
Abstract
Background:
Posterior shoulder instability (PSI) is a multifactorial condition of atraumatic or traumatic onset that most frequently affects young male athletes. To address capsulolabral detachment, arthroscopic posterior capsulolabral repair with suture anchors can be performed.
Purpose:
To report patient-reported outcomes (PROs), failure rates, survivorship, and return-to-sport/activity rates after arthroscopic posterior capsulolabral repair with suture anchors at a minimum of 10 years after surgery.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent arthroscopic posterior capsulolabral repair for PSI by a single surgeon between November 2005 and September 2010 were included; patients with multidirectional instability and concomitant bony reconstruction were excluded. Demographic, surgical, and subjective data were collected prospectively and retrospectively reviewed. PROs that were collected included the American Shoulder and Elbow Surgeons (ASES); Single Assessment Numeric Evaluation (SANE); Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH); and 12-Item Short Form physical component summary (SF-12 PCS) scores. Recurrent instability, dislocations, and reoperations were recorded, and a survivorship analysis was performed.
Results:
Overall, 17 shoulders in 16 patients (all male; mean age, 31.4 years; age range, 19.2-51.2 years) were included. The onset of PSI was atraumatic in 11 shoulders (65%) and traumatic in 6 shoulders (35%). Three patient shoulders (17.6%) underwent revision surgery for instability or osteoarthritis at 6.3, 7.6, and 12.5 years postoperatively. A minimum 10-year follow-up was obtained in 12 of 14 remaining shoulders (86%), with a mean follow-up of 13.1 years. For patients not requiring revision surgery, pre- to postoperatively, the ASES score significantly improved (72.6 to 89.9; P = .016), as did the SF-12 PCS score (43.8 to 55.0; P = .002). The mean postoperative SANE score was 86.9, and the mean postoperative QuickDASH score was 6.6. Median satisfaction was 8 (range, 3-10). At follow-up, 67% of patients had returned to their original fitness program. Kaplan-Meier survivorship analysis showed an 86.7% survival rate at 10 years.
Conclusion:
Study findings indicated that arthroscopic posterior capsulolabral repair was an effective treatment for patients with PSI, albeit with a 17.6% revision rate. Patients who did not require revision had satisfactory PRO scores that were maintained at long-term follow-up.
Keywords
Posterior shoulder instability (PSI) is a multifactorial condition representing approximately 2% to 5% of all detected instabilities. 18 PSI predominantly affects male contact and overhead athletes who experience repetitive microtrauma or blunt force trauma with the shoulder in a position of flexion, adduction, and internal rotation. 5 Posterior shoulder dislocations may also occur in the setting of a seizure disorder. Risk factors include bony abnormalities such as glenoid retroversion, large reverse Hill-Sachs lesions, and specific posterior acromion morphology, as well as soft tissue factors such as joint laxity and weak muscular stabilizers.5,7,20 The condition is often overlooked, resulting in delayed diagnosis and treatment. 5
PSI can be treated nonoperatively, with treatment consisting of physical therapy to strengthen the local dynamic glenohumeral muscular stabilizers such as the deltoid and the rotator cuff, as well as the global stabilizers such as the teres major, rhomboid, serratus anterior, pectoralis minor, trapezius, latissimus dorsi, pectoralis major, and levator scapulae muscles. Nonoperative management is often insufficient in addressing PSI, with 46% of patients treated with physical therapy for at least 1 year requiring operative management within 10 years. 23
Surgical treatment of PSI has expanded over recent years. An epidemiological study found that 87.5% of PSI cases identified between 2009 and 2015 underwent surgical treatment within 5 years, as opposed to 53.1% of cases treated before 2002. 24 Surgical methods to treat PSI have also evolved over the years, with the first description of posterior capsulorrhaphy/capsular plication in 1981, 21 and the posterior Bankart repair described by Hawkins and Janda in 1996. 10 Arthroscopic management of PSI has become increasingly common, although open surgery may be required in cases with substantial bone loss requiring a bone block procedure. Arthroscopic management has demonstrated superior clinical outcomes compared with open treatment and is currently the most widely used approach for addressing soft tissue pathology in PSI. 7
Current evidence for arthroscopic posterior shoulder stabilization is favorable, with low rates of recurrent shoulder instability, good clinical outcomes, and high rates of return to sport.7,19 However, the long-term clinical results and failure rates of arthroscopic management of PSI have not been established.
