
Abstract
Background:
The rates of surgeries for ulnar collateral ligament (UCL) injuries continue to rise for baseball pitchers. The physical size of pitchers has also increased, bringing into question whether today’s larger pitchers have proportionally bigger and stronger UCLs able to withstand greater elbow varus torque. Furthermore, controversy exists in biomechanics literature regarding whether kinetics during pitching should be reported as torque (in N·m) or normalized torque (scaled by body weight and height).
Hypothesis/Purpose:
The purpose of this study was to quantify the relationships between body size and mechanical properties of the UCL measured directly on cadaveric specimens. It was hypothesized that greater body weight and height would correlate with greater UCL strength, stiffness, and cross-sectional area.
Study Design:
Descriptive laboratory study.
Methods:
UCL thickness and length were measured by ultrasound for 20 cadaveric right elbows from young adult (mean age, 33 ± 6 years) male donors. Each elbow was then dissected, potted, and placed into a mechanical test frame at 90° of flexion. The specimen was then tested to failure at a rate of 1° of valgus rotation per second. Correlations between geometric and biomechanical data were tested by linear regressions (P < .05).
Results:
The mean UCL failure torque was 45.0 ± 10.5 N·m, and the mean stiffness was 2.72 ± 0.48 N·m/deg. Correlations between failure torque and height (P = .25), weight (P = .85), and height × weight (P = .72) were nonsignificant. Similarly, stiffness showed no significant correlation with height (P = .24), weight (P = .21), or height × weight (P = .18). UCL cross-sectional area did not significantly correlate with body height (P = .34), height × weight (P = .064), or weight (P = .065).
Conclusion:
Body size is not correlated with UCL strength and stiffness.
Clinical Relevance:
Clinicians should not assume that bigger athletes have a stronger UCL. Furthermore, elbow varus torque during throwing for adult athletes should not be normalized by body weight and height.
The rates of ulnar collateral ligament (UCL) injuries and surgeries continue to rise for baseball pitchers.6-8,22,29,30 The physical size (height and weight) of pitchers has also continued to increase over the years, bringing into question whether today’s larger pitchers have proportionally bigger and stronger UCLs able to withstand greater elbow varus torque. 19 Numerous biomechanical studies have reported elbow varus torque during pitching; however, controversy exists on how pitching kinetics should be reported. 17 Some studies have reported pitching elbow varus torque in absolute units (eg, N·m),5,13,14,16,33 others have reported unitless normalized elbow varus torque (ie, torque divided by body weight and height),9,23 and still others have reported both absolute and normalized values of elbow varus torques.10,11,15,25 If UCL strength is proportional to body size, then normalizing elbow torque in pitching is warranted; however, if UCL strength is not correlated with body size, the absolute value of elbow torque in pitching is the better choice for comparing different pitchers.
Understanding whether UCL strength is related to body size is also vital information for orthopaedic surgeons, physical therapists, and other clinicians treating baseball players. Current surgical techniques and rehabilitation modalities do not consider body size in UCL strength and injury treatment; however, if UCL strength were proven to be proportional to body size, perhaps surgical and rehabilitative treatments should be individualized for bigger or smaller athletes.
The purpose of this study was to quantify the relationships between body size and mechanical properties of the UCL measured directly on cadaveric specimens. We hypothesized that greater body weight and height would correlate with greater UCL strength, stiffness, and cross-sectional area.
Methods
Cadaveric Specimens
Twenty unmatched fresh-frozen cadaveric right upper extremities from adult male donors 40 years of age or younger were procured and allowed to thaw to room temperature for approximately 24 hours before the beginning of the experiment. Our institution did not require institutional review board review or approval for cadaveric studies. This age range was intended to be representative of the throwing athlete population of interest. Because roughly 90% of the general population is right-handed, 26 most right arms can be assumed to be dominant. Hence, only right arms were selected to reduce any effects of arm dominance. Donor height and weight were provided by the vendor (Science Care) and documented for later analysis (Table 1). Donor causes of death were noted to be largely (17/20) sudden and/or traumatic (ie, cardiac arrest, drug toxicity, blunt force, and gunshot). The remaining causes of death (3/20) were due to seemingly prolonged illness/disease (eg, diabetes, liver failure, and enlarged heart).
