
Abstract
Background:
Medial tibial stress syndrome (MTSS) can impair training and daily activities, underscoring the need for effective treatment. However, there’s limited evidence on using lower-leg exercises for MTSS in recreational runners.
Purpose/Hypothesis:
The purpose of the present study was to determine whether adding lower-leg exercises to a multimodal therapeutic intervention improves the recovery from MTSS in recreational runners. It was hypothesized that adding lower-leg exercises to a multimodal therapeutic intervention would enhance its effect on foot posture and make MTSS recovery more effective than multimodal therapeutic interventions alone.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 40 recreational runners diagnosed with MTSS using history and physical examination (40% women; mean ± SD age, 23.9 ± 3.9 years) were then randomly divided into intervention (n = 20) and control (n = 20) groups. Both groups underwent a multimodal therapeutic intervention involving ice massage, foot orthoses, and extracorporeal shockwave therapy. The intervention group additionally received a tailored lower-leg exercise protocol involving stretching, strengthening, sensorimotor exercises, and foam roller myofascial release. Pain intensity, MTSS severity, perceived treatment effect, quality of life (QoL), and static and dynamic foot posture were assessed at baseline, 6-week, and 12-week follow-up evaluations.
Results:
A mixed model analysis of variance found no significant differences in pain intensity (P = .17) or MTSS severity (P = .30) between the intervention group and the control group. However, there were significant improvements in QoL (P = .003), static foot posture index (FPI) (P = .02), and dynamic arch index (DAI) (P < .001), for the intervention group. After 6 and 12 weeks, the intervention group displayed lower DAI scores than controls (P = .04 and P = .02, respectively). By week 12, the intervention group exhibited significantly higher QoL scores (P = .02) and lower FPI scores (P = .04) compared with controls.
Conclusion:
The study demonstrated that lower-leg exercises within a multimodal treatment positively affected foot posture and QoL, although they did not significantly alleviate pain or affect MTSS severity in recreational runners. Therefore, health care providers are encouraged to integrate these exercises into rehabilitation programs to improve foot posture and QoL for individuals with MTSS. However, future research should focus on larger sample sizes, objective measures, resting control groups, and longer follow-up periods to enhance the understanding of the effects of lower-leg exercises on MTSS management.
Registration:
IRCT 20170114031942N5 (Iranian Registry of Clinical Trials).
Keywords
Medial tibial stress syndrome (MTSS) is a prevalent and debilitating overuse condition associated with jogging, running, and jumping activities. 24 MTSS refers to exercise-induced pain along the posteromedial border of the distal two-thirds of the tibia that occurs during activity and is provoked by palpation of the affected area, but it excludes pain from ischemic origin or signs of the stress fracture. 43 It accounts for up to 35% of all cases of exercise-induced leg pains 24 and involves approximately 10.7% of male and 16.8% of female recreational runners. 6 Clearly, MTSS is problematic, as it can interrupt an individual’s active lifestyle and sports performance and potentially end sporting careers.1,44 The long recovery time ranges from 4 to 18 months,23,31 and there is a high recurrence rate, with individuals who have a history of MTSS experiencing a recurrence rate between 20.1 and 32.2 times greater than those without a history of the condition,13,36 adding to the costs and inconvenience of MTSS. Therefore, there is an urgent need to reduce MTSS recurrence rates and prevent the development of MTSS in physically active individuals.