The purpose of this study was to illustrate clinical outcomes, patient satisfaction, failure rates/survivorship, and return to sport rates/activity at a minimum of 10 years after arthroscopic posterior capsulolabral repair for PSI.
Methods
Study Cohort
This institutional review board–approved study consisted of patients who underwent arthroscopic posterior shoulder stabilization by a single surgeon (P.J.M.) between November 2005 and September 2010. Data were prospectively collected and retrospectively reviewed. Patients were included if they were diagnosed with PSI and treated for a posterior labral tear with arthroscopic capsulolabral repair utilizing suture anchors. Patients received surgery after failed nonoperative therapy. Exclusion criteria included multidirectional instability, bony lesions to the glenohumeral joint requiring reconstruction, concomitant humeral avulsion of the glenohumeral ligament, severe chondrolysis, prior glenohumeral joint fracture fixation, and prior refusal to participate in research. Patient demographic, clinical, radiologic, and surgical information was collected. Revision surgeries and complications were recorded.
PSI was defined as a history of involuntary posterior instability consisting of either dislocation(s) or subluxation(s) in patients without multidirectional instability or underlying hyperlaxity disorders. The diagnosis was determined from clinical evaluation and preoperative imaging and was confirmed intraoperatively as posterior translation of the humeral head over the glenoid rim. Onset of PSI was classified as traumatic or atraumatic based on whether a distinct, traumatic event after which symptoms of shoulder instability began could be identified. Patients were classified based on a review of clinical and surgical reports.
Surgical Technique
Operations were performed by the senior surgeon (P.J.M.) with the patient in the beach-chair position under general anesthesia with an additional interscalene nerve block. The operative extremity was placed in a pneumatic arm holder (Tenet T-Max Beach Chair and Spider arm positioner; Smith & Nephew) and was prepared and draped in the standard fashion. A clinical examination under anesthesia was performed to verify instability using the posterior load and shift test. After standard anterosuperior and posterior portals were established, a diagnostic arthroscopy was performed to confirm the suspected posterior labral tear and identify any concomitant pathology (Figure 1).

Surgical setup, beach-chair position of a right shoulder, with the arthroscope in the anterosuperior working portal. The inset on the left shows an intra-articular view of the posterior labral tear.
An anteroinferior portal was then placed low in the rotator interval with an 8.25-mm cannula (Arthrex). This portal was placed parallel to the glenoid to allow for suture shuttling without inflicting cartilage damage. With the arthroscope in the anterosuperior portal, a posterolateral working portal was then established with a 5-mm cannula 2 cm inferior and 2 cm lateral to the standard diagnostic portal. An 18-gauge spinal needle was first used to ensure that the portal trajectory allowed for access to the entire posterior labrum. Via the posterior working portal, the labrum was then released with an elevator, and an arthroscopic shaver was utilized to create a bleeding surface to optimize healing.
Labral fixation was initiated by using a curved drill guide to drill into subchondral bone on the glenoid face at the 6-o’clock position where the first bioabsorbable suture anchor (SutureTak; Arthrex) was placed. The working suture was then brought out of the anteroinferior portal using a suture grasper. Via the posterior working portal, a crescent-shaped lasso (Arthrex) was passed through the posterior capsule and the chondrolabral junction, where the shuttling wire was retrieved through the anteroinferior portal. The working suture was then loaded into the shuttling wire and passed underneath the labral tissue and through the posterior capsule. Obtaining a large grasp of the posterior capsule functioned to simultaneously shift the posterior capsule and reduce any redundancy in the capsule when the suture was secured utilizing sliding, locking Weston knots. Immediately before labral fixation, a soft tissue grasper was used to shift the labral tissue to its anatomic location. This technique was repeated, typically with 3 additional anchors (4 total), placed from distal to proximal on the glenoid face to help re-create the posterior capsulolabral buttress (Figure 2). Repairs were then tested with a diagnostic examination and arthroscopic probe to confirm adequate fixation. Notably, during the study period, posterior labral repairs were performed with knotted suture anchors. Contemporarily, the senior author's (P.J.M.) preference is to use knotless all-suture anchors (1.8-mm FiberTak; Arthrex) given their biomechanical profile and ease of use.13,14
Intra-articular view from the anterosuperior viewing portal of the repaired posterior labral tear. Three knotless suture anchors were placed, firmly securing the capsulolabral complex.