Specimen Characteristics a

BMI, body mass index.
Geometric Measurements
Before dissection, geometric measurements of the UCL were made under direct sonographic visualization. A Samsung HS60 ultrasound machine with an LA4-18BD linear probe (Samsung/Neuro Logica Corp) was used by a sports medicine physician with 13 years of experience with musculoskeletal ultrasound (R.E.C.) to noninvasively assess UCL thickness and length (Figure 1). Thickness was defined as a line beginning from the lateral/deep origin of the medial epicondyle and ending at a point perpendicular to the overall medial/superficial length, similar to a previous study. 20 This was later used for calculation of cross-sectional area. Sonographic measurements were recorded with the specimen’s elbow stabilized at 90° of flexion to ensure repeatability.

Ultrasound image of a right elbow. The 5 measurements illustrated are (1) length of the medial epicondyle origin, (2) medial-side length from origin to insertion, (3) distance between medial and lateral insertion points on the sublime tubercle, (4) lateral-side length from origin to insertion, and (5) ulnar collateral ligament thickness.
Dissection
After ultrasound, the humerus and forearm were transected at the mid-diaphysis. With the forearm in neutral rotation, the ulna and radius were drilled and fixated with a quadricortical screw to maintain neutral forearm position during subsequent biomechanical testing. A medial incision was created just posterior to the medial epicondyle. The cubital tunnel was then exposed and the sublime tubercle and medial epicondyle were identified. For UCL exposure, a muscle-elevating approach was utilized to dissect and elevate the flexor-pronator musculature off the anterior band of the UCL.2,4 The ulnar nerve was excised to allow for complete visualization of the ligament. The lateral elbow was not dissected so as to not disrupt the lateral ligamentous complex. Ligament width was not able to be reliably measured via ultrasound, so with the elbow once again at 90° of flexion, width was measured with a digital caliper at the medial epicondyle, midsubstance, and sublime tubercle. The midsubstance caliper width measurement was multiplied by the corresponding thickness measurement from the ultrasound procedure to calculate a single overall cross-sectional area measurement.
Biomechanical Testing
Once initial dissections were completed, the humerus and forearm were potted in an acrylic pipe using polymethylmethacrylate. Each specimen was then secured into a custom test fixture that we have used extensively21,28 and mounted into an MTS 858 MiniBionix II servohydraulic mechanical test frame (MTS Systems) at a fixed elbow flexion angle of 90° (Figure 2). Biomechanical testing in the intact condition was conducted by commanding the test frame actuator in torque control to internally rotate the humerus while holding the forearm stationary, creating a valgus torque on the medial elbow. A 2-N·m valgus preload was applied, followed by 10 cycles of valgus joint torque between 2 and 10 N·m to provide a consistent strain history as well as to precondition the soft tissues. This range was chosen based on a previous study, 12 to fall well within the physiological (ie, elastic) range of the joint. At the completion of these subfailure cycles, a return-to-zero command was followed by a constant torque-to-failure test in rotation control at a rate of 1 deg/s as in previous studies.21,28 Failure was defined as both the sudden appearance of a visible defect in the tissue and a concurrent dramatic decrease in the real-time torque-rotation curve. Failure torque was defined as the torque at the instant of failure. Stiffness was calculated as the slope of the linear region of the torque-rotation curve.
