Abstract
Objectives:
Patients often experience a significant amount of muscle and bone atrophy following Achilles tendon rupture and surgical repair due to mechanical unloading and an inability to safely perform resistance training at intensities sufficient to preserve mass in the early postoperative period. This potentially increases the risk of reinjury, increases recovery time, and delays return to sports. Low intensity resistance training combined with blood flow restriction (BFR) therapy has been shown to induce muscle hypertrophy similar to high intensity exercise while mitigating the risks during the early postoperative period. The objective of this study was to determine if BFR added to the standard postoperative rehabilitation protocol would reduce skeletal muscle and bone atrophy in the lower extremity compared to traditional rehab following Achilles tendon reconstruction. Secondary outcome measures were changes in muscular strength and improvement in functional outcomes.
Methods:
A total of 19 patients undergoing acute Achilles tendon rupture repair were randomized into 2 groups (12 control, 7 BFR). Patients underwent 15 weeks (wks) of postoperative rehabilitation (2/wk) and performed the same standardized protocol. The BFR group performed select exercises under 80% arterial occlusion of the postoperative extremity. Body composition, total lean mass, lower extremity bone mass, thigh lean mass, calf lean mass, and bone mineral density (BMD) of the tibia were measured presurgery, prior to physical therapy (wk3), 8wks post-operatively, and 16wks post-operatively for all subjects. Calf girth, single-leg (SL) squat, single heel raise test, and gastrocnemius and soleus strength were measured in both the operative and contralateral legs at 8wks and 16wks postoperatively. Data were analyzed using a 2(group)x3(time) analysis of covariance repeated on timepoint and covaried on initial measurement values (significance set at p<0.05).
Results:
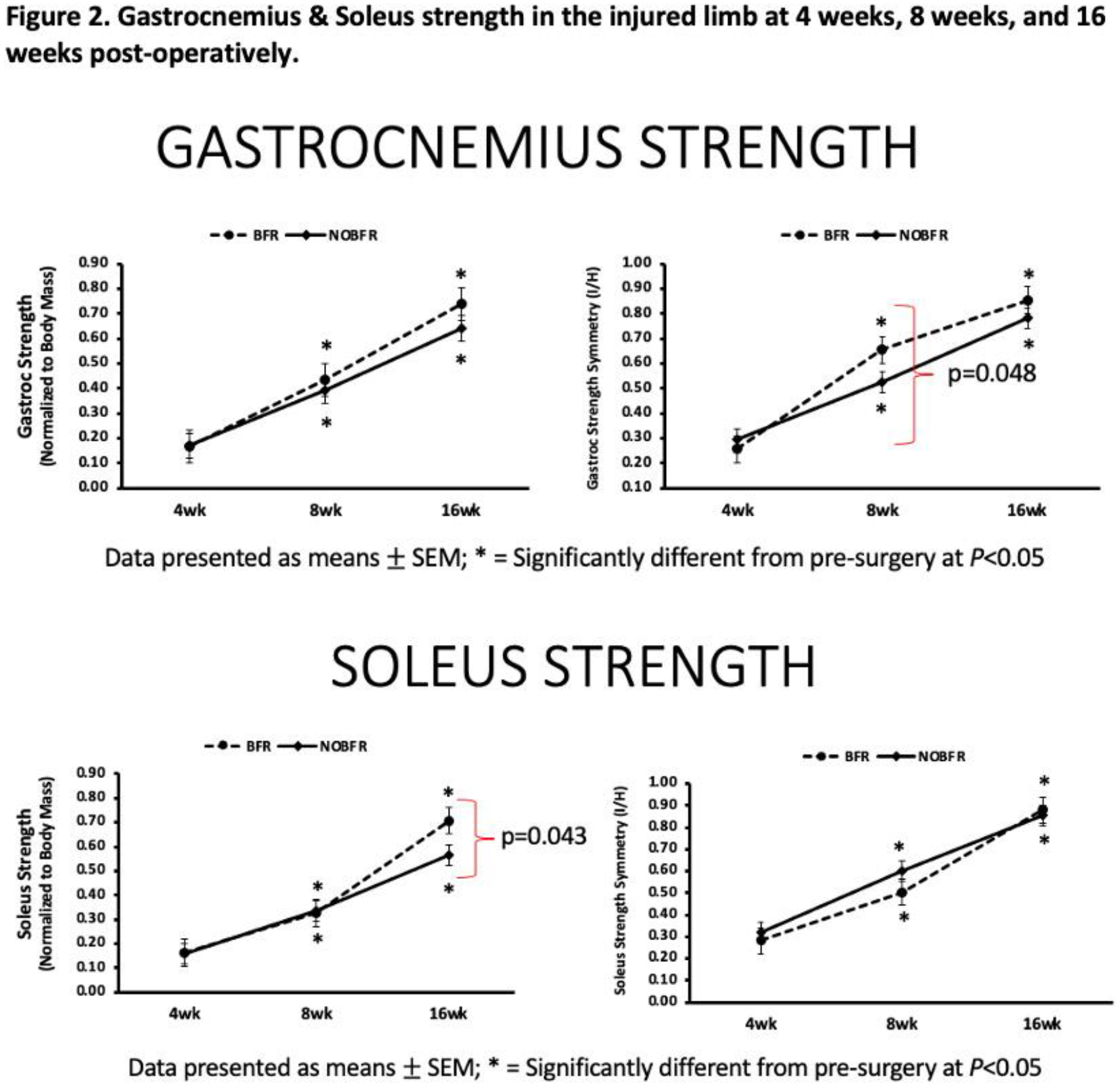
Only the control group was observed to have lower extremity bone mass loss in the injured limb at the 8wks postoperative (p=0.006) and 16wks postoperative (p<0.001) timepoints (Figure 1). Compared to the control group, the BFR group was observed to have preserved tibia BMD at 16wks postoperative (p=0.016) whereas the control group experienced a significant decrease at 16wks compared to preoperative (p=0.003) (Figure 1). Both groups were observed to have similar increases in gastrocnemius strength at the 8wks (BFR: p=0.004; control: p<0.001) and 16wks postoperative (BFR: p=0.002; control: p<0.001)(Figure 2). However, there was a greater improvement towards achieving limb symmetry in the BFR group at 8wks postoperative (p=0.048) (Figure 2). The BFR group demonstrated greater improvements in soleus strength at 16wks (p=0.043) compared to 4wks postoperative (Figure 2).
Conclusions:
Preliminary findings suggest that the application of BFR to a standardized rehabilitation protocol following Achilles tendon rupture repair may result in preservation of lower extremity bone mass and tibial BMD, greater recovery of calf muscle strength, and greater preservation of calf muscle mass.