Abstract
Objectives:
Increased knee posterior tibial slope (PTS) angle is risk factor for primary and secondary ACL injury. Adult biomechanical research indicates that decreasing the PTS may reduce ACL injuries, and osteotomy techniques have been developed to alter tibia slope to reduce risk of re-injury. Pediatric and adolescent athletes have the highest rates of primary and secondary ACL injury, and many in this age group may have abnormal PTS angle. The purpose of this study was to evaluate PTS in medial and lateral tibial plateaus in large database of CT scans, and to develop normative PTS data in this age group.
Methods:
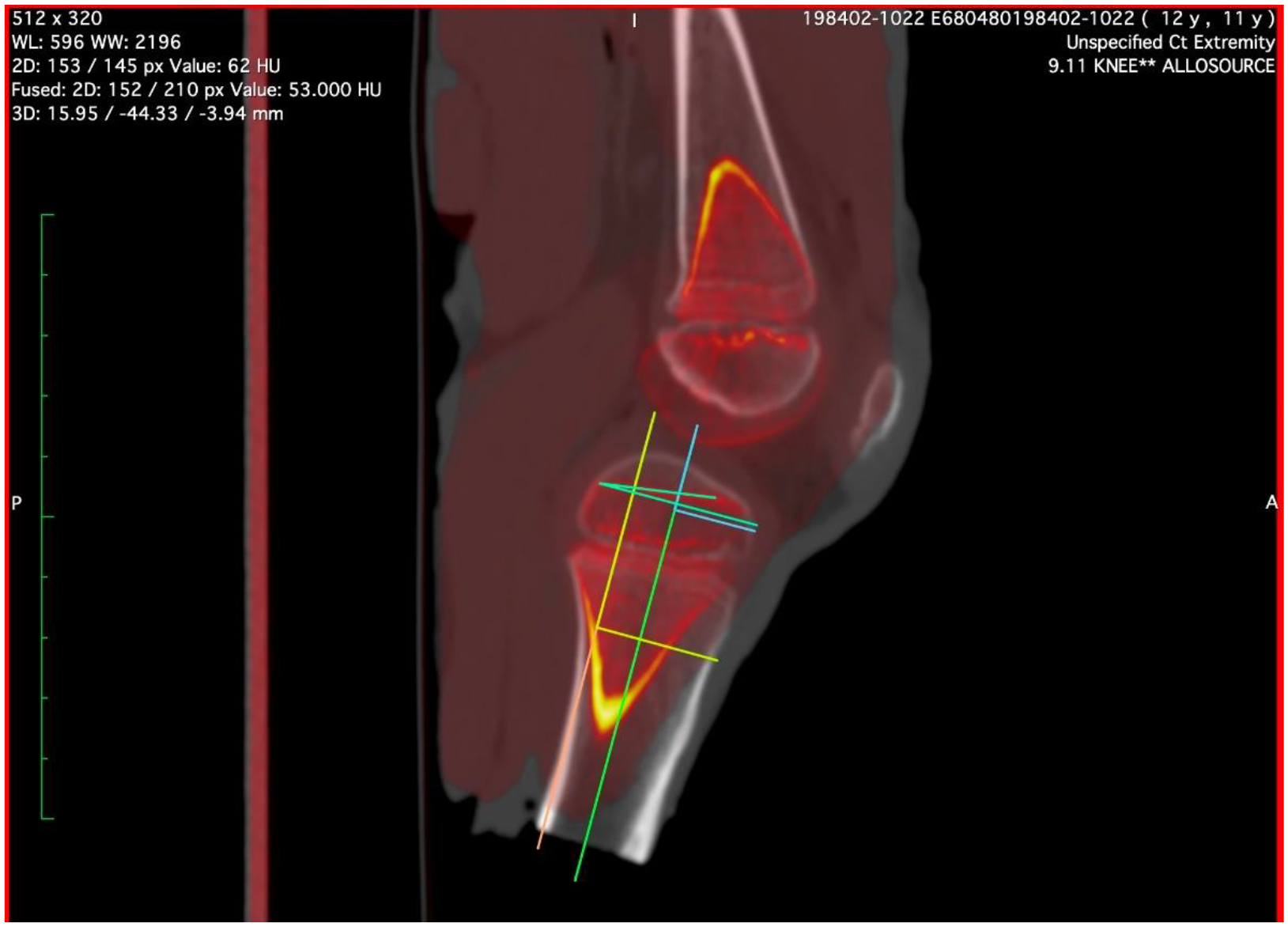
IRB approval was waived, as the specimens were donated for research, no genetic information was collected, and there were no plans for family contact. 83 pediatric knee CT scans, ranging from ages 1 to 12, were analyzed using OsiriX imaging software. The PTS was evaluated at two distinct points on sagittal CT sections: (1) At the medial tibia plateau and 2) lateral tibial plateau, both aligned with the central part of on a coronal view of the medial femoral and lateral femoral condyles respectively condyle.
