Abstract
Objectives:
Recent studies have been using the anterior cruciate ligament reconstruction (ACLR) mouse model to study the tendon-bone healing process and the development of post-traumatic osteoarthritis. While it is known that mechanical load has an important effect on ACL graft healing, a limited number of studies have investigated the impact of treadmill exercise. No study has yet examined the effects of different exercise regimens following an ACLR in mice. The purpose of this study is to explore the effect of different mechanical loading stimuli on the tendon-bone interface (TBI) healing process following ACLR in mice. We hypothesized that moderate loading would positively affect TBI healing after ACLR.
Methods:
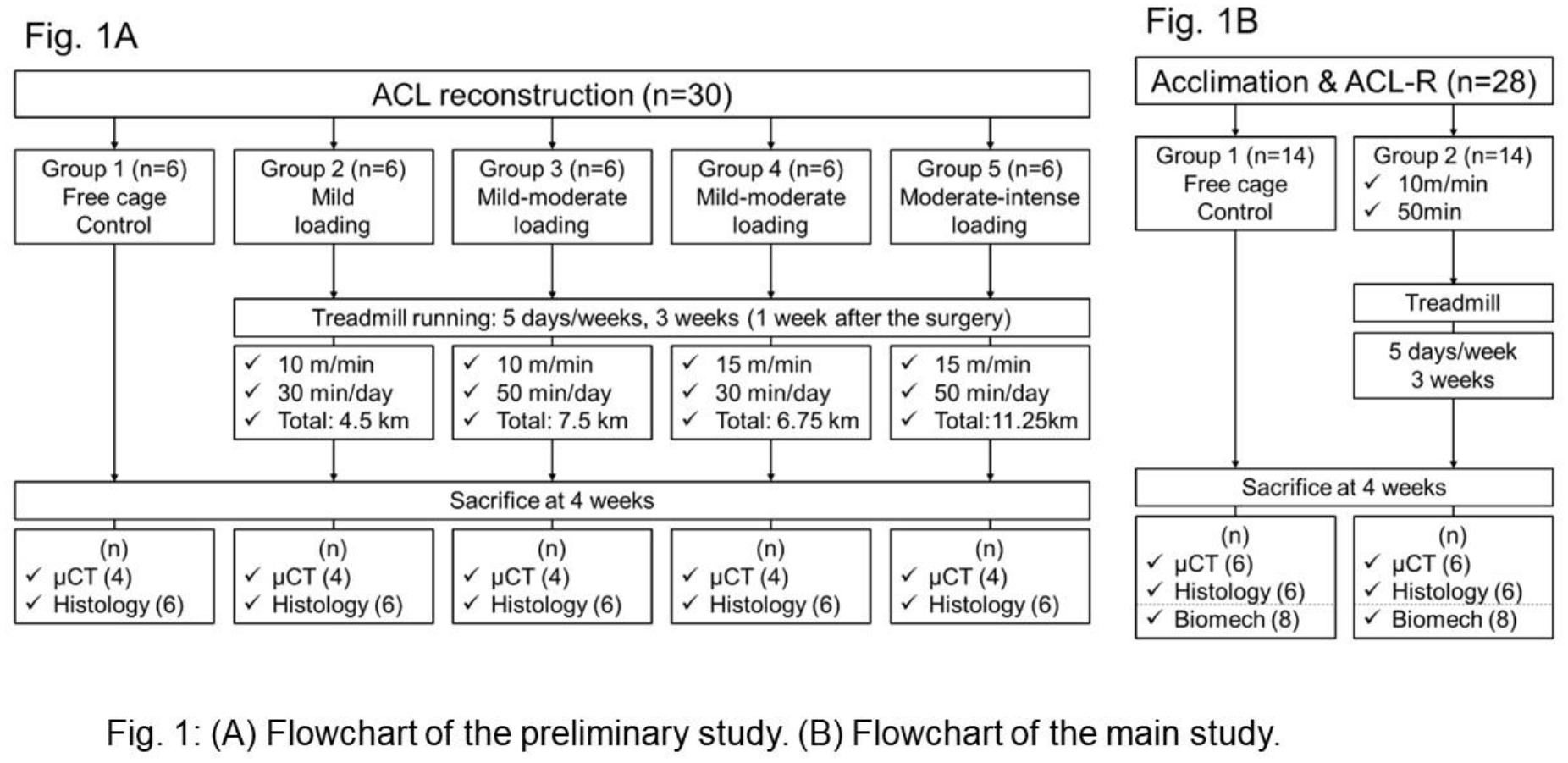
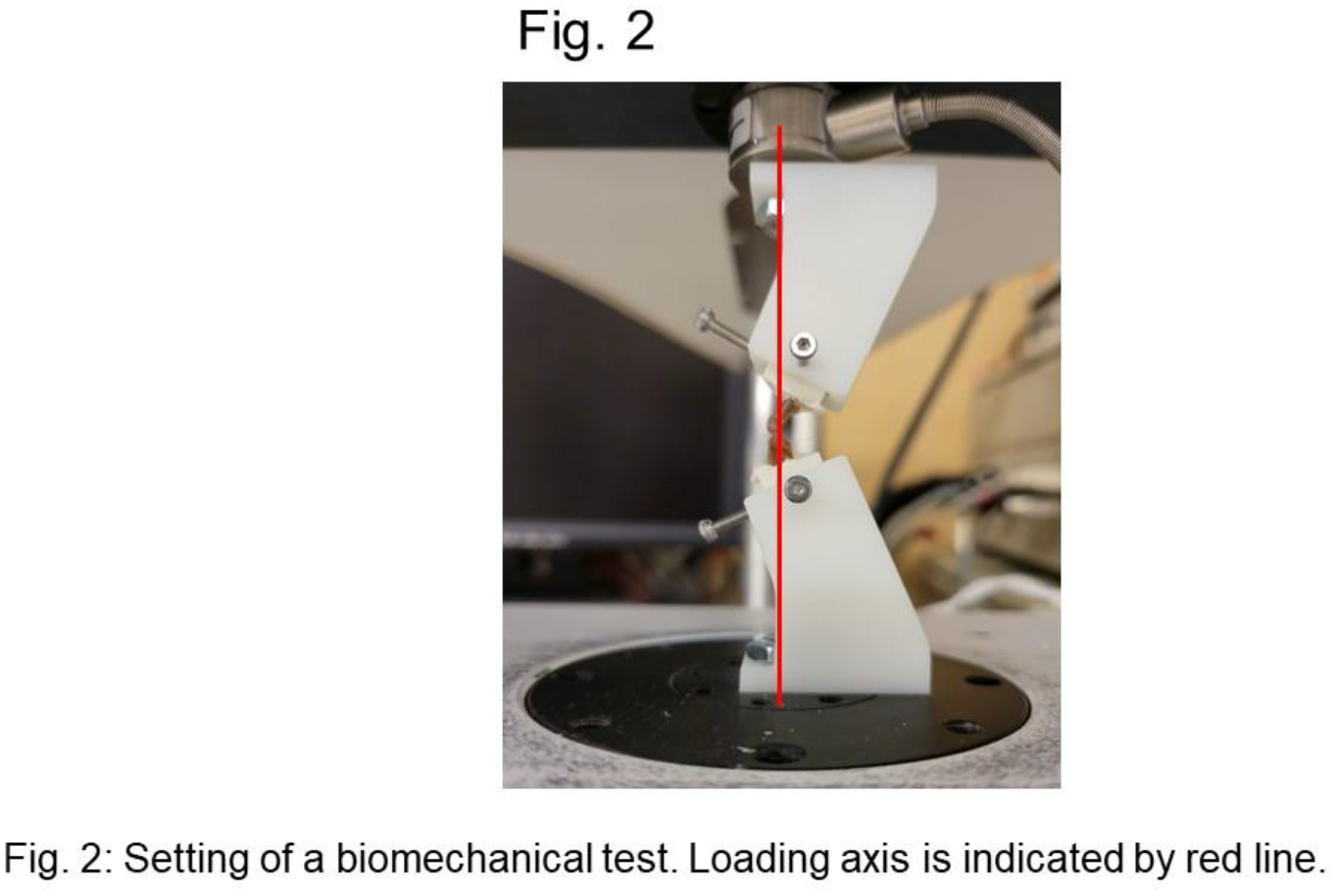
The study protocol was approved by our Institutional Animal Care and Use Committee (IACUC 2020-0024). A total of 58 C57BL/6 (12 weeks old) male mice underwent to an ACL reconstruction in the right knee as previously described. The first 30 mice were assigned into 5 different exercise groups (n=6 per group) and used to evaluate different exercise regimens (Study Arm 1- Fig. 1A). After identifying the optimal exercise regimen, an additional 28 mice were included in the study (Study arm 2 - Fig. 1B). All mice were acclimated on the treadmill following a 5-day acclimation protocol prior to surgery. Starting 7 days post-surgery, the treadmill exercise was performed 5 days/week for a total of 3 weeks. All animals were euthanized at 4 weeks post-surgery. Micro-CT imaging was performed using a Scanco mCT 45 system (Scanco Medical). The bone tunnel was identified, a region of interest (ROI) was defined as