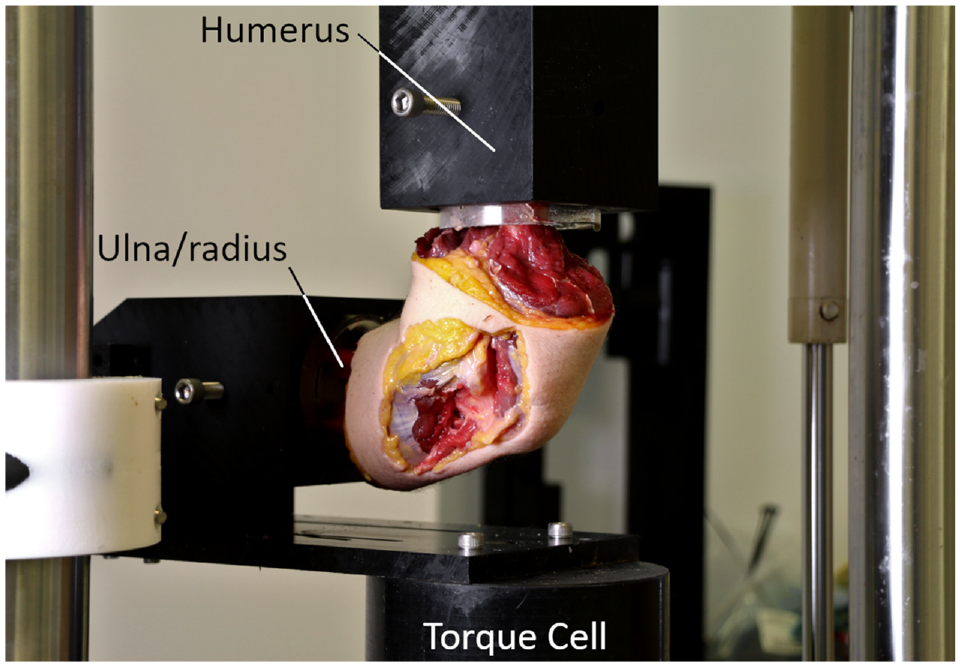
Biomechanical test setup with a right elbow joint fixed at 90° of flexion. The humerus is attached to the test frame actuator, which rotates to create a valgus torque in the elbow, measured by the torque cell attached to the ulna/radius.
Statistical Analysis
Geometric and biomechanical data from all 20 specimens were analyzed via individual linear regressions to test for correlation with height and weight. Correlation coefficients were calculated and significance was set at a P value < .05.
Results
Failure Modes
Of the 20 specimens tested under valgus torsion, 18 failed at the UCL, while 2 specimens failed via humeral fracture. Failure strength data were not used for the latter; however, their native geometric properties (ie, cross-sectional area) and subfailure mechanical properties (ie, stiffness) were used for analysis. Of the 18 UCL failures, 7 (39%) failed near the medial epicondyle, 6 (33%) failed near the sublime tubercle, and 5 (28%) failed in the midsubstance (Figure 3).

Midsubstance failure of a right ulnar collateral ligament (UCL) subjected to a constant elbow valgus rotation.
Biomechanical Properties
UCL failure torque (n = 18) resulting from valgus rotation of the elbow at 90° of flexion was 45.0 ± 10.5 N·m (Table 2). Stiffness (n = 20) during the torque-to-failure test was 2.72 ± 0.48 N·m/deg. Linear regression showed no significant correlation (P≥ .25; R≤ 0.28) between failure torque and height, height × weight, weight, or body mass index (BMI). Similarly, stiffness during the torque-to-failure test showed no significant correlation (P≥ .18; R≤ 0.31) with height, height × weight, weight, or BMI.