The treatment of MTSS includes various interventions such as avoiding the triggering activity, cross-training, cryotherapy, shockwave therapy, massage, and a pneumatic leg brace.28,29,44 However, some systematic reviews have shown that these interventions are not effective in treating MTSS,28,29,44 and most only address pain rather than the main causes of the condition. It is suggested that interventions targeting modifiable risk factors, such as normalizing lower-limb biomechanics, arch taping, foot orthoses, and ankle strengthening and stretching exercises, are more likely to be effective in treating MTSS.1,15
Numerous risk factors have been proposed for MTSS, among which excessive foot pronation and reduced lower-leg girth are the most well-known and at the same time modifiable.3,4,45 Both excessive foot pronation and reduced lower-leg girth can lead to MTSS symptoms by increasing tibiofascial traction and ground-reaction force on the tibia during running.4,36,45,46 This is caused by the decreased damping capacity of the lower leg, impaired lower-leg muscle strength and endurance, and greater and longer eccentric activity of the antipronatory muscles.4,36,45,46 Reduced plantarflexor muscle endurance capacity,18-20 invertor and evertor strength imbalance,20,47 smaller flexor hallucis longus cross-sectional area, 19 and deficits in maximal plantarflexor isometric strength 19 are other muscular risk factors associated with MTSS development. Burne et al 4 found a causal relationship between reduced lean lower-leg girth and MTSS development in athletes, suggesting that the amount of lower-leg muscle bulk could affect the ability of the lower leg to attenuate ground-reaction forces, potentially leading to MTSS. In addition, Clement 7 believes that calf muscle weakness and fatigue can predispose athletes to MTSS by transferring excessive force to the tibia. Wakeling et al 40 have reported that lower-leg muscle activity is responsive to ground-reaction forces, and this damping effect may play a role in injury prevention. Therefore, addressing well-known and modifiable risk factors such as foot pronation and lower-leg muscle dysfunction during treatment can be an effective therapeutic option to reduce the recurrence rates of MTSS and treat and/or prevent the condition.
Lower-leg exercises are often recommended for the treatment of MTSS,21,41 and they are a key component of almost all interventions provided by studies for people with MTSS.15,32 While it has not been scientifically proven yet, some studies suggest that lower-leg exercises may be effective in managing the pain and symptoms of individuals with MTSS.21,23 Although lower-leg exercises have been shown to be effective in managing some overuse injuries related to excessively pronated feet14,16 and resulted in a 2.42-fold lower rate of running injury compared with the control group in recreational runners, 38 no study has investigated the use of these exercises for runners with MTSS. Furthermore, a controlled trial found that adding arch support foot orthoses to a therapeutic intervention leads to an earlier diminishment of pain and MTSS severity and better perceived therapeutic effects. 30 However, this begs the question that if arch support foot orthoses can have such an effect by supporting the longitudinal foot arch, should it not be possible to address this directly through training of the ankle and foot muscles? Therefore, the purpose of the present study was to determine whether adding lower-leg exercises to a multimodal therapeutic intervention improves the recovery from MTSS in recreational runners. We hypothesized that adding lower-leg exercises to a multimodal therapeutic intervention would enhance its effect on foot posture and make MTSS recovery more effective than multimodal therapeutic interventions alone.
Methods
Study Design
This was a 12-week, parallel-group randomized controlled trial with repeated measures at baseline, 6-week, and 12-week follow-up (Figure 1).
