indicate statistically significant differences (P < .05). CA, crossbody angle; EA, elevation angle.
There were no notable differences in EA matching error between males and females at any of the targets examined (Table 4). The CA matching error, however, differed between males and females at the following targets: (1) EA60° CA90°; (2) EA90° CA90°; and (3) EA120° CA90° (Table 4). At these targets, females tend to undershoot (negative error value) the CA more than males, as can be observed by rightward clustering of male data points (positive mean CA error, CA overshoot) and a leftward (negative mean CA error, CA undershoot) clustering of female data points (Figure 7).
Comparison of EA and CA Matching Error Between Males and Females at Each Target a

Data are presented as mean (95% CI). Bold P values indicate a statistically significant difference between males and females (P < .05). CA, crossbody angle; EA, elevation angle.
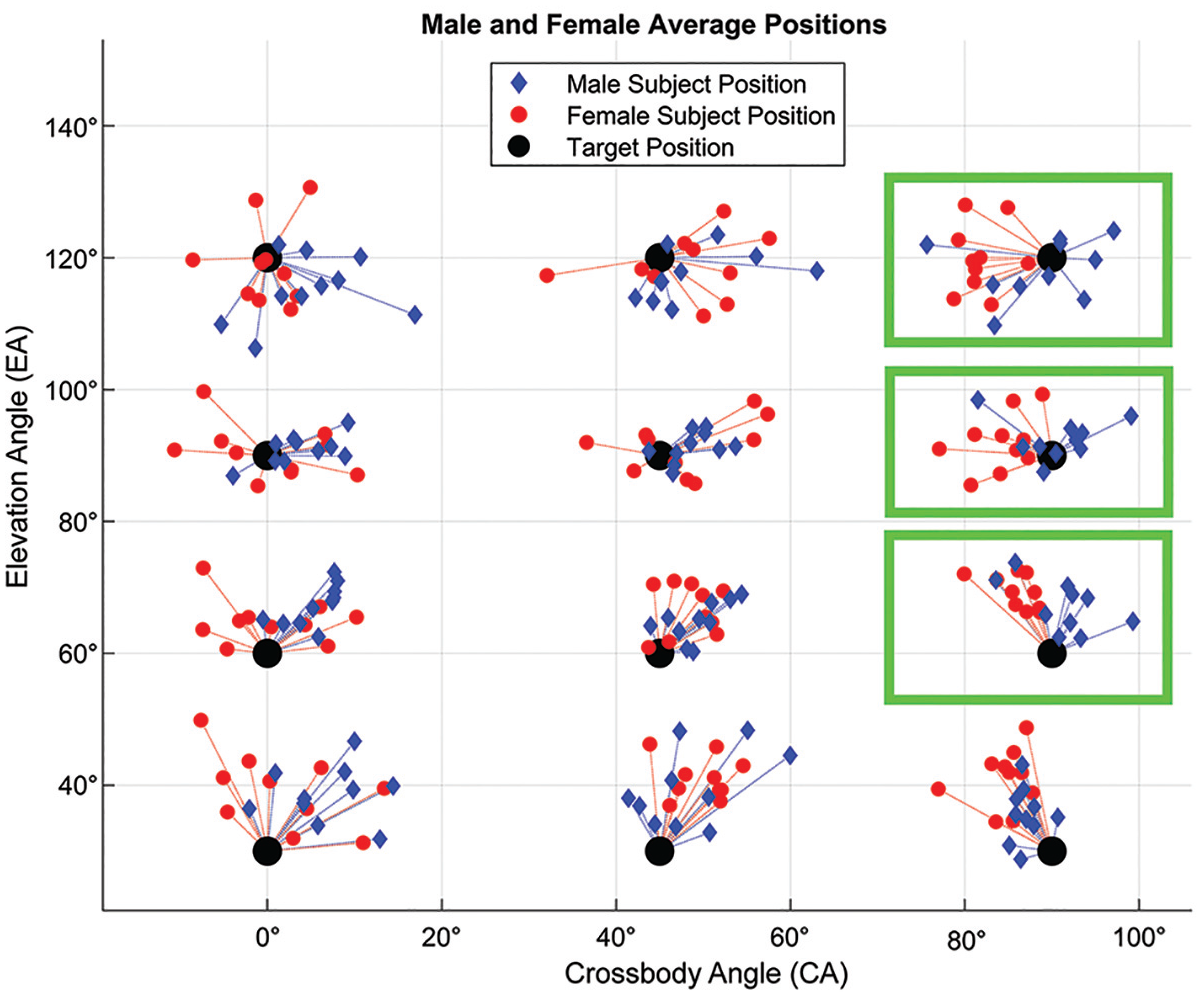
A CA vs EA scatter plot of male and female positions (mean of 3 trials). Target positions with statistically significant differences in the CA error between males and females are boxed in green. CA, crossbody angle; EA, elevation angle.
