Abstract
Objectives:
Rotator cuff calcific tendinopathy (RCCT) is a common condition characterized by the presence of calcific deposits in the rotator cuff tendons or the subacromial space. Its prevalence in individuals experiencing shoulder pain ranges from 7.3% to 42%. This condition mainly affects people aged between 30 and 60 and is more common among women. Subacromial corticosteroid injections (SAI) are considered a standard treatment for RCCT. Although ultrasound-guided barbotage (UGB) is thought to improve clinical and radiographic outcomes in treating RCCT, its impact on the rate of subsequent shoulder surgery has yet to be characterized on a large scale. This study aims to determine the rate of shoulder arthroscopy among patients treated with UGB and SAI for RCCT and analyze other contributing factors (e.g., calcification size, number of procedures, age, and sex).
Methods:
After institutional review board (IRB) approval was obtained, all medical records at a single institution were retrospectively reviewed to identify patients diagnosed with RCCT between March 2013 and March 2023. Patient records were identified using ICD 9 and 10 diagnosis codes and current procedural terminology codes. When individual patients were treated with multiple procedures, each procedure was included in the analysis. Imaging reports were reviewed to determine the size, location, and quantity of calcific lesions. Additionally, patients' demographics were also extracted. The percentage of patients undergoing shoulder surgery was compared between patients that received UGB versus SAI, comparing the number of UGB and SAI procedures prior to surgery, calcific lesion size, lesion location, patient age, and patient gender.
Results:
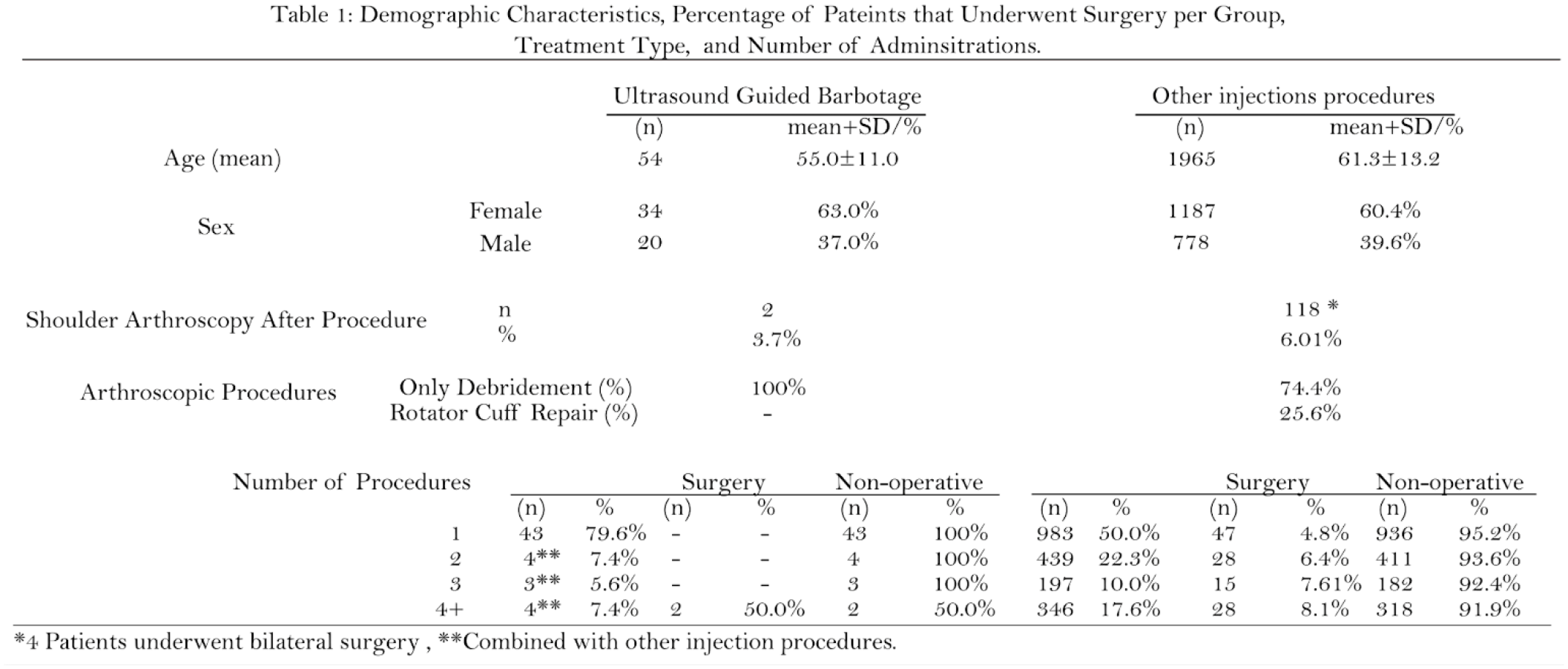
A total of 6,021 RCCT patients were identified, including 2,019 patients who underwent UGB and/or SAI procedures (mean age, 61.1±13 years [60%] female). Patients in the UGB group were younger (55±11years) than the SAI group (61.3±13 years old). The percentage of patients who underwent subsequent shoulder surgery was lower in the UGB group (3.70%, 2 of 54 patients) than in SAI procedures (6.01%,118 of 1943). The 2 patients in the UGB group who underwent surgery underwent 3 SAI procedures prior to UGB. Conversely, most of the patients in the UGB group (80%) underwent a single barbotage procedure (Table 1).