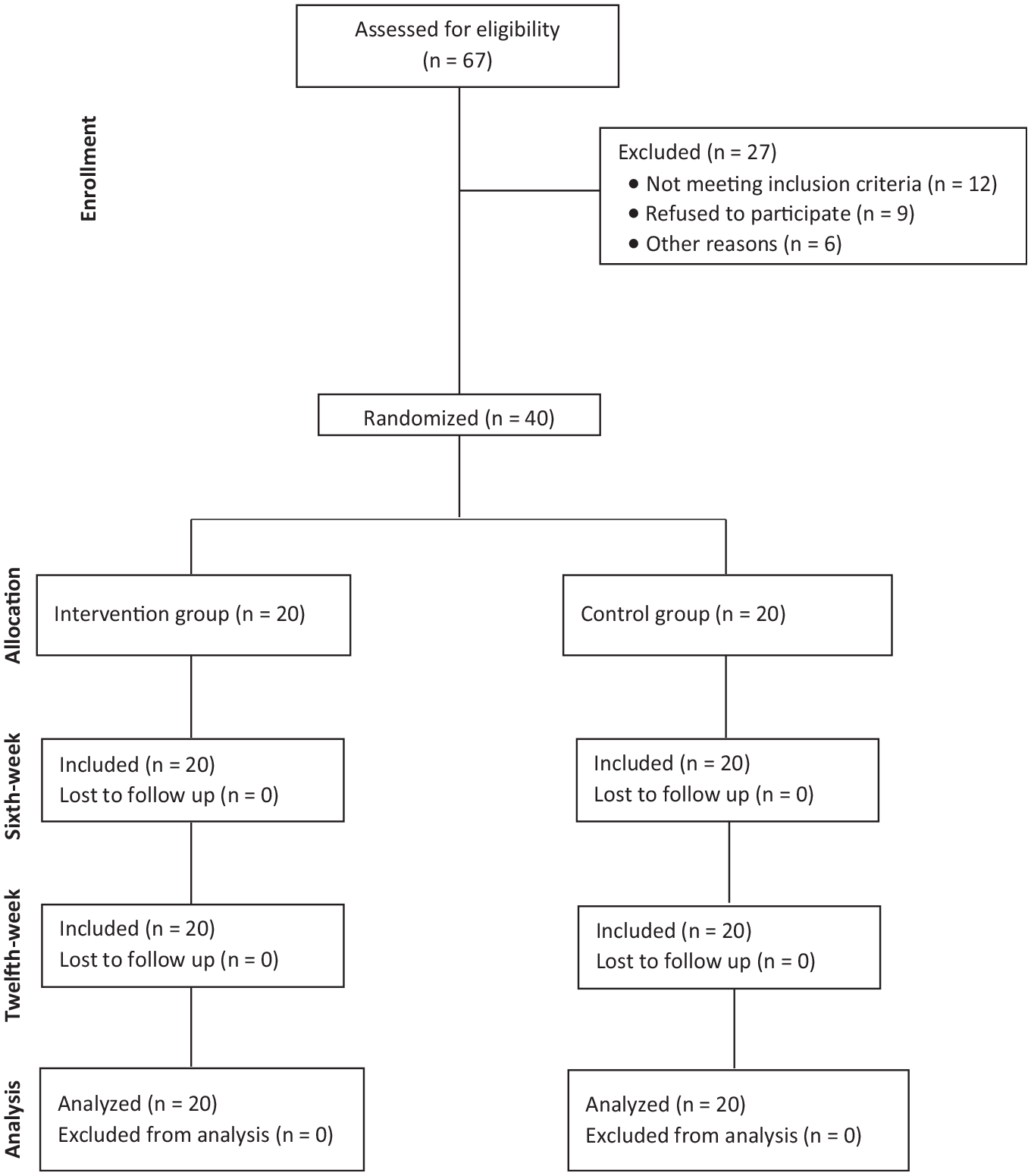
CONSORT (Consolidated Standards of Reporting Trials) flow diagram of participants’ enrollment, randomization, follow-up, and analysis.
Participants
Participants were recruited between June 2018 and August 2018 through presentations in local community, public, and university clubs in Isfahan, Iran. A group of 67 recreational runners with potential symptoms of MTSS were screened by a health care practitioner, and 40 individuals who met the inclusion criteria were included in the study. MTSS can be diagnosed accurately through patient history and physical examination. 42 The inclusion criteria for the study required participants to have experienced exercise-induced pain that persisted for hours or days afterward, the pain located in the distal half of the posteromedial tibia over an area >5 cm in length (as pain <5 cm is typically associated with stress fractures). 46 Symptoms must have been present for ≥3 weeks, with discomfort specifically elicited upon palpation of the tibial posteromedial border, confirmed by a health care practitioner.10,13,46 Confirmation of the diagnosis by a health care practitioner was also necessary. Additionally, participants had to be between 18 and 45 years old, regularly engage in recreational running for ≥45 minutes or >10 km per week over the past 3 months, and be capable of providing informed written consent.