Visual analysis of CA and EA matching error distributions between individual trials did not indicate any learning effect resulting from target repetition. The interquartile ranges of the EA matching error (Figure 8A) and the CA matching error (Figure 8B) did not appear to systematically shrink or expand between trial 1, trial 2, and trial 3. Therefore, there was no evidence to suggest that subject performance was improving or worsening as the testing was repeated.

(A) EA matching error and (B) CA matching error (3 trials shown for each) associated with each position. Box ranges are 75% quantile and 25% quantile of each trial with the horizontal line within denoting the median, while whiskers are nonoutlier minimum and maximum values, with outliers defined as values outside of 1.5 times the interquartile range. The dashed horizontal line denotes zero error (exact EA or CA match), while the vertical dashed lines indicate a change in target EAs or CAs. Targets are listed in order of increasing EAs from 0° to 120° at CAs of 0°, 45°, and 90°. CA, crossbody angle; EA, elevation angle.
Discussion
This study aimed to introduce a novel testing system and employ it in studying the proprioception of healthy persons (N = 20, 10 males and 10 females), searching for differences in proprioceptive accuracy based on EA, CA, and sex. Our results from testing across 12 targets indicated that EA matching accuracy is influenced by target EA in both males and females. Both groups exhibited increased EA matching accuracy when tested at EAs of 90° and 120° compared with EAs of 30° and 60°. Within the higher elevation targets, the EA matching error differed between targets with EAs of 90° and 120° at all CAs, with the error changing from overshoot to undershoot from an EA of 90° to an EA of 120°. In the lower elevation targets, participants showed a significant difference in EA matching accuracy between targets with EAs of 30° and 60° in the 0° and 45° CA planes. While there was no trend in the CA matching error based on the target position EA in either sex, there was a pattern of smaller mean CA error magnitudes compared with corresponding EA error magnitude at target positions <90° EA in both sexes.
Three out of the 12 targets exhibited a difference in CA matching error between males and females. At these 3 targets, females consistently undershot the target CA, whereas males overshot or barely undershot the target CA. The CA error pattern of female undershooting and male overshooting is intriguing, particularly as it occurs only in the 90° CA plane, corresponding to arm movement parallel to the sagittal plane, with the potential for contact with the chest mass.
Several other studies have also identified that shoulder proprioception is most accurate at higher elevations,8,29,34,37 which can potentially be explained by training of the sense with daily use of the arms out in front of the body in the 90° EA region. An additional consideration is the torque exerted on the shoulder by the weight of the arm. The torque increases as the shoulder angle increases from an EA of 0° up to 90°, where it reaches a maximum, and then decreases from an EA of 90° to 180°. While torque alone may not account for matching differences between 30° and 120° EAs, it could play a role in the high degree of position-matching accuracy observed at the 90° EA, where torque is at its peak. Studies have indicated that deficits in external rotation peak torque can lead to impairments in active JPS performance. 38 Notably, the influence of elevation-dependent torque on EA matching accuracy would be independent of CA, which aligns with our findings that EA matching accuracy does not significantly differ across different target CA.
The trend of mean CA matching error magnitude being lower than the corresponding EA matching error magnitude may be explained by a difference in the degree of proprioceptive feedback provided by glenohumeral motion compared with scapulothoracic motion. Shoulder movement occurs at the acromioclavicular, sternoclavicular, and glenohumeral joints, which contain a synovial lining, and at the scapulothoracic articulation, which is not a true joint. Matching target EA involves scapulothoracic motion in forward elevation/abduction planes where synovial mechanoreceptors experience less tension, reducing proprioceptive feedback. Matching target CA involves rotation, which may place the synovial-lined joint mechanoreceptors under greater tension, improving proprioceptive feedback. Research on glenohumeral and scapulothoracic contributions to shoulder proprioception supports this explanation, as it shows that the scapulothoracic motion has a weaker predictive effect on proprioceptive accuracy and that JPS performance depends mainly on the glenohumeral joint. 23
The directional sex-based difference observed in this study appears to be unique and, in fact, contrary to the findings of research in the field. Most studies cite no differences in shoulder proprioception between males and females.5,10,36 In 1 study that did identify a sex-based difference, it was concluded that females mostly overestimate targets compared with males 43 ; this trend is the opposite of our finding that females tend to underestimate targets in certain positions aligning with the sagittal plane. The 90° CA of the target positions where this difference was observed suggests that chest anatomy may influence position matching once a subject's arm crosses the 90° CA plane, as resistance may be felt as the arm encounters breast mass.
