Abstract
Objectives:
This is a cadaveric biomechanical study of remplissage technique for recurrent anterior shoulder instability. Remplissage is a surgical procedure in which the infraspinatus tendon is tenodesed into a bony defect on the humeral head called a Hill-Sachs lesion (HSL). There is substantial variation in remplissage technique between surgeons, suggesting that the number and location of anchors may be critically important to patient outcomes. One clinical question is whether medial anchor placement, which has been shown in biomechanical studies to decrease humeral external rotation, regularly causes clinically significant decreases in shoulder range of motion. There is also uncertainty about how many anchors are necessary for different size Hill-Sachs lesions. Our hypothesis was that two fixation points as well as medial fixation would yield significantly higher peak resistance in both large and small HSL when compared to single fixation and central fixation.
Methods:
Ten cadaveric shoulder specimens were tested with a 6-axis industrial robot (KUKAKR6R700) that is integrated with simVITRO LabVIEW-based control software (Cleveland Clinic). Eleven conditions of the shoulder were tested: (1) intact, (2) 15% HSL, (3) 15% HSL with one central, (4) 15% HSL with 2 central, (5) 15% HSL with one medial, (6) 15% HSL with 2 medial, (7) 30% HSL, (8) 30% HSL with one central, (9) 30% HSL with 2 central, (10) 30% HSL with one medial, (11) 30% HSL with 2 medial. Statistical analysis comparing testing conditions was performed using pairwise paired t-tests with Holm adjustment. A P value < 0.05 was considered significant.
Results:
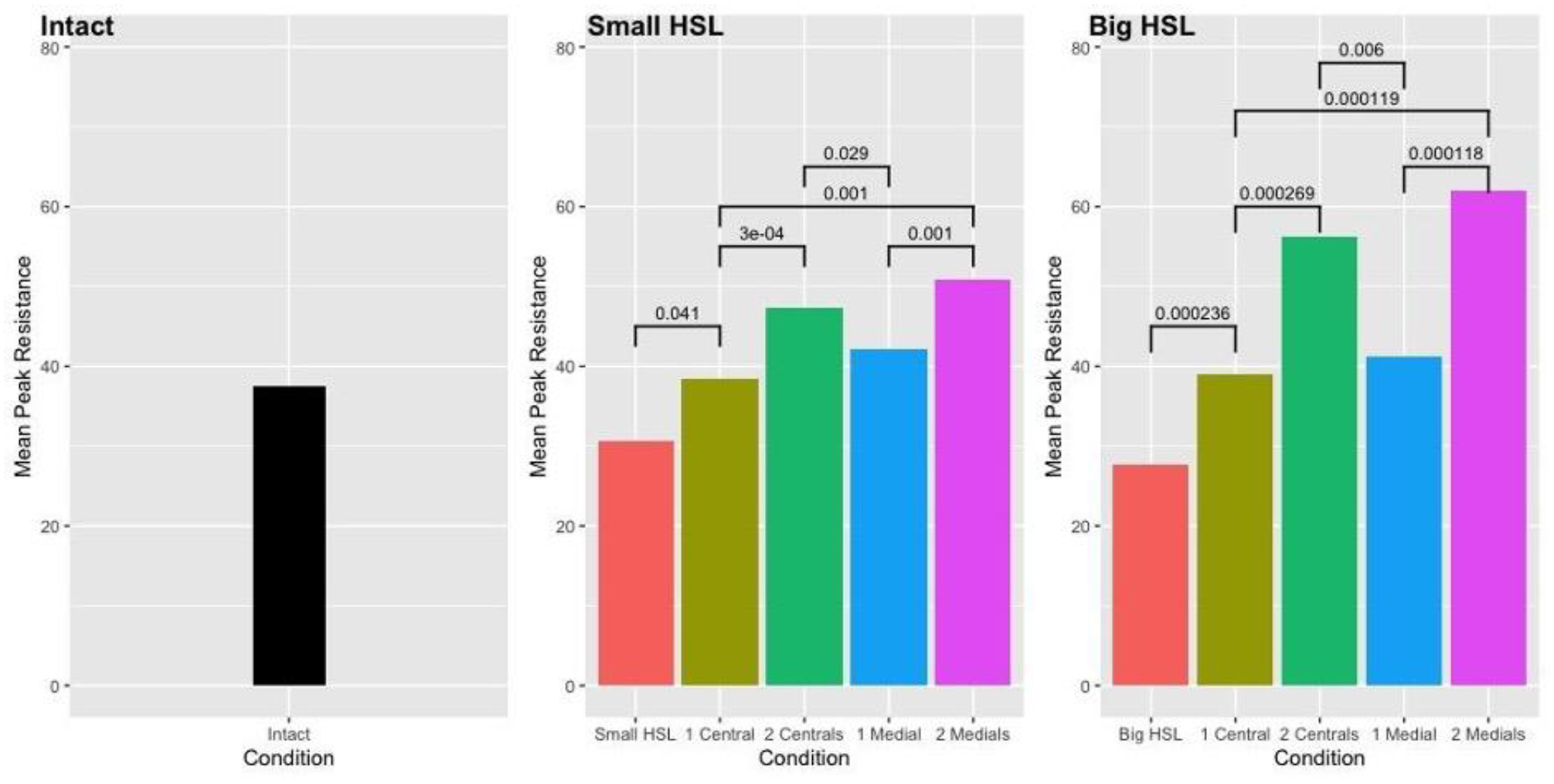
All remplissage techniques tested were able to successfully restore mean peak resistance to anterior translation to at least equal that of the intact shoulder condition (
In the small HSL condition there was not a significant difference in resistance when comparing 1 central to 1 medial (p=0.07) or 2 centrals to 2 medial (p=0.026) fixation points.
Likewise, in the large HSL condition there was not a significant difference in resistance when comparing 1 central to 1 medial (p=0.37) or 2 centrals to 2 medial (p=0.214) fixation points.
Conclusions:
All the remplissage techniques tested restored native stability. The use of 2 fixations points yielded higher resistance to translation than the single for both medial wall and central placement. Importantly, there was not a difference in resistance force between medial wall and central placement for either the single or double fixation configurations. This study did not show medial fixation placement providing greater GH stability and therefore may not be worth the risk of stiffness. Our findings suggest that two central fixation points provide as much or more resistance to anterior translation than either 1 or 2 medial. Future clinical studies will be needed to determine whether the robust tenodesis provided by 2 anchors, either medially or centrally, is worth the risk of potential postoperative stiffness.