Abstract
Objectives:
Tunnel widening can occur following ACL reconstruction (ACL-R). Tunnel widening can be challenging when faced with revision and can be an indication of poor graft/tunnel healing. In this study, we aim to focus on the effect of bone tunnel length on ACL graft healing. We hypothesized that shortening the femoral and tibial bone sockets during all-inside ACL-R (without an interference screw and with increased contact between the graft and the bottom of the socket) can improve graft maturation and decrease bone tunnel widening. The objective of this study is to compare the clinical outcomes, graft maturation and post-operative bone tunnel widening between all-inside ACL-R with short bone sockets and anteromedial portal ACL-R.
Methods:
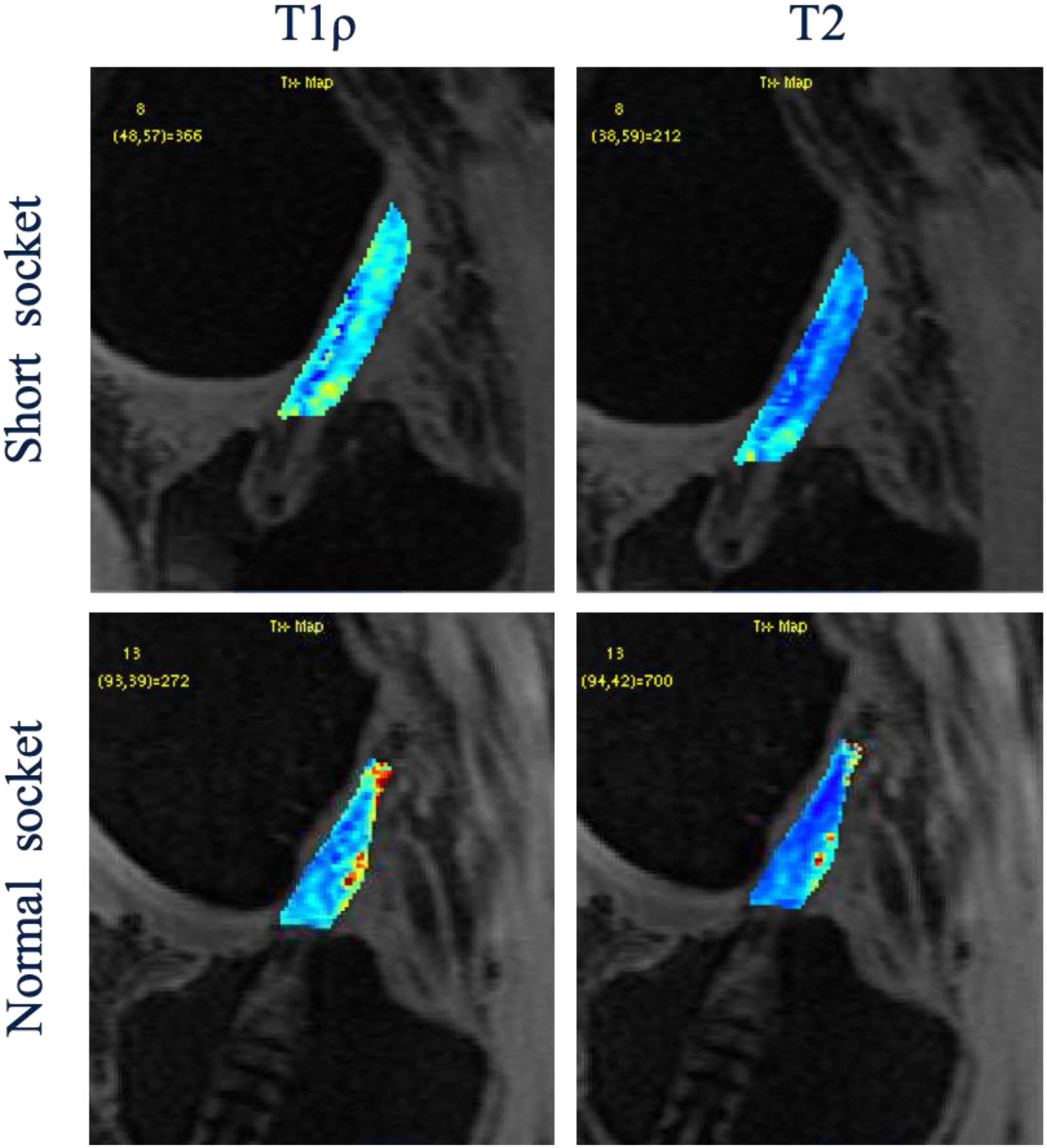
We prospectively evaluated patients who underwent ACL-R with a hamstring autograft at our institution from 2021 to 2023. Surgical reconstruction was performed by one of three fellowship-trained sports medicine orthopedic surgeons. In the all-inside ACL-R with short socket (Short socket group), the femoral and tibial sockets were drilled using an outside-in retroreaming technique for a depth of 10- and 15-mm socket, respectively. The graft was passed and fixed with suspensory fixation on the femoral side (Infinity Femoral Adjustable Loop Button, CONMED, Largo, FL). It was then tensioned with the knee at 