Participants were not included in the study if they had a prior diagnosis of paresthesia, experienced other causes of exercise-induced leg pain (eg, tibial stress fracture and chronic compartment syndrome), were unhealthily obese (body mass index >35 kg/m2), had received physical therapy treatment in the previous 6 months, had a history of lower-limb traumatic injury or had undergone surgery within the past 6 months, or had a leg-length discrepancy of ≥2.5 cm. 12
Ethical Approval
Participants were informed of the study procedures and provided written informed consent. All procedures were approved by the institution review board of Shahroud University of Medical Sciences, and the trial protocol was prospectively registered in the Iranian Registry of Clinical Trials.
Randomization
Participants were enrolled by an independent health care practitioner, and concealed allocation was conducted using a computer-generated sequence (Version 2.0; Random Allocation Software), created by an independent assessor who was not directly involved in the trial and did not participate in the analysis or interpretation of the results. A block randomization design (block sizes of 2, 4) was applied to ensure an equal number of male and female participants in each group. Patients were randomly assigned to either the intervention group or the control group using simple randomization with a 1:1 allocation ratio. Outcomes were assessed by a trained sports scientist (AH) who was blinded to the treatment allocation group. The group allocations were concealed from the investigators enrolling participants, laboratory specialists assessing the variables, and data analysts in sequentially numbered, opaque, sealed envelopes. The corresponding envelopes were opened after enrolled participants had completed all baseline assessments.
Outcome Measures
All assessments were carried out by a trained sports scientist who was blinded to group allocation (A.H.) and were performed 4 days before the first intervention session (baseline measurements), 6 weeks after intervention (follow-up 1), and 12 weeks after intervention (follow-up 2) for each group. All clinical assessments were conducted at a university-based laboratory.
Participants’ body mass was measured to the nearest 0.1 kg using a digital scale (SECA 760; Vogel & Halke GmbH & Co), and height was recorded with an accuracy of 0.1 cm. The body mass index was calculated by dividing body mass by the square of height (kg/m2). Data on the affected side, duration of symptoms in days, and weekly running distance in kilometers were also documented.
Pain severity was assessed using a linear visual analog scale, with pressure of 3 kg applied using an algometer (Baseline model 12-0304; Fabrication Enterprise Inc.) over the most tender area of the tibial border. The tenderest area of the leg (portion of 5-cm length ) was highlighted with a marker on each affected leg. 30
Perceived treatment effect was measured using the global rating of change on a 7-point Likert scale. 37 Patients were requested to assess their self-perceived “overall change” compared with their status at the initial visit. Response options were presented on a continuum, ranging from −3 (labeled "totally worse") on the left to +3 (labeled "totally better") on the right, with zero in the middle (labeled "no change"). A positive point to the right indicates improvement, while a negative point to the left indicates deterioration of the condition.
Quality of life (QoL) was measured using the paper format of the 36-item Short Form Health Survey (SF-36). 25 SF-36 consists of 36 items that are grouped into 8 domains and summarized in 2 summary subscales: the Physical Component Summary (PCS), composed of the physical functioning, role limitations due to physical health problems, bodily pain, and general health domains; and the Mental Component Summary (MCS), composed of the vitality, social functioning, role limitations due to mental health problems, and mental health domains. The SF-36 is scored from 0 to 100, with a higher score representing a better or more favorable QoL.