The system used for this study, which involves a single wrist-worn sensor no larger than a common “smartwatch,” offers an alternative tool to study shoulder proprioception—one with a shallow learning curve and low barrier to access. Devices used previously in the literature often pose technical or financial challenges. One of the most accurate systems—the isokinetic dynamometers—is costly, difficult to install, and challenging to work with in terms of hardware and protocol.2,16 More recent tools—such as laser pointer systems and inclinometers—address access obstacles but present their limitations such as restricted planar motion or changes in accuracy at different elevations. 42 Other systems—such as the electric goniometer—appear cumbersome and require high levels of patient concentration. 25
Looking ahead, the foundation laid by this project can be used to drive research on the relationship between rotator cuff tears, which affect roughly 25% of the general population,21,28,39 and shoulder proprioceptive health. The high prevalence of rotator cuff tears, combined with the poor prognostic power of magnetic resonance imaging in gauging unique patient experiences of pain and impairment, 30 makes proprioception a valuable area to investigate. Patients with rotator cuff tears display a reduction in their proprioceptive acuity3,18 and studies show that surgical repair of rotator cuff tears can restore tension in mechanoreceptors and can result in a restoration of proprioceptive acuity.26,40 Testing pre- and postoperatively can improve our understanding of the degree of initial impairment in shoulder function and can be incorporated into rehabilitation regimes to assess recovery. 3 Understanding that healthy shoulder proprioception appears most accurate at higher elevations, as shown in this study, can make these positions focal data points when studying injured shoulders.
Moreover, the sex-based differences outlined in this study suggest that we should further explore the effect of chest size on position matching at targets near the 90° CA plane. We now know that sex stratification is necessary when comparing CA matching errors at target positions within this region in future work.
Limitations
The primary limitation of this study stems from the potential for the introduction of human error during the data collection phase. The position learning phase of JPS testing involves hands-on guidance of a subject's arm to a specific target position, a task performed manually by a researcher who relies on a real-time position readout displayed on a screen. Adjustments are made based on visual feedback, which leaves room for slight shifts to occur as the subject's arm is released. Another limitation is related to the collection of subject-specific data. While study participants were recruited randomly, no data were collected to account for factors such as athletic background or other variables that may affect proprioceptive acuity and the overall fitness of shoulder musculature.
The simplicity and ease of use associated with the single-sensor system also come with their limitation—the need for careful initial calibration. During the initial positioning of participants in the at-rest reference position (with their arm down by their side while seated), it is crucial to ensure that the sensor's face remains parallel to the coronal plane. The accuracy of data collection is closely linked to this initial referencing, and significant shifts on the part of the subject may affect the referencing process and later data-processing steps.
Last, the device used in the study exhibits sensitivity to metal interference, necessitating that participants be tested in a metal-free chair and an environment free of metal within a radius of several feet. All testing conducted for this study adhered to this requirement, and it is essential to maintain the same standard in any future device use.
Conclusion
The JPS testing performed in this study confirmed that the accuracy of shoulder proprioception improves at higher elevation angles in both males and females. The position-matching data also revealed a new sex-based difference in shoulder proprioception, with females undershooting target position CA compared with males at targets in or beyond the 90° CA plane. This trend calls for sex stratification in future studies when testing targets positioned around 90° CA. The findings of this study enhance our understanding of proprioceptive accuracy in the uninjured shoulder and offer baseline data that can be used to evaluate proprioceptive deficits in patients with conditions like rotator cuff tears or instability. The portable, 3-dimensional system developed for this study delivers valuable functional data, which can be integrated with imaging to improve treatment decisions and rehabilitation strategies.
Footnotes
Acknowledgements
The authors thank Layla Lynch and Joe Confessore for their involvement in participant recruitment and testing.
Correction (April 2025):
This article has been updated to correct the y-axis in Figure 2.
Final revision submitted August 17, 2024; accepted September 10, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.A.A. has stock/stock options in Anika Therapeutics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Lifespan, Research Protection Office (reference No. 1809128-1).