30 degrees and end button fixation was used on the tibial side (Infinity Standard Tibial Button, CONMED, Largo, FL). In the ACL-R with normal tunnel (Normal socket group), the femoral tunnel was created using a reamer through the anteromedial portal that is 20 mm deep and a full tibial tunnel created using outside in drilling. The graft was fixed with suspensory fixation on the femoral side (RIGIDLOOP, Depuy Synthes, Raynham, MA or Ultrabutton Adjustable Fixation Device, Smith & Nephew, Watford, England, UK) and with a sheath and interference screw on the tibial side (Intra-Fix, Depuy Synthes, Raynham, MA). To assess patients reported outcome (PRO) score, International Knee Documentation Committee (IKDC) score, Marx activity scale and Knee Osteoarthritis and Injury Outcome Score (KOOS) were completed at 6 and 12 months follow up. Postoperative 3T magnetic resonance (MR) imaging was acquired 6 and 12 months after surgery. A 3D combined T1ρ/T2 MAPSS sequence and a high-resolution 3D fast spin-echo sequence (CUBE) were obtained in the sagittal plane. Measurement of tunnel diameter and tunnel cross-sectional area (CSA) were calculated perpendicular to the long axis of the tunnel at 5 mm from the joint-tunnel interface via the 3D multiplanar reconstruction (MPR) function based on 3D CUBE images. The percentage of tunnel widening (% of original diameter and CSA) was determined by dividing the