UCL Parameters a
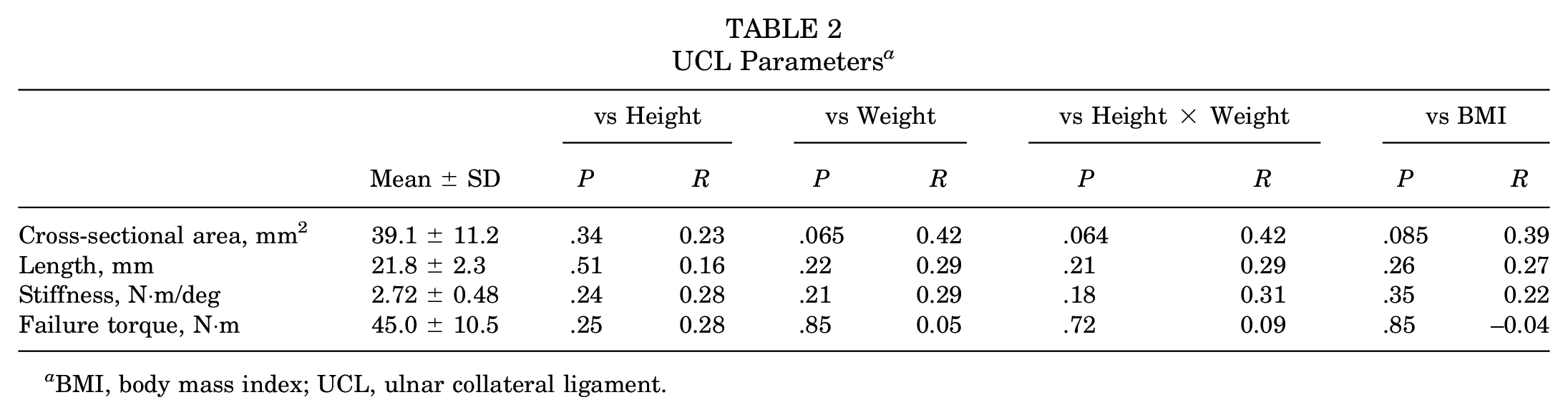
BMI, body mass index; UCL, ulnar collateral ligament.
Geometric Properties
The calculated UCL cross-sectional area (n = 20) was 39.1 ± 11.2 mm2 (Table 2). The mean medial-side and lateral-side lengths of the UCL were 27.6 ± 3.7 mm and 20.6 ± 1.9 mm, respectively; the mean length was calculated to be 21.8 ± 2.3 mm (Table 2). Linear regression showed cross-sectional area to have no relationship with height (P = .34; R = 0.23) and a trend toward correlation with height × weight (P = .064; R = 0.42), weight (P = .065; R = .42), and BMI (P = .085; R = 0.39). There was no significant relationship (P≥ .21; R≤ 0.29) between mean length with height, height × weight, weight, or BMI.
Discussion
Contrary to our hypothesis, native UCL cross-sectional area did not significantly correlate with donor height, weight, height × weight, or BMI. This finding is in contrast to findings from recent clinical studies, which positively correlated patient height with various tendon diameters.3,24,31 It is conceivable that differences between tendons and ligaments could account for this discrepancy; however, a more likely explanation is that the previous studies used tendons from the lower extremities, which may have been developmentally affected by body weight inherently more than the upper extremity, nonweightbearing ligament in the present study.
Furthermore, our hypothesis that UCL strength and stiffness are correlated with body size was not supported by the data. To our knowledge, there have been no previous studies investigating in vitro failure torque of the elbow as it relates to the donor’s anthropometry. Previous experiments have shown failure torques ranging from 19 to 34 N·m for the native UCL.1,18,32 Our mean failure torque of 45 N·m was higher than this range, possibly because of differences in test factors between studies such as magnitude of elbow flexion during valgus loading and rate of loading. Additionally, the inclusion of only male specimens and right arms and the relatively young age of specimen donors in our study likely contributed to the greater failure torque experienced compared with previous work.
Because UCL failure torque and stiffness were not correlated with body weight and height, we recommend that biomechanical analyses of adult baseball pitchers should report absolute magnitudes of elbow varus torque instead of values normalized by body weight and height. Several recent publications have focused on absolute magnitude of elbow varus torque. For example, Escamilla et al 14 compared the biomechanics of professional pitchers with high, moderate, and low contralateral trunk tilt at the instant of ball release and found no difference in absolute magnitude of elbow varus torque among the 3 groups. Solomito et al 33 divided the biomechanics of 99 collegiate pitchers into quartiles based on their stride length. There was lower, but not significantly different, elbow varus torque in the 2 middle groups (70.3 ± 15.9 N·m and 73.4 ± 15.5 N·m) compared with the shortest stride group (78.3 ± 11.8 N·m) and longest stride group (79.5 ± 15.8 N·m). Dowling et al 11 compared high-velocity and low-velocity professional pitchers and reported greater elbow varus torque in the high-velocity group (91 ± 15 N·m) than the low-velocity group (84 ± 15 N·m). Studies such as these, in which elbow varus torque values are reported in newton-meters (instead of unitless normalized values), provide better insight into biomechanics that may lead to UCL stress and risk of failure.