Dynamic foot posture was assessed using the dynamic arch index (DAI), measured with a pressure plate (50 × 60 cm, PT 3D Scan; Payafnavaran Ferdowsi Co) located at the center of a 12-m runway during self-selected walking speed trials. The DAI is calculated as the ratio of the midfoot contact area relative to the whole footprint area excluding the toes. 8 A high ratio indicates higher foot pronation, with a ratio of <0.21 indicating a high arch, 0.21-0.28 indicating a normal arch, and >0.28 indicating a low arch. 5
Static foot posture was assessed using the foot posture index (FPI)–6, which includes 6 specific criteria: palpation of the talar head, curvature above and below the lateral malleoli, calcaneal alignment in the frontal plane, prominence around the talonavicular joint, congruence of the medial longitudinal arch, and the degree of forefoot abduction or adduction relative to the rearfoot. Each criterion is rated on a scale from −2 to +2, and the total score defines the target foot posture as normal (0 to +5 score), pronated foot (+6 to +9 score), highly pronated foot (≥+10 score), supinated foot (−1 to −4 score), or highly supinated foot (−5 to −12). 35
Adverse events and adherence to the exercise program were recorded using a questionnaire completed by participants 4 times every 3 weeks. Adverse events were defined as short- to long-term consequences manifested in serious, distressing, uncomfortable, and unacceptable symptoms for the participants with a known or plausible association with treatment and those for which there is none. 33
Interventions
Extracorporeal shockwave therapy consisted of 5 sessions, beginning with 1500 pulses at an energy flux density of 0.1 mJ/mm2 and incrementally increasing to 0.3 mJ/mm2 by the final session. Participants were instructed to avoid intense exercise training for 48 hours following each shockwave therapy session. Additionally, they adhered to a graduated walk-to-run protocol designed to restore their functional level in accordance with operational requirements.
Multimodal Therapeutic Intervention
All participants, in both the control and the intervention groups, received a multimodal therapeutic intervention. This involved applying ice directly to the affected area for approximately 15 to 20 minutes after each running session. 11 Extracorporeal shockwave therapy was administered in 5 sessions, beginning with 1500 pulses at an energy flux density of 0.1 mJ/mm2 and incrementally escalating to 0.3 mJ/mm2 by the final session.22,30 Participants were instructed to avoid intense exercise training for 48 hours following each shockwave therapy session. Additionally, they adhered to a graduated walk-to-run protocol designed to restore their functional level in accordance with operational requirements.22,23 This protocol was based on the Wolff Law, emphasizing the need for appropriate stress to remodel bone and soft tissue, promoting optimal strength and tissue integrity. 17 Preexisting foot orthoses were permitted, but participants were not allowed to modify them during the study period. At the beginning of the study, 25% of the participants in the intervention group and 30% of those in the control group were using foot orthoses, and they continued to use them throughout the study. Analgesic use was also recorded during baseline testing and at all follow-up visits. Participants were instructed to avoid cointerventions during the study period, starting 72 hours before participation in the study.
Participants in the intervention group received both the multimodal therapeutic intervention and the prescribed leg exercises concurrently right from the beginning of the treatment period.
Lower-Leg Exercise Intervention
Recreational runners in the intervention group received a lower-leg exercise intervention aimed to improve ankle flexibility, strength, and proprioception. The exercise program included 2 calf muscle stretching exercises (gastrocnemius and soleus), 3 strengthening exercises for the plantarflexors and invertor muscles, 1 sensorimotor exercise (the short-foot exercise) to enhance proprioception and intrinsic foot muscles, and 1 foam roller myofascial release technique to reduce calf muscle stiffness and improve ankle joint range of motion. Resistance exercises were performed using the participant’s body weight and TheraBand tubing. intensity of the strengthening exercises progressed throughout the study by increasing the load from yellow to red, green, blue, and finally black bands, as well as from 40% to 85% of one-repetition maximum (1RM) in free weights. The progression also included an increase in the number of sets (from 3 to 4) and repetitions (from 12 to 15) for isotonic strengthening exercises. For stretching exercises, the hold time increased from 20 to 30 seconds, and the repetitions rose from 5 to 7, provided the participants demonstrated good-quality movement. Once participants could complete 4 sets of 15 repetitions for 1 week without increasing symptoms, they advanced to the next color-coded levels of resistance with TheraBand (starting with yellow bands and moving sequentially to red, green, blue, and finally black bands, and from 40% to 85% 1RM of free weight). The intensity of the exercise program was prescribed on an individual basis and progressed from moderate (a score of 12-14) to high (a score of 14-16) using the rate of perceived exertion of the Borg scale 27 (Table 1).