the bone tunnel diameter (0.64mm), and bone volume fraction (bone volume/total volume), bone mineral density, and trabecular number were evaluated in the tibial tunnel. Biomechanical Testing was performed in a materials-testing machine (EnduraTEC ELF 3200) (Fig. 2). The knee joints were carefully dissected to isolate the ACL graft. Custom fixtures were designed to ensure that the ACL was aligned in the direction of loading. The specimens were subjected to load until failure at a rate of 5.0 mm/min and the load-to-failure (N) data were recorded. The tendon-to-bone tunnel healing (TBTH) was further evaluated using a well-established histological scoring system [4]. Paraffin-embedded samples were cut into sagittal and axial planes. Hematoxylin and eosin as well as Picrosirius red staining were performed, followed by examination and photography using both brightfield and polarized light microscopy. Statistical analysis was performed by a Wilcoxon signed-rank test in GraphPad Prism 6 software. Statistical significance was defined as a p-value of less than 0.05 (P<0.05).
Results:
In study arm 1 no significant difference was observed in micro-CT analysis and histological assessment (sagittal slices of the entire tibia) among the groups. Although the sample size was limited, the most relevant trend was observed in the 10m/min, 50min treadmill group compared to the free cage group. Further analysis of micro-CT and biomechanical testing in study arm 2 revealed no significant differences between the groups. However, histological evaluation (axial slices of the femoral/tibial intra-articular/extra-articular parts; Fig. 3) demonstrated significantly higher TBTH scores in the treadmill group compared to the free