The absence of a correlation between UCL strength and body size suggests that the sports medicine physician can maintain a consistent approach to treatment of adult baseball pitchers, with no special adjustments to clinical evaluation and/or surgical treatment being made based on their physical stature. In the context of the preoperative clinical examination by the surgeon, our findings could help guide the discussion with the patient regarding expected surgical techniques and treatments. Our data imply that factors beyond mere size, such as pitching mechanics, training regimen, and individual physiological differences, may play more significant roles in determining UCL strength and injury risk. Therefore, the physician’s focus should be on treating patients based solely on clinical indications, while assessing the multifaceted elements comprehensively to tailor treatment plans effectively for all pitchers, regardless of their body size, ensuring that optimal care and rehabilitation strategies are used to promote long-term health and performance.
In the realm of physical therapy, Reinold and colleagues 27 recently published a new interval throwing program based on biomechanical data as well as clinical experience with today’s baseball pitchers. This updated program replaces their longstanding interval throwing program published years ago. In developing the new program, the authors considered the workload of flat ground throws and partial effort pitches prescribed, based on the absolute elbow varus torque (N·m) of each throw, not normalized torque. The fact that the current study found no relationship between UCL strength and body size supports that development decision and suggests that the new interval throwing program can be utilized by adult baseball pitchers of all heights and weights.
Limitations
Given that roughly 1 out of every 10 individuals is left-handed, 26 it would be reasonable to assume that approximately 2 of the 20 right arms tested were nondominant arms. In the absence of handedness information pertaining to the cadaveric donors, we elected to choose solely right arms for our study to maximize the percentage of dominant arms. Additionally, donor heights (to the nearest inch) and weights were obtained from the specimen vendor and were not directly measured. These height measurements likely did not have a dramatic effect on our correlations, but they did cause the height data to be somewhat stratified. It is possible that weights were influenced by lifestyle (eg, activity level and overall health) to varying degrees among our sample population, which could cause variability in the BMI. Only 3 of the 20 specimens used in this study could be characterized as likely having a prolonged illness leading to their death (eg, diabetes, liver failure, and enlarged heart). All 3 of these specimens failed via UCL tear near the humerus, which was the most common failure mode in our study. Furthermore, within these 3 specimens, the mean failure torque and stiffness were 52.2 ± 10.3 N·m and 3.40 ± 0.43 N·m/deg, respectively, which were in line with the overall means for the study (45.0 ± 10.5 N·m and 2.72 ± 0.48 N·m/deg, respectively). Finally, it should also be noted that this study tested the relationships between body size and UCL mechanical properties in adult male specimens. Further research is warranted to investigate the relationships in female, youth, and adolescent populations.
Conclusion
Based on our study, valgus failure torque in the elbow does not correlate with patient height or weight. This would suggest that elbow torque from biomechanical analysis of baseball pitchers and other athletes should not be normalized by size but rather be reported as absolute kinetic measurements. The results from this study have the potential to improve the clinical value of studies that investigate pitching biomechanics and their effect on elbow loading as well as also providing valuable insight for surgical and rehabilitative decisions in the treatment of elbow injuries.
Footnotes
Acknowledgements
The authors express their gratitude to Charlie Kutz, Thomas McCutcheon, Matthew Poczatek, and Grant Uldrich for their assistance in study preparation and data collection, as well as Major League Baseball for providing funding for the acquisition of cadaveric arms.
Final revision submitted July 31, 2024; accepted September 10, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was sponsored by Major League Baseball in the form of direct funding for the purchase of cadaveric elbows used in completion of the study aims. R.E.C. received nonconsulting fees from Smith & Nephew. B.K.K. received hospitality payments from Alon Medical Technology and Zimmer Biomet Holdings; education payments from Arthrex, Stryker, Prime Surgicals, and Smith+Nephew; and a grant from Arthrex. M.A.R. received nonconsulting fees from Arthrex; consulting fees from Zimmer Biomet Holdings; and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.