measured diameter and CSA by the initial diameter and CSA according to the diameter of tunnel or interference screw during surgery. To assess graft maturation and healing, a manual segmentation for ACL graft was performed to obtain the T1ρ and T2 relaxation time of the intra-articular portion of the ACL graft. We also segmented the ACL graft within the femoral and tibial tunnel and obtained the T1ρ and T2 relaxation time at 5 mm beyond the tunnel aperture. Statistical analysis was made using Mann-Whitney test to obtain the differences between the two groups. Significance level was set at p = 0.05.
Results:
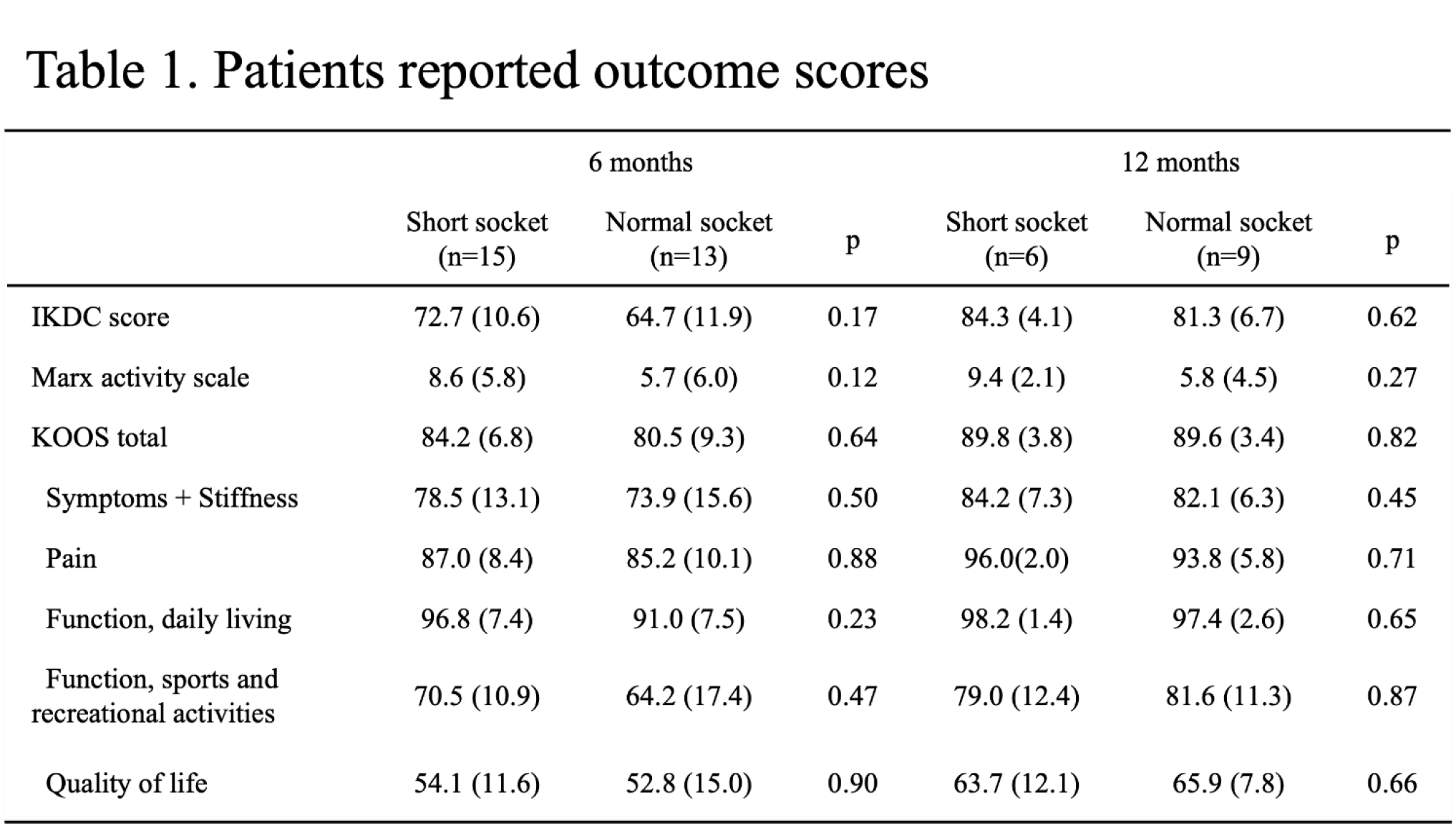
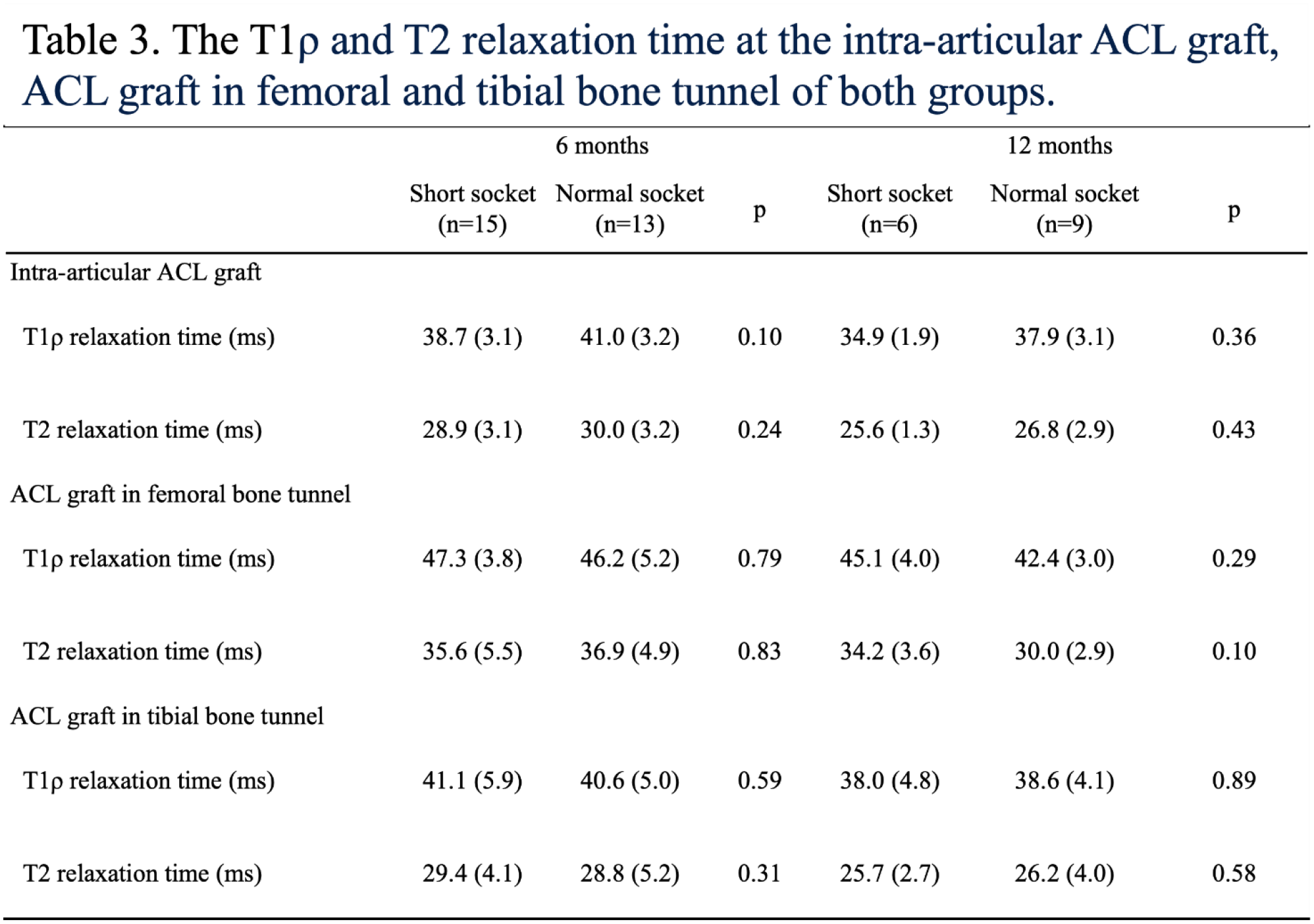
There were 28 patients who were enrolled in this study. 15 patients were in the Short socket group and 13 patients were in the Normal socket group at 6 months postoperatively, and 6 patients were in the Short socket group and 9 patients were in the Normal socket group at 12 months postoperatively. There were no significant differences in age, BMI, sex, and graft diameters between the two groups. There were no significant differences in PRO scores between the two groups at 6 and 12 months (Table 1). The % of original diameter in femoral and tibial socket of the Short socket group (99.3% ±17.3% and 100.1% ± 9.7%, respectively) were significantly lower than those of the Normal socket group (117.0% ± 12.7% and 119.8% ± 10.6%, respectively) at 6 months postoperatively. The % of original CSA in femoral and tibial socket of the Short socket group (109.2% ± 36.1% and 109.0% ± 18.6%, respectively) were significantly lower than those of the Normal socket group (145.6% ± 21.8% and 144.55 ± 24.7%, respectively) at 6 months postoperatively (Table 2). The % of original CSA in tibial socket of the short socket group 126.7% ± 36.3% were significantly lower than that of the Normal socket group 140.6% ± 21.8% at 12 months postoperatively (Table 2). For graft maturation, there were no significant differences of the ACL graft in mean T1ρ and T2 relaxation time between the two groups (Figure1 and Table 3). For graft healing within the tunnels, there were also no significant difference of the ACL graft signal between the two groups (Table 3).
Conclusions:
We observed significantly less postoperative bone tunnel widening on the femoral and tibial side in all-inside ACL-R with short sockets compared to regular femoral socket length and full tibial tunnel ACL-R, while achieving the same clinical outcome and graft maturation and healing. Short socket ACL-Rs can offer advantages by decreasing the amount of bone removed, especially when faced with revision ACL-R. Further studies are being performed to evaluate longer-term follow-up and also the significance in differences in the development of post-traumatic arthritis.