Results:
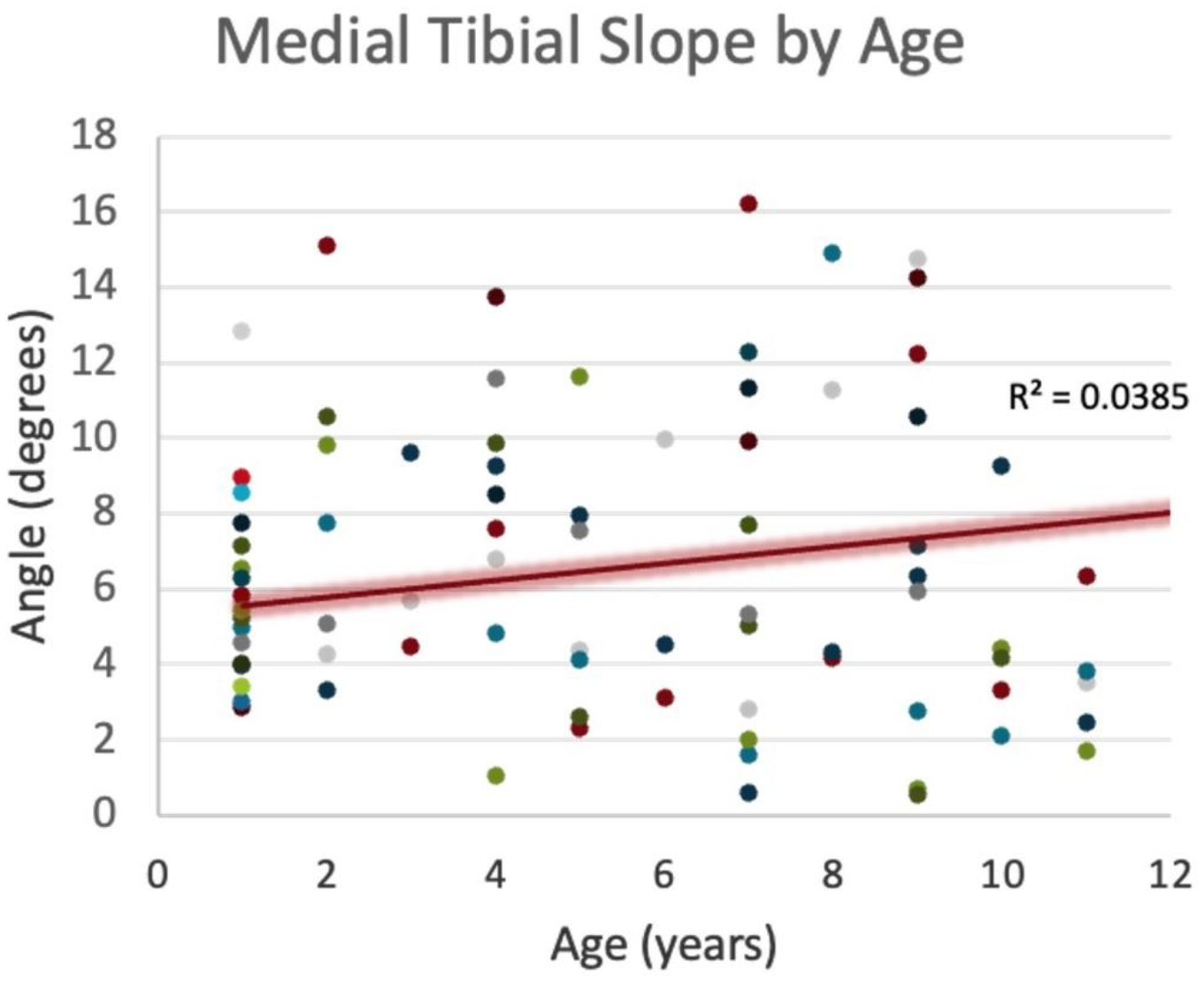
The average medial PTS angle was 6.56° ± 3.84° and 6.81° ± 3.62° for the lateral PTS. There was not a significant statistical difference between the medial and lateral PTS (P = 0.6632, determined using an independent-samples t-test and analysis of variance). When plotting the age versus PTS, we observed a positive correlation with the medial PTS (R2 = 0.0385) and a negative correlation with the lateral PTS (R2 = 0.0393).
Conclusions:
The data demonstrate variability in medial and lateral pediatric PTS and provides normative values for pediatric PTS values. For pediatric patients undergoing ACL surgeries, consideration of increased PTS values that are associated with higher rates of recurrent ACL injury may influence surgical treatment techniques. Correction of increased PTS to lower ACL injury risk is performed in adults with major corrective osteotomy surgery, but such procedures have not been performed in children due to osteotomy-induced damage to growth plates. Due to open growth plates, pediatric patients may be treated with minimally invasive guide growth procedures to lower PTS, with minimal complication risk. Guided growth procedures have a long history of successful alignment correction in the coronal plane. Future animal and clinic studies may also demonstrate the safety and effectiveness of guided growth sagittal plane correction as applied to increased PTS. PTS developmental anatomy and its relationship to ACL injury is crucial for surgical advancements, including the use of low risk guided growth interventions to reduce PTS and ACL injury in pediatric patients with high risk of recurrent injury.