Postoperative Rehabilitation
Postoperatively, patients were placed in a pillow sling for 6 weeks. Physical therapy was initiated on postoperative day 1 with full passive range of motion except for internal rotation, which was limited for 1 month. Patients were then advanced to full active range of motion. Strengthening and stabilization exercises were initiated 6 weeks postoperatively. Strengthening and range of motion were advanced, with a return to full activity expected by 4 months after surgery. 9
Patient-Reported Outcomes
A minimum 10-year follow-up was obtained by electronic questionnaire and compared with preoperatively collected patient-reported outcomes (PROs). PROs utilized in this study included the American Shoulder and Elbow Surgeons (ASES) score; Single Assessment Numeric Evaluation (SANE) score; Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) score; and the 12-Item Short Form physical component summary (SF-12 PCS) score. Patient satisfaction with outcomes was also assessed (1-10; 10 = highly satisfied). Complications and further surgical interventions were recorded. Additional questions were asked regarding return to physical activity/sports and ability to use arm painlessly. If patients had not returned their annual questionnaires after 10 years, they were contacted regarding elective participation in the study. After informed consent was obtained, an electronic questionnaire was sent via email. No PROs were assessed via telephone.
Patient questionnaires collected into the database before the year 2013 did not include QuickDASH and SANE scores, so only ASES and SF-12 PCS scores were available for both pre- and postoperative time points.
Statistical Analysis
Means and standard deviations were calculated for continuous variables, as were medians and ranges for discrete variables. Categorical data are reported as numbers with percentages. The Kolmogorov-Smirnov test was used to determine the normality of distribution. For normally distributed variables, an independent or paired t test was used. A Wilcoxon signed-rank test was used for nonparametric data. Survivorship analysis was performed using Kaplan-Meier survival curves, with failure defined as (1) progression to subsequent shoulder surgery for recurrent instability or osteoarthritis or (2) recurrent shoulder dislocation. The level of significance was set at a P value <.05.
Results
Study Population
Sixteen male patients (17 shoulders) who underwent arthroscopic posterior stabilization were included in this study. The onset of PSI was atraumatic in 11 shoulders and traumatic in 6 shoulders. No differences between traumatic or atraumatic onset were found for age at surgery (P = .683). Three patients had prior ipsilateral shoulder surgeries, including 2 prior superior labral anterior-posterior (SLAP) repairs and 1 prior posterior capsulolabral repair for PSI. Demographic and injury data are depicted in Table 1.
Cohort Characteristics and Injury Data (N = 17 Shoulders) a

Data are presented as No. of shoulders (%) unless otherwise indicated.
The study cohort included 3 professional athletes (2 golfers and 1 baseball player) and 1 collegiate shortstop athlete. Eight patients participated recreationally in softball, hockey, swimming, climbing, snowboarding, wakeboarding, golf, or gym exercises/general fitness. Two patients did not report recreational athletic activity. Both of these patients worked as underground coal miners, a profession involving repetitive overhead lifting of heavy loads. Sports and activity participation was not known for the remaining 2 patients.
Operative Findings
Intraoperative assessment of posterior translation revealed mild instability (0-1 cm of translation) in 3 shoulders, moderate instability (1 to 2 cm of translation, or translation to the glenoid rim) in 5 shoulders, and severe instability (>2 cm of translation, or translation over the glenoid rim) in 9 shoulders. No shoulders were locked out over the rim of the glenoid.