Lower-Leg Exercise Intervention Framework

The control group did not receive lower-leg exercises to uphold the integrity of the randomized controlled trial design, ensuring a clear baseline for assessing the specific effects of the exercise intervention and minimizing confounding variables. However, since all study participants experienced some degree of pain and disability, including a multimodal therapeutic intervention in both groups addressed ethical concerns regarding nontreatment and promoted robust results. Additionally, after completing the study, participants in the control group were given the opportunity to become familiar with the leg exercise intervention.
The interventions comprised clinic-based programs supervised by an experienced physical therapy and sports science specialist (M.F.M.), with input from a sports physician.
Statistical Analysis
Using the software package G*Power 3.1, we conducted a priori sample size calculations based on effect sizes of MTSS intensity from a previous study. 30 With an effect size of Cohen f = 0.25 (medium effect size), a 2-tailed significance level (α) of .05, and desired power (1-β) of 0.85, a sample size of 16 in each group was required. To account for an anticipated dropout rate of 20%, we enrolled 20 participants in each group.
SPSS statistical software (Version 18.0; SPSS Inc) was used for all statistical analyses. The normality of the data was assessed using the Shapiro-Wilk test. A 2 (groups: control/intervention) ×3 (times: baseline/6 weeks/12 weeks) mixed model analysis of variance was used to test the main and interaction effects of lower-leg exercise on the outcome measures (ie, pain intensity, MTSS severity, QoL, dynamic foot posture, and static foot posture). Additional follow-up comparisons were conducted using Bonferroni-corrected t tests for multiple comparisons. The values are presented as mean ± SD as well as the corresponding 95% CIs, and the statistical significance level was set at P < .05. To better understand the range of training gains, Cohen d_z was calculated, expressing the effect size of the comparisons. Values between 0.01 and 0.2, 0.21 and 0.50, 0.51 and 0.80, and over 0.81 represent trivial, small, medium, and large effects, respectively.
Results
