Abstract
Objectives:
Anterior cruciate ligament (ACL) tears are common knee injuries that greatly increase osteoarthritis (OA) risk. By 1 year after ACL reconstruction (ACLR), most patients have been released to unrestricted activities. However, ACLR does not fully restore knee mechanics and altered knee loading has been associated with greater OA risk. Knee mechanics can be challenging to measure. Consequently, clinical outcomes are more commonly assessed using patient reported outcomes (PRO) such as the Knee Injury and Osteoarthritis Outcome Score (KOOS). Patient acceptable symptom state (PASS) criteria were developed to aid in the interpretation of the KOOS. This study was performed to test the following hypotheses: (1) that loading patterns of ACLR knees 2 years after ACLR differ between patients who achieve an acceptable symptom state (PASS-Y) and those who do not (PASS-N); and (2) that those who fail to reach PASS exhibit loading patterns associated with greater pain and higher OA risk.
Methods:
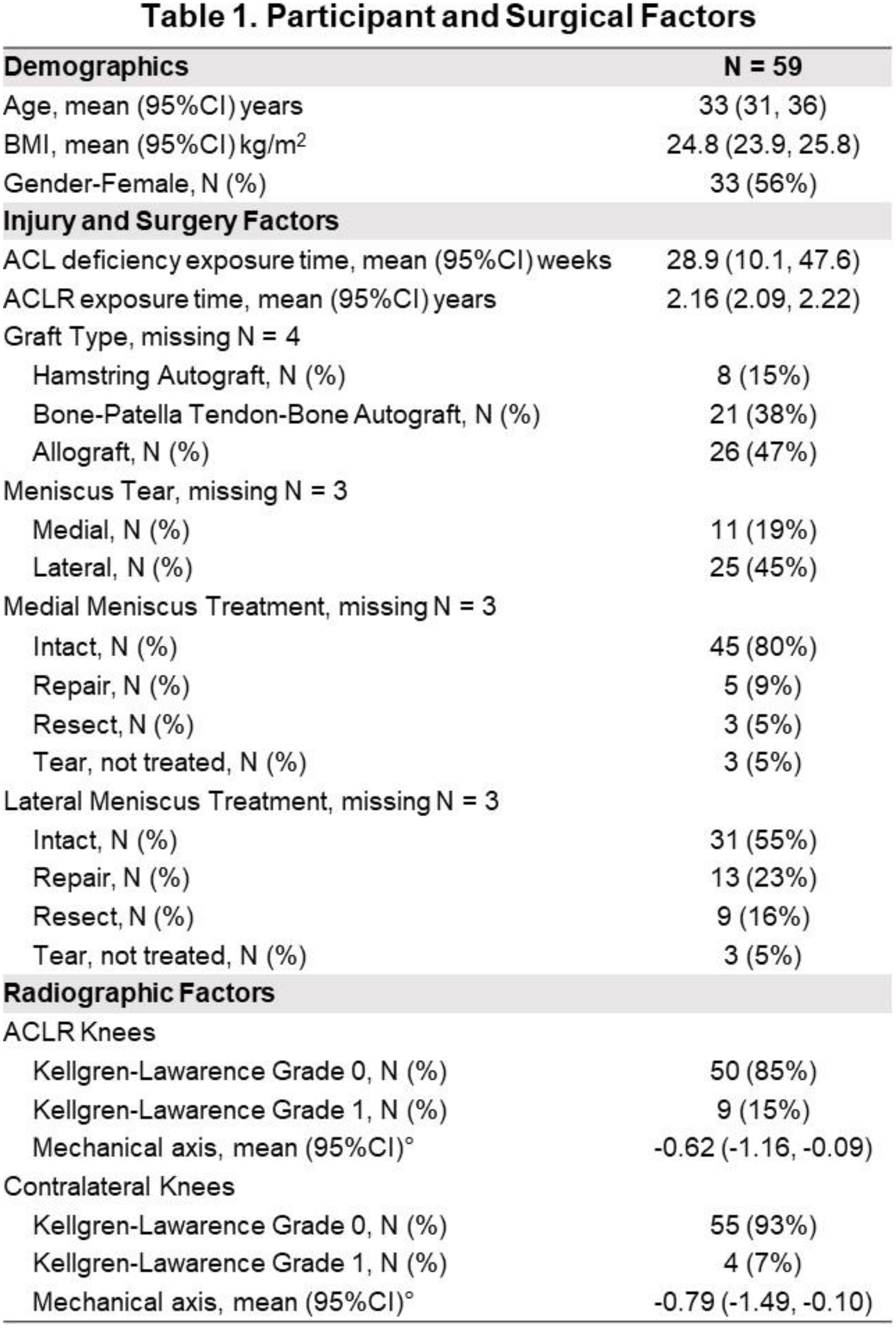
This IRB-approved study included 59 individuals who completed the KOOS and underwent gait analysis 2 years after primary unilateral ACLR (
Results:
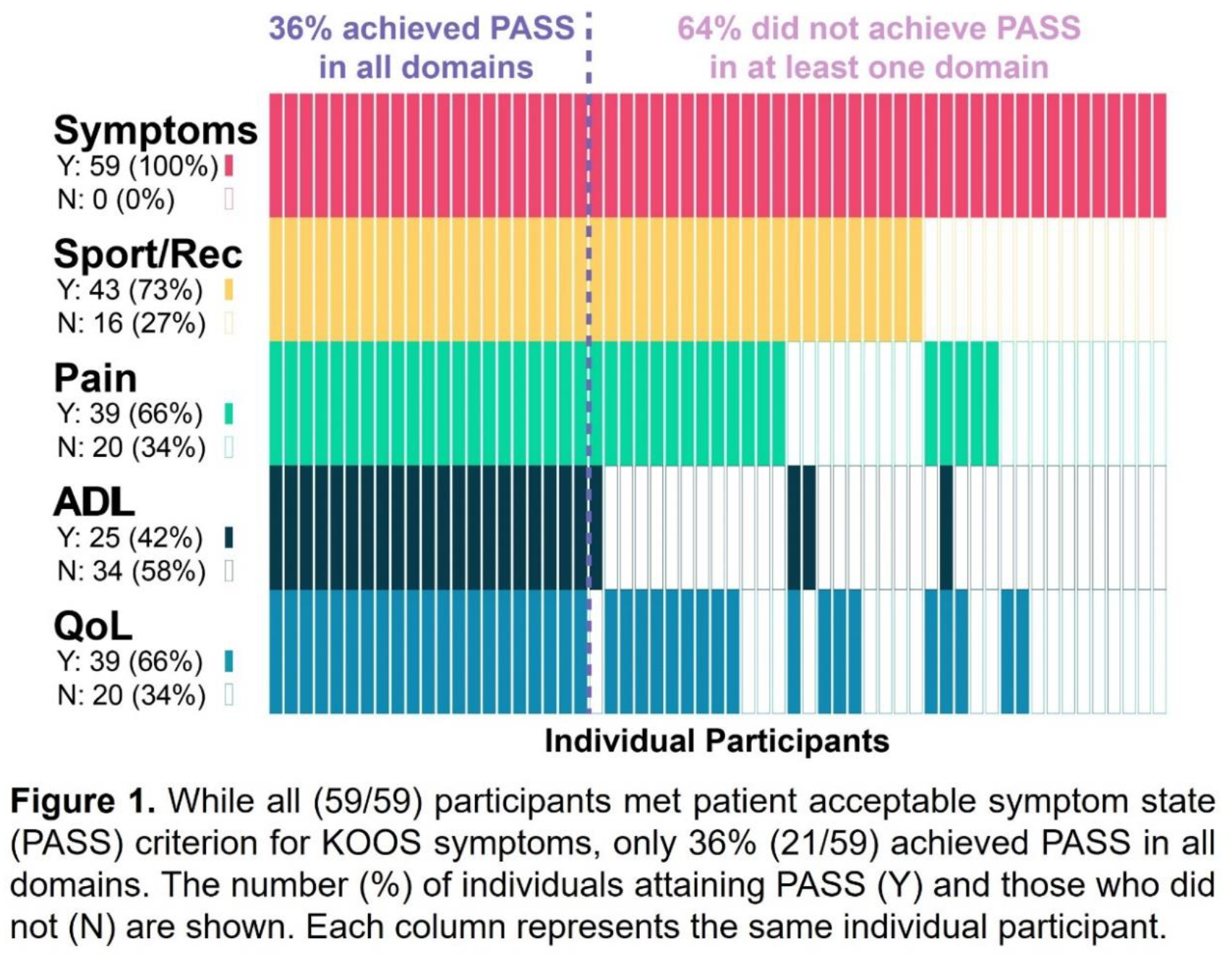
While all participants (59/59) met PASS-Y for symptoms, only 36% (21/59) achieved PASS in all domains (
Conclusions:
Nearly two-thirds of patients 2 years after ACLR did not achieve PASS in at least one KOOS subscore. Failure to achieve PASS correlated with quantitative gait data reflecting altered loading known to reduce longer term outcomes. These data demonstrated utility and sensitivity of the KOOS subscore PASS criteria for personalized assessment of outcomes early after ACLR where the relative lack of symptoms may mask suboptimal recovery. Furthermore, participants 2 years after ACLR who did not consistently reach PASS exhibited loading patterns associated with greater pain and greater OA risk than those achieving PASS-Y. Cross-sectionally greater KAM 2 years post-ACLR has been shown to correlate with medial knee degenerative changes at the same time point and to predict worse outcomes 8 years after ACLR. ACLR knees with a lower KFM than contralateral knees also exhibited altered extensor/flexor co-activation patterns. The KFM and TJM are responsive to changes in pain and are indicative of knee muscle strength and activation. This means that interventions aimed to increase KFM and to restore the relative loading contributions (%KFM & %KAM) to TJM may lead to improved quadriceps strength and pain relief. The absolute loading metrics, as suggested by the regression analyses, may also have predictive value for identifying participants who may benefit from additional interventions.
Significance:
These data suggest that KOOS PASS criteria may be an accessible screening tool to provide early warning of patients at higher risk for poor outcomes who may potentially benefit from further assessment, additional physical therapy, or closer follow-up.