cage activity group. This difference was most pronounced in the extra-articular region of the femoral tunnel (4.1 vs. 8.4, *P=0.02), as well as in the intra-articular part of the tibial tunnel (6.9 vs. 18.0, **P<0.01). Furthermore, significantly higher TBTH scores were observed in the extra-articular part of the tibia compared to those of the femur, both in the free cage (4.1 vs. 17.3, **P<0.01) and the treadmill group (8.4 vs. 19.3, **P<0.01). Additionally, within the treadmill group, the extra-articular part of the tibia exhibited a significantly higher TBTH score compared to that of the femur (6.6 vs. 18.0, **P<0.01).
Conclusions:
The most important finding of this study is that TBI healing exhibited better outcomes in the extra-articular part of the femur and the intra-articular part of the tibia among the treadmill group compared to those in the free cage group. These findings suggest that moderate treadmill exercise following ACLR has a positive impact on TBI healing in both the femoral and tibial tunnels, confirming our hypothesis. The lack of a significant difference in the biomechanical test between the groups could potentially be attributed to incomplete healing of the graft in the femoral tunnel across all groups. Failure during biomechanical testing was most often observed on the femoral side. Further studies are warranted to achieve a more robust sample size, investigate alternative loading regimen such as periods of immobilization followed by remobilization, and higher intensity treadmill running (20m/min) to evaluate TBI healing following ACLR. A moderate load rehabilitation protocol might potentially result in improved healing of the tendon graft-to-bone interface following ACLR.