Baseline characteristics are outlined in Table 2. No side effects were reported for the interventions.
Participants’ Demographics and Clinical Characteristics a
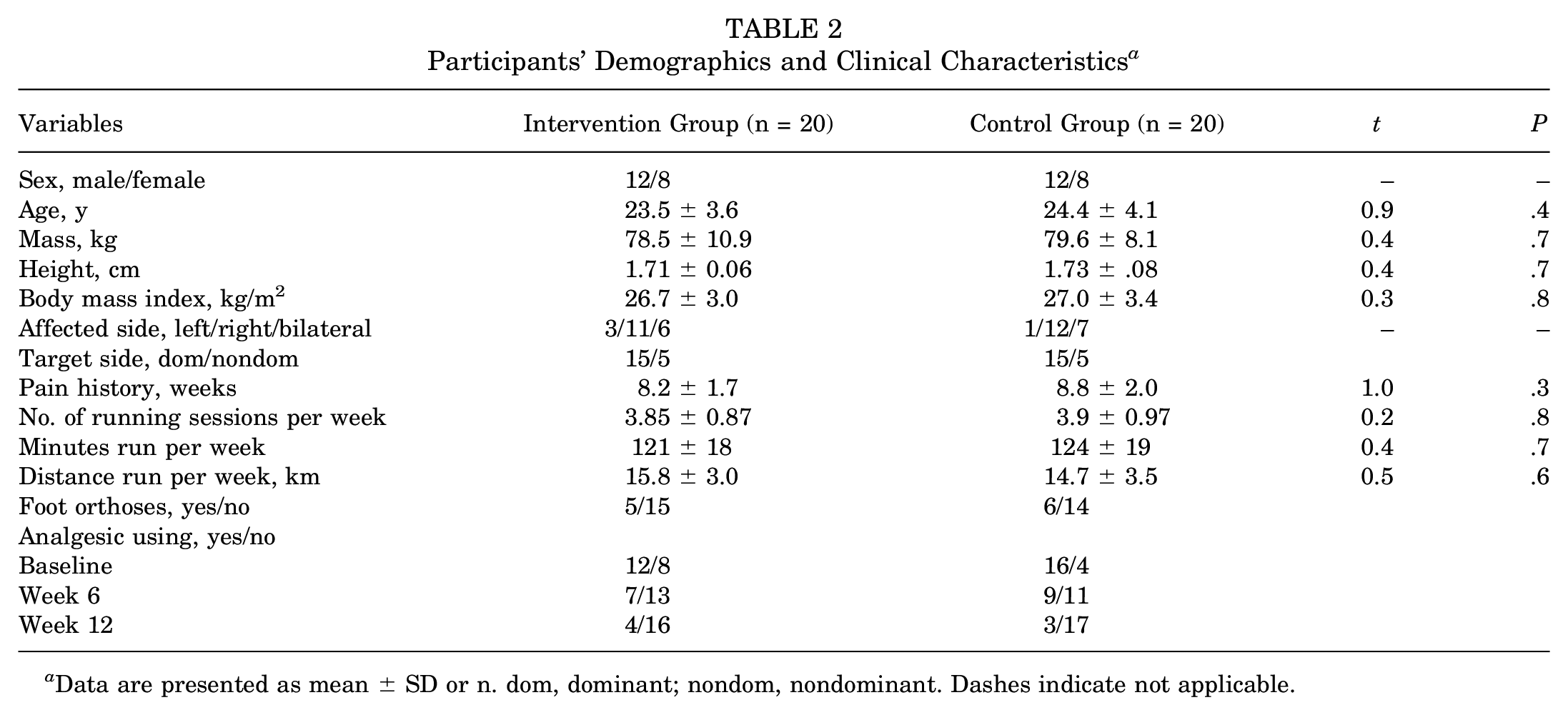
Data are presented as mean ± SD or n. dom, dominant; nondom, nondominant. Dashes indicate not applicable.
There were no significant differences between groups in terms of pain intensity (F(1, 38) = 1.8; P = .17) and MTSS severity (F(1, 38) = 1.23; P = .30), indicating no significant difference between the intervention and the control groups (Table 3). However, a significant difference was found for QoL (F(1, 38) = 6.25; P = .003), FPI (F(1, 38) = 4.11; P = .02), and DAI (F(1, 38) = 8.53; P < .001), indicating a significant difference between the intervention and control groups (Table 3). Follow-up comparison revealed that participants in the exercise group exhibited lower scores in DAI compared with the control group after 6 weeks of intervention (t(38) = 2.2; P = .04; Cohen d = 0.69 ) and 12 weeks of intervention (t(38) = 2.5; P = .02; Cohen d = 0.79) (Figure 2, A and B). In addition, a follow-up comparison showed that the QoL (t(38) = 2.6; P = .02; Cohen d = 0.43) and FPI (t(38) = 2.0; P = .04; Cohen d = 0.41) were significantly higher and lower for the intervention group than the control group at week 12, respectively (Figure 2, A and B). Regarding the physical and mental components of the QoL, there was a significant interaction for PCS scores (F(1, 38) = 9.1; P = .001) but not for MCS scores (F(1, 38) = 2.5; P = .07) (Table 3). Our data indicate that the perceived treatment effects improved over time for both the intervention and the control groups, with the intervention group showing more pronounced positive outcomes. By week 12, 55% of the intervention group reported feeling "totally better," compared with 40% in the control group. Additionally, at both week 6 and week 12, a higher percentage of participants in the intervention group reported "much better" or "totally better" improvements. However, chi-square analysis revealed no significant differences between the groups at the 6th and 12th weeks, with results showing χ2 = 1.61 (P = .66) and χ2 = 1.1 (P = .60), respectively (Figure 3).
Descriptions of the Outcomes and Results of Mixed-