
Abstract
Objectives:
Anterior cruciate ligament (ACL) reconstruction remains one of the most common procedures performed on the knee with over 250,000 being performed each year in the United States. Although common, results of ACL reconstructions remain less impressive than would be expected. Getgood et al showed a 40% failure of ACL reconstructions including recurrent ACL tears and continued rotational instability.1 The group found that by adding a lateral extra-articular tenodesis (LET) decreased the failure rate to 25%. Sommerfeldt et al identified recurrent ACL instability as a risk factor for meniscal tears after ACL reconstruction.2 In patients with a medial meniscal tear after ACL reconstruction, the decision to proceed with revision ACL reconstruction is straightforward when the graft is completely torn. However, the best approach for a medial meniscal tear after ACL reconstruction with recurrent rotational instability when the ACL graft is intact or partially torn has not been determined. The purpose of this study was to evaluate clinical outcomes of patients with intact or partially torn ACL grafts with continued rotational instability and a medial meniscal tears treated with revision ACL reconstruction, ACL reconstruction with lateral extra-articular tenodesis (LET) and isolated LET. We hypothesized that an isolated LET would have similar clinical outcomes compared to the ACL and ACL+LET groups at 2 years.
Methods:
A retrospective review was performed of all patients with medial meniscal tears after ACL reconstruction. Patients were included in the study if the ACL graft was intact or partially torn with an exam consistent with residual or recurrent rotational instability. Residual ACL instability was determined by a pivot shift of 2 or more on examination. Patients with a grade 3 Lachman’s and partial ACL tear were treated with ACL reconstruction and not included in the study. Over time, the senior author evolved in the treatment of these patients from ACL reconstruction to ACL reconstruction with LET to isolated LET. Patients were placed into different groups based on which treatment they underwent. Clinical outcomes included recurrent meniscal tears, residual rotational instability and recurrent ACL graft tears. Patient reported outcomes (PROs) included IKDC and Lysholm scores at 6, 12, and 24 months. In athletes, we also calculated the percentage of return to play.
Results:
A total of 47 patients were included in the study including 19 patients in LET group, 12 patients in the ACL+LET group, and 16 patients in the ACL group. The patient demographics between the 3 groups were similar. Ligamentous laxity was identified in 42% of the LET group, 50% of the ACL+LET group and 44% of the ACL group. Partial ACL tears were identified in 63% of the LET group, 75% in the ACL+LET group and 62% of the isolated ACL group. The 6-month International Knee Documentation Committee (IKDC) and Lysholm scores were significantly higher for the isolated ACL group compared to the ACL+LET group and isolated LET groups. However, at the 12 and 24-month follow-up the LET and ACL+LET groups had significantly higher IKDC and Lysholm scores compared to the isolated ACL group (Figures 1 and 2). There was no difference between the LET group and ACL+LET group’s IKDC or Lysholm scores at time point. The ACL group showed a significantly higher percentage of patients with a post operative positive pivot shift (44%) compared to the ACL+LET group (8.3%) and isolated LET group (10.5%) at the 2-year postoperative visit (p=0.02). No difference was seen between the LET and ACL+LET groups with regards to residual pivot shift (p=0.88). Recurrent meniscal tears were significantly higher in the ACL group (31.3%) compared to the LET (5.3%) and ACL+LET (8.3%) groups (p=.04). There was no difference with regards to postoperative graft tearing with 5.3% of LET group, 0% of ACL+LET and 12.5% of the ACL group having a postoperative graft tear. There was a significantly higher rate of return to play in the LET group (90%) compared to the ACL+LET group (71.4%) and ACL group (75%). Return to play at the same or higher level was also significantly higher in the LET group (80%) compared to the ACL+LET (57.1%) and ACL group (50%).
Conclusions:
In patients with partially torn or intact ACL grafts with residual rotational instability and medial meniscal tears, the addition of a LET with or without revision ACL reconstruction leads to improved patient outcomes, a lower rate of residual rotational instability and recurrent meniscal tearing compared to an isolated revision ACL reconstruction. The addition of an ACL reconstruction to LET in patients with intact or partially torn ACL grafts and meniscal tearing did not decrease the rate of residual pivot shift or recurrent meniscal tears compared to an isolated LET. Isolated LET in this patient population leads to a higher return to play and play at same or higher level compared to an isolated ACL revision or ACL revision with LET. Isolated LET in this patient population is an acceptable option.
