Abstract
Objectives:
Medial patellofemoral ligament reconstruction is performed to address cases of patellar instability. Historically, this is a well-tolerated procedure though complications, including redislocation and recurrent instability can occur. While risk factors for redislocation following MPFLR have been proposed, there remains no agreed upon consensus. This is even more true in setting of isolated MPFL reconstruction, as concomitant procedures may naturally exclude certain anatomic risk factors. The purpose of this study was to correlate demographic, anatomical, and clinical risk factors to redislocation following isolated medial patellofemoral ligament reconstruction (MPFLR).
Methods:
A retrospective review of patients who underwent isolated MPFLR for recurrent patellar instability at a single institution between December 2015-June 2021 was performed. Included patients had a minimum of 2 years of follow-up data available. Demographic, pre-operative radiographic, surgical, and clinical data was compared between those who had a dislocation event after surgery and those who did not. Subluxation and subjective instability were not considered dislocation events. Independent samples T-test and univariate binary logistic regression was performed.
Results:
This study included 126 patients with a mean age of 21.74 ± 9.20 and a mean BMI of 25.93 ± 6.36. Of these, 67.5% were female and 61.9% of operations were on the left knee. In total, 8.7% (11/126) of patients experienced a redislocation event with a mean time to redislocation of 19.11 months after surgery (range 5 – 32 months). On preoperative magnetic resonance imaging (MRI), greater trochlear bump height measured to bone (p=0.032) and measured to cartilage (p=0.033) was associated with redislocation
Conclusions:
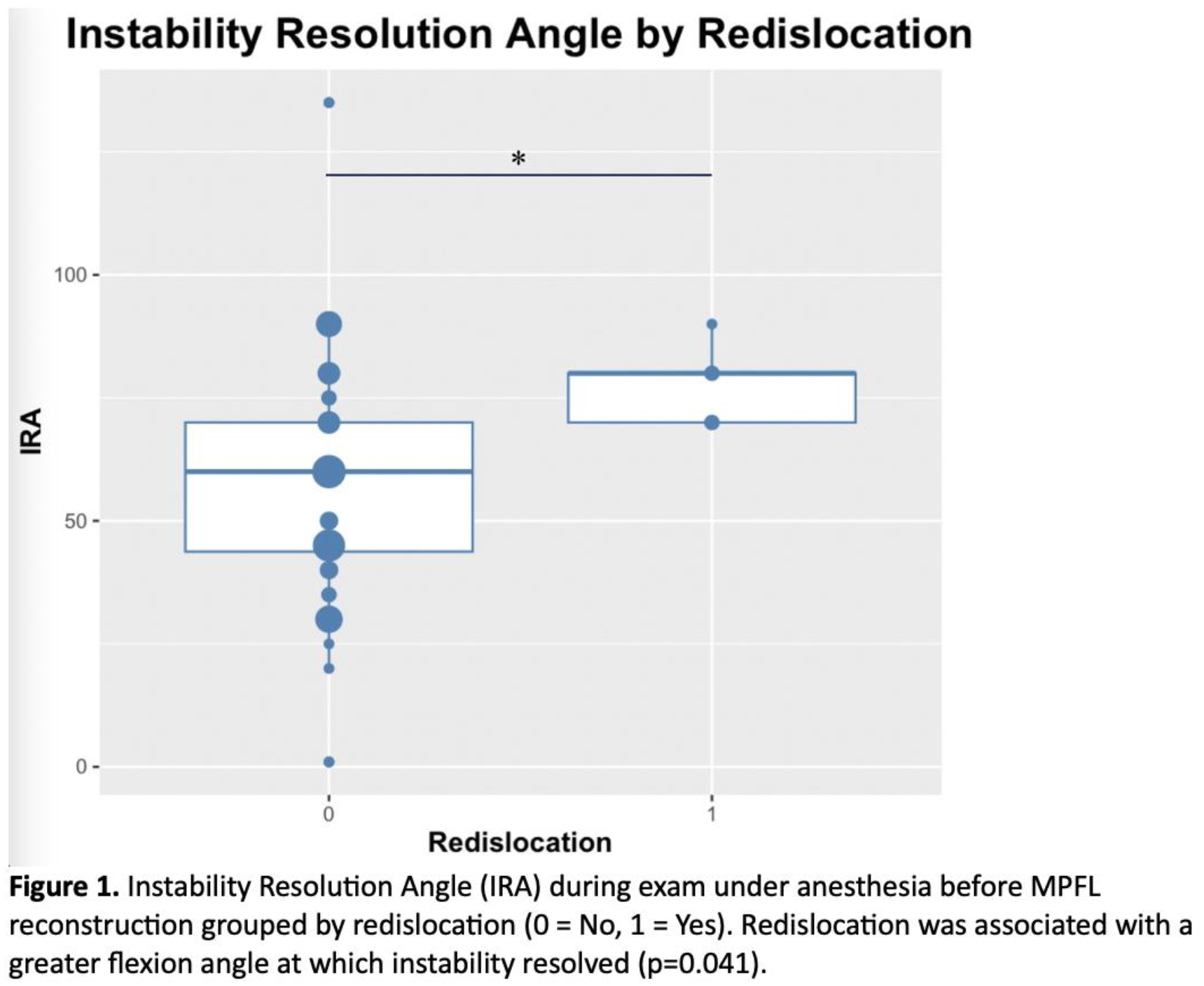
MPFLR is associated with a high level of success with a redislocation rate of 8.7% in this study. On pre-operative MRI, wide sulcus angle and increased bump height measured to bone and to cartilage were risk factors for redislocation. Additionally, redislocation was associated with a greater flexion instability resolution angle (IRA).