In the SAI group, 50% of patients had a single injection, 22% underwent 2 injections, and 28% underwent 3 or more injections. Notably, multiple SAI procedures correlated with an increased rate of subsequent surgical procedures (Table 1). Although the percentage of patients undergoing a surgical procedure was slightly higher among men than women (6.4% vs. 5.7%), no statistical difference was found between the genders overall. On the other hand, women ages 41 and 50 years old had a lower risk of undergoing surgery than their male counterparts (3.4% vs. 11.8%, RR: 0.3 [95%CI, 0.1-0.8]; p=0.01) (Table 2). A similar trend was observed when comparing patients over 71 years old versus the rest (2.7% vs. 7.1%, RR:0.4 [95%CI, 0.2-0.7]; p=0.001). Conversely, there was a contrasting trend in patients ages 61 to 70 years old (7.9% vs. 5.3%, RR: 1.5 [95%CI, 1.04-2.1]; p=0.03) (Table 2).
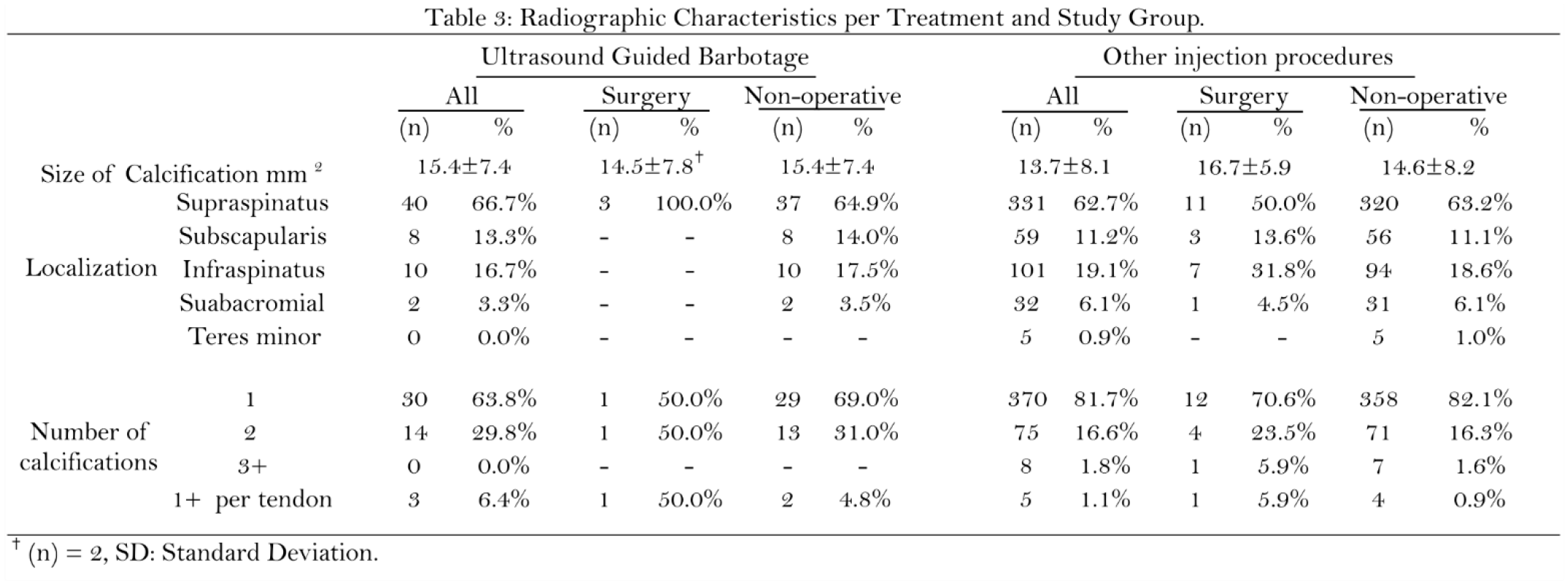
The radiographic report review (n=486) determined that 400 (80%) patients had a single calcific deposit, and the most common location of calcifications was the supraspinatus tendon (63.2%), followed by the infraspinatus (18.6%) and the subscapularis (11.1%). There was a slight difference in the mean size of the calcifications between the UGB group (15.4±7 mm) and the SAI group (13.7±8 mm). No difference was found between the 2 patients who underwent surgery after UGB (14.5±8 mm.) and the nonoperative patients (15.4±7mm). However, in the SAI group, patients who underwent surgery had larger calcifications (16.7±5 mm) than those who did not (14.6±8 mm). Additionally, calcifications measuring over 15 mm and 20 mm had a higher percentage of eventual surgical management (7.5% and 8.6%, respectively) than the overall SAI group (6%) (Table 3).
Conclusions:
The results indicate that patients who underwent UGB had a lower likelihood of requiring surgery compared to those initially treated with SAI (3.7 % vs. 6.01%; odds ratio: 0.60). It was observed that 11 patients received both UGB and SAI procedures, and among these patients, 2 underwent surgery. There was a tendency between more previous SAI procedures and a higher percentage of surgical procedures.
The most commonly involved tendon was the supraspinatus (63%), followed by the infraspinatus (19%) and subscapularis (11%), which aligns with past epidemiologic series. In the UGB group, there were no differences in mean calcification size between patients undergoing operative and nonoperative treatment, which may be attributed to the small number (n=2) of patients who underwent surgery. In the SAI group, there was a higher percentage of patients requiring surgery for calcifications larger than 15 mm and 20 mm in this group.
In our series, patients undergoing UGB demonstrated a lower relative risk of being treated with a surgical procedure for treating RCCT compared with SAI procedures. The surgery rate in patients with RCCT is influenced by factors such as age, sex, and the number of previous procedures.