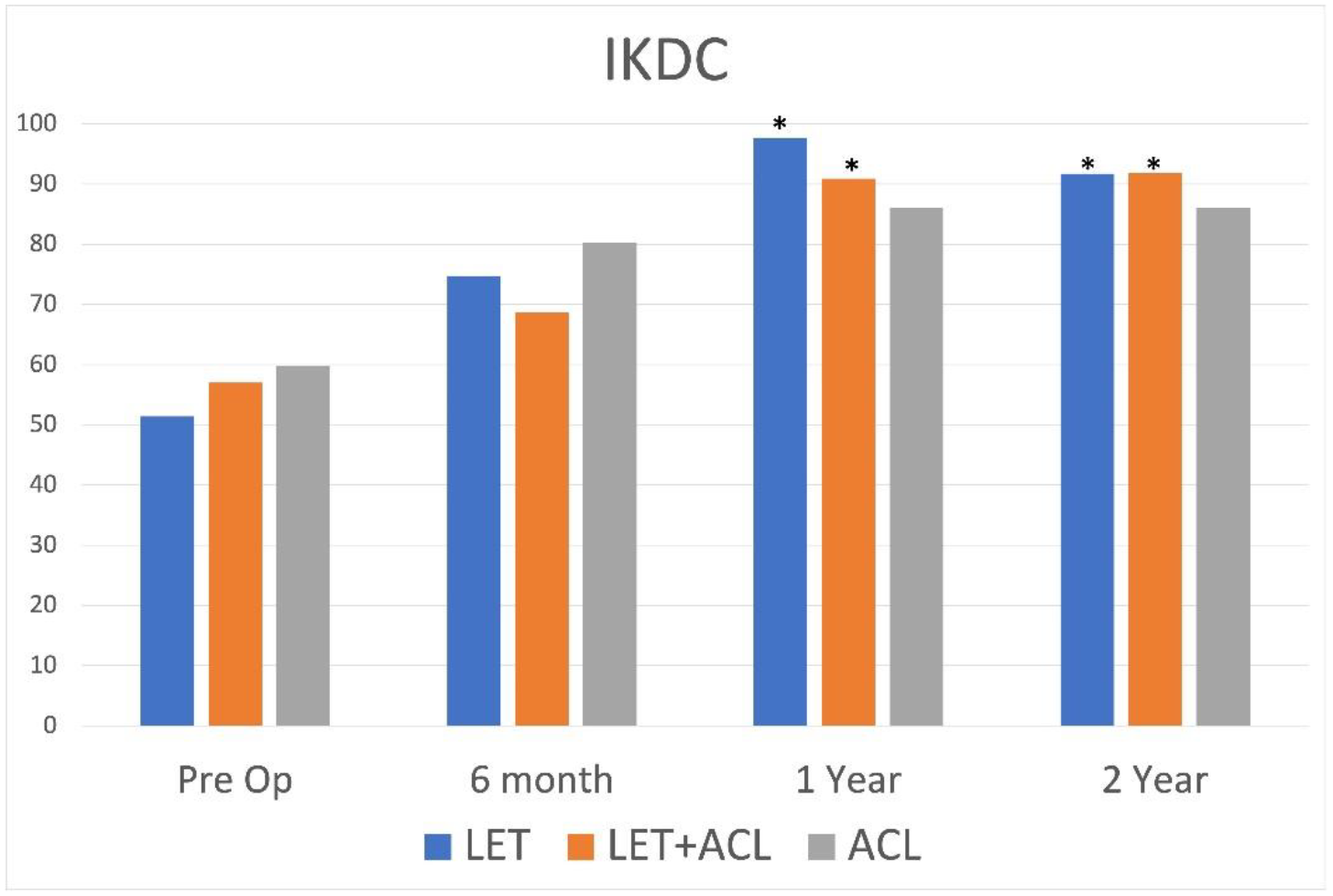
Comparison of International Knee Documentation Committee scores at various stages preoperatively and postoperatively.