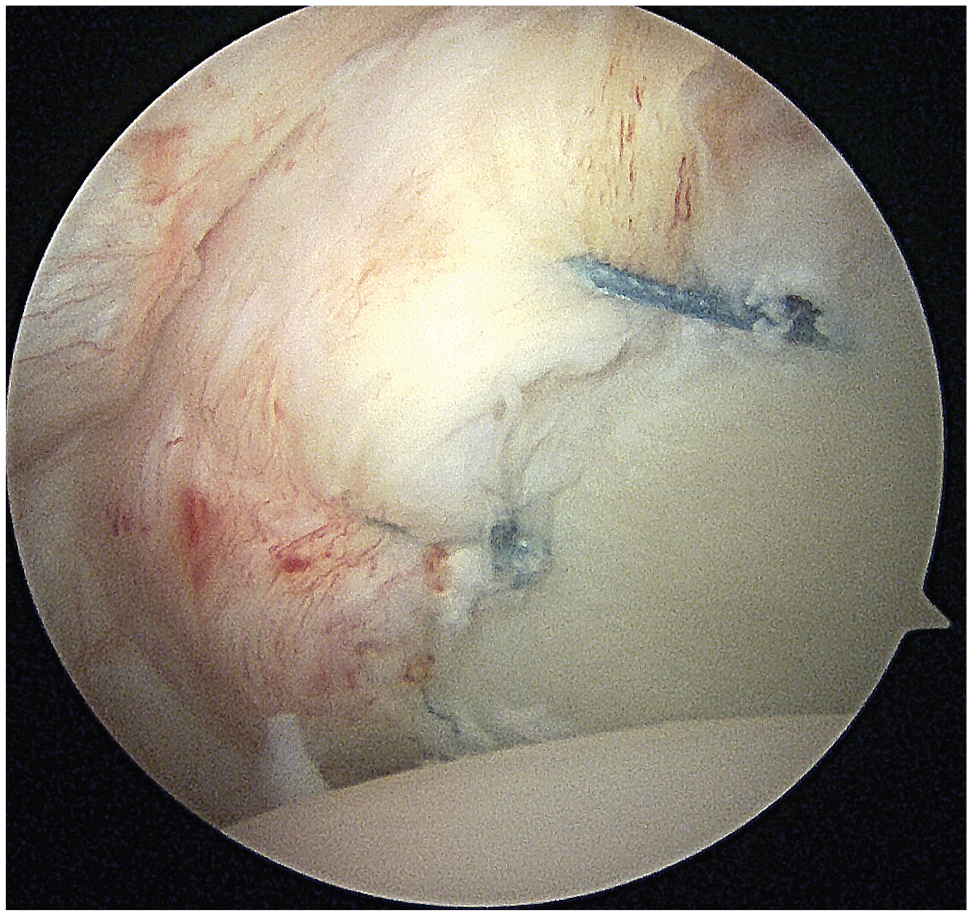
Intraoperatively, a posterior labral tear was seen in all patients (Figure 3). The majority of shoulders (n = 13) had a SLAP tear requiring repair (Figure 4). Focal chondral defects were detected on the glenoid 2 shoulders; both patients received additional microfracture treatment. In 1 patient, the biceps tendon was affected. The patient received additional biceps tenodesis. All additional procedures are listed in Table 2.

Posterior labral tear in a right shoulder with the arthroscope placed through the anterosuperior viewing portal.

Intra-articular view from the posterior viewing portal showing a concomitant grade 1 superior labral anterior-posterior lesion.
Procedures Performed in Addition to Posterior Capsulolabral Repair a

SLAP, superior labral anterior-posterior.
Clinical Outcomes
Of the 17 shoulders included in this study, 17.6% required additional surgery, either for recurrent instability (2 shoulders) or progression of arthritis (1 shoulder). Patients who underwent subsequent surgeries were excluded from the PRO analysis. Follow-up data were collected for 12 of the remaining 14 shoulders (86%) (Figure 5).

Flow diagram of the study cohort involved in clinical outcome evaluation (n = 12 shoulders). CAM, comprehensive arthroscopic management; HAGL, humeral avulsion of the glenohumeral ligament; ORIF, open reduction and internal fixation; PSI, posterior shoulder instability; TSA, total shoulder arthroplasty.
Clinical outcome scores for the patient cohort are illustrated in Table 3. The mean 10-year postoperative ASES score was 89.9 ± 15.6, which was a significant improvement from the preoperative baseline score of 72.6 ± 19.6 (P = .016). The mean SF-12 PCS also improved from preoperatively to postoperatively (from 43.8 ± 8.5 to 55.0 ± 4.8; P = .002). No differences were seen between traumatic or atraumatic onset for postoperative ASES (P = .561), SF-12 PCS (P = .284), QuickDASH (P = .403), or SANE (P = .729) scores.
Preoperative and Postoperative Clinical Outcome Scores a

Data are presented as mean ± SD or median (range). Patient questionnaires collected into the database before the year 2013 did not include QuickDASH and SANE scores. ASES, American Shoulder and Elbow Surgeons; NA, not available; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand; SANE, Single Assessment Numeric Evaluation; SF-12 PCS, 12-Item Short Form Physical Component Summary.
At the minimum 10-year follow-up, patients’ ability to participate in usual sports and recreational activities had improved from preoperatively (P = .026 and .016, respectively). The majority of patients (7/12) reported being able to painlessly lift their arms to the level of their heads. Self-reported ability to throw a ball 20 yards (18.3 m) significantly improved from preoperative evaluation (P = .010). Eight of 12 patients (67%) reported being back at their preinjury fitness program. Four patients reported modifying their recreational sport/activity for the following reasons: pain (3 patients), weakness (3 patients), feelings of instability (2 patients), and fear of reinjury (2 patients).
Complications and Failures
No intraoperative complications occurred. Three patients (3 shoulders; 17.6%) failed and required subsequent surgeries. Two patients underwent revision arthroscopic surgery for PSI. One of these patients was initially asymptomatic, but subsequently developed recurrent instability while bicycling, weightlifting, and conducting activities of daily living at 9 years postoperatively. He underwent revision surgery with distal tibial allograft augmentation. The other patient had bilateral shoulder surgeries for PSI performed by the senior author. One of his shoulders required revision surgery at 8 years postoperatively for recurrent posterior instability, and the other shoulder did not experience recurrent instability. A third patient, age 51 years at the index surgery, had 2 subsequent surgeries to address osteoarthritis. This patient underwent comprehensive arthroscopic management (CAM) 6.4 years after the initial procedure, followed by conversion to total shoulder arthroplasty (TSA) at age 62 years for grade 4 osteoarthritis. Given the patient's history of residual instability, early posterior glenoid wear is a possibility.
One patient reported prolonged postoperative physical therapy. In the follow-up surveys, no subsequent surgeries or dislocation events were reported. However, it should be stated that both the 10-year and 11-year surveys showed decreasing PRO scores.
Based on the time points of the 3 known failures, a Kaplan-Meier survivorship analysis yielded an 86.7% survival rate at 10 years.
Discussion
Clinical Outcomes
The findings of this study demonstrated favorable clinical outcomes but a 17.6 % failure rate after arthroscopic posterior stabilization with follow-up at a minimum of 10 years and a mean of 13.1 years. The patients who did not require revision demonstrated a significantly improved mean ASES score from 72.6 at baseline to 89.9 at final follow-up. Additional improvement was seen in the SF-12 PCS score, a widely used and validated scale of physical health. Postoperative SANE and QuickDASH scores were favorable at 86.9 and 6.6, respectively.
The results of this long-term study are quite promising for the durability of arthroscopic surgery for PSI, as they are comparable to outcomes reported in studies with short- to midterm follow-ups. A minimum 1-year follow-up study of 96 athletes, including throwers and nonthrowers, reported a mean postoperative ASES score of 89.5, 15 similar to the results in the current study. Katthagen et al 11 reported a slightly higher postoperative mean ASES score of 95.8 at a minimum 2-year follow-up. In their study, SANE, QuickDASH, and SF-12 scores only improved in traumatic cases. Another minimum 2-year study of 22 shoulders with PSI reported a postoperative SANE score of 85 and ASES score of 83, 12 slightly inferior to the results in the current study. This study did not reveal any differences in patients treated for anterior, posterior, or combined shoulder instability. 12 Asturias et al 2 also reported inferior clinical outcome scores at a minimum 2-year follow-up with a mean SANE score of 78.59 and a QuickDASH score of 17.15. However, their study solely included adolescent patients, a population known to have inferior outcomes after instability surgery. Finally, Bradley et al 4 reported on 149 patients with a minimum follow-up of 4.1 years and a mean follow-up of 13.0 years, nearly identical to the mean follow-up in the current study. In patients who did not require revision surgery, they found that the mean ASES score at follow-up was 87.8, similar to our results. Overall, clinical results reported in the literature were good to excellent postoperatively during all time frames.
Patients in the present study were stratified as having traumatic or atraumatic onset PSI. No differences were seen with regard to patient characteristics or outcomes between the 2 groups. However, it is not possible to draw conclusions from these results because of the small cohort size. Also, because of the small cohort, a possible influence of SLAP tears could not be analyzed. Atraumatic PSI has been previously shown to be associated with higher degrees of glenoid retroversion and inferior outcomes after arthroscopic surgery for PSI. 11
Return to Activity
As PSI is a condition that predominantly affects active individuals, a primary goal for surgery is returning patients to athletic participation and restoring function during activity. The current cohort included active patients, with many patients participating in professional or recreational sports involving overhead motion before injury. However, because the cohort was not limited to patients participating in organized sports, we assessed return to fitness activity in lieu of return to sport. The results showed that 67% (8/12) of patients were successfully able to return to their preinjury activity. However, it should be mentioned that 5 of 12 reported pain with lifting their arm to the level of their head.
Definitions for return to play or return to activity vary within the literature, making it challenging to compare across studies. However, a 2021 systematic review 8 that included 25 short-term outcome studies of arthroscopic stabilization for PSI concluded that overall return-to-play rates were between 62.7% and 100.0%, with 50.0% to 100.0% returning to the same level of play. These results are promising, particularly considering that many patients being treated for PSI are overhead or contact athletes who undergo repetitive, extreme stress on their shoulders. Combined with the results of the current study, surgeons can advise their patients that there is a good chance for active patients to be able to return to their previous level of activity, and they can expect to be able to remain active in the long term. Additionally, patients treated arthroscopically for PSI are not at a disadvantage for return to play compared with patients treated for anterior or combined instability. 12
Failures and Survivorship
The current study demonstrated a failure rate of 17.6%, with an 86.7% survival rate at 10 years as determined by a Kaplan-Meier survivorship analysis. The 3 patients who were considered failures all underwent subsequent shoulder surgery for recurrent instability or osteoarthritis. Those who did not progress to revision surgery reported stable shoulders, with no reported dislocations and only 1 case of recurrent subluxations that resolved with physical therapy.
The failure rate of the current cohort is similar or slightly inferior to the rates reported in the literature for short- to midterm studies. In a cohort of 22 PSI patients from the Norwegian Register for Shoulder Instability Surgery, 2 patients (8%) underwent revision surgery, and 4 patients (16%) experienced recurrent instability at the 1-year follow-up. 3 In a study of 65 high-risk military patients, only 1 (1.5%) required revision surgery at a minimum 2-year follow-up; however, 10 (15.4%) were deemed to have experienced clinical failure due to persistent pain that prevented return to active duty. 6 Other minimum 2-year outcome studies have reported revision rates of 4.9% 11 and 8.2%. 22 With a longer-term follow-up of a minimum of 4 years and a mean of 13 years, Bradley et al 4 found a revision rate of 5.4% after arthroscopic posterior capsulolabral repair. Although the failure rate of 17.6% in the current study is higher than the previously reported rates for revision, it is important to note that the failure rate included a patient treated with a subsequent arthroscopic CAM procedure followed by a TSA for shoulder osteoarthritis. This patient was 58 years old at the time of the first subsequent surgery. It is unknown whether the development of osteoarthritis after arthroscopic surgery for PSI was due to recurrent instability events or natural aging. Additionally, all revisions in this study occurred after 6 years, indicating that shorter-term studies may not be fully descriptive of the true revision rates after PSI. Despite the 3 failures that occurred, the 86.7% survivorship at 10 years indicates that arthroscopic posterior capsulolabral stabilization is a long-lasting option for the complex condition of PSI. It should be mentioned that the study cohort did not have any military patients or patients participating in American football. Both are known to be potential risk factors for PSI.
A complete risk factor analysis was not feasible given the small number of patients in this study. Risk factors for failure after arthroscopic surgery for PSI have been reported to include small glenoid width/glenoid bone loss,1,4 younger age, 2 and female sex.2,22 The current study did not include adolescent patients, so the results may not be applicable to this demographic. Younger patients may be at risk of treatment failure after arthroscopic shoulder instability, as evident by a study of 48 adolescent patients (mean age, 16.5 years), in which 31.3% of surgeries were considered failures, as defined by progression to revision surgery or persistently low postoperative outcome scores. 2 However, a study of 68 adolescent athletes with 81 shoulders found a low failure rate of 8.5% at a minimum of 2 years after PSI surgery, comparable to the failure rates seen in the adult population. 16 This study involved only male patients, similar to the current study. Although the male predominance in PSI research is representative of the patient population with this condition, the lack of female patients may influence the results in the positive direction.2,22 Further studies are needed to determine how female patients treated for PSI fair at long-term follow-up.
Limitations and Strengths
The main limitation of this study was the inability to assess a large cohort of patients because of the rare incidence of PSI and the long-term follow-up design of the study. This was compounded by the lack of preoperative data available for SANE and QuickDASH scores, limiting analysis for these 2 questionnaires. The small cohort size limited the ability to perform subanalyses in this study. A subanalysis of traumatic versus atraumatic patients was performed; however, the finding of no significant differences in outcomes between the 2 groups may have been a type 2 beta error. Given the individuality of each case, there was no specific time frame for nonoperative management before surgery.
Despite these limitations, the results from this study are valuable for understanding the durability and effectiveness of arthroscopic posterior shoulder stabilization. To our knowledge, this is the first minimum 10-year outcome study for this procedure. Most of the cohort was represented in the study's results, as 86% of the eligible patients had follow-up scores available. Finally, the procedures were all performed by a single surgeon at a single facility, minimizing confounding variables.
Conclusion
Study findings indicated that arthroscopic posterior capsulolabral repair was an effective treatment for patients with PSI, albeit with a 17.6% revision rate. Patients who did not require revision had satisfactory PRO scores that were maintained at long-term follow-up.
Footnotes
Final revision submitted August 9, 2024; accepted August 30, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was partially funded by a philanthropic donation from Paul and Lee Schmidt. The study was also supported by the Steadman Philippon Research Institute (SPRI), which is a 501(c)(3) nonprofit institution supported financially by private donations and corporate support. SPRI exercises special care to identify any financial interests or relationships related to research conducted here. During the past calendar year, SPRI has received grant funding or in-kind donations from Arthrex, Canon, DJO, Icarus Medical, Medtronic, Ossur, Smith & Nephew, SubioMed, Stryker, and Wright Medical. R.O.D.H. has received research support from AGA. M.V. has received grant support from Arthrex, education payments from Arthrex and Smith & Nephew, and hospitality payments from Stryker. P.J.M. has received consulting fees and nonconsulting fees from Arthrex, royalties from Arthrex and MedBridge, and has stock/stock options in VuMedi and Game Ready. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Vail Health (reference No. 2021-104).