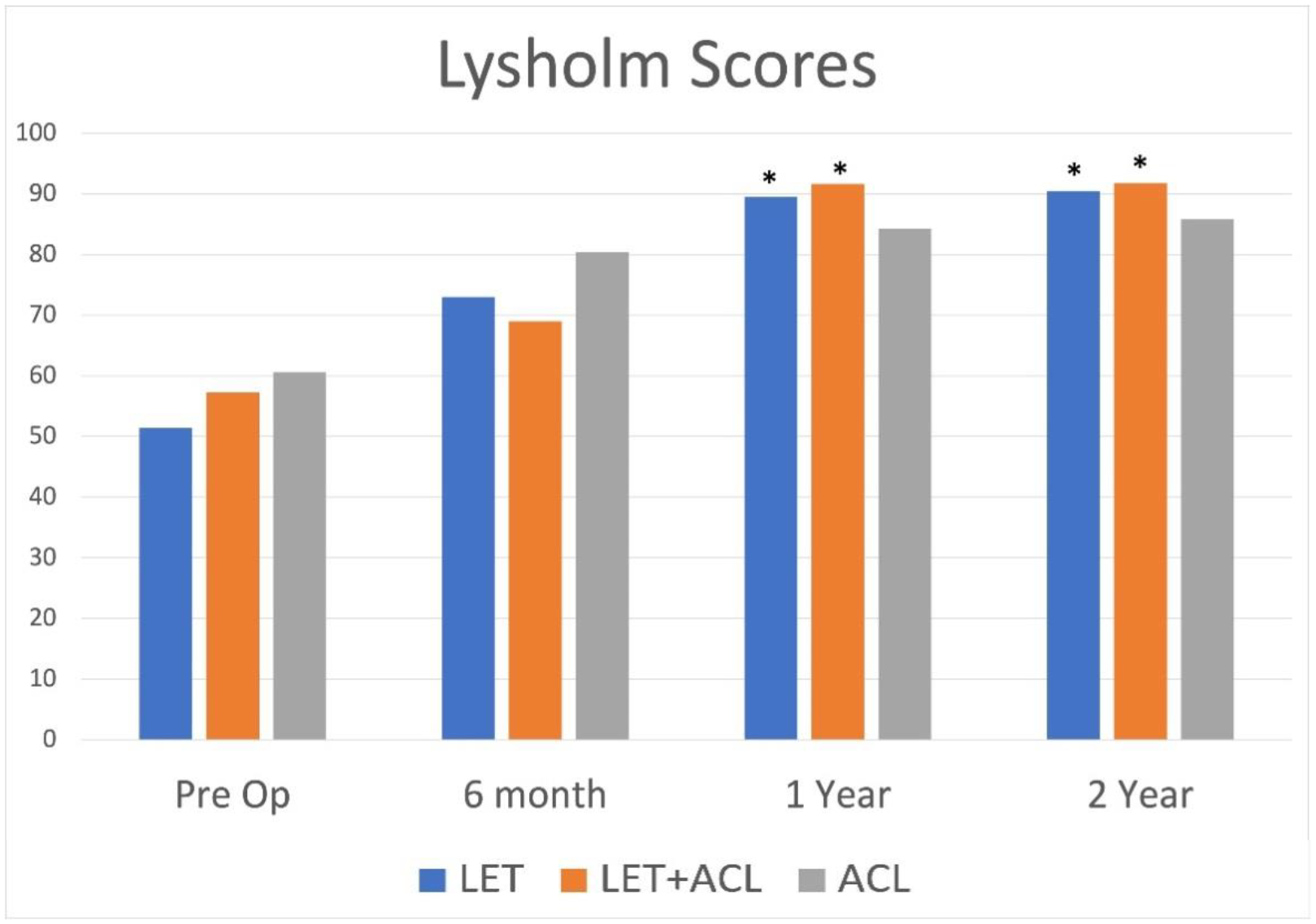
Comparison of Lysholm scores at various stages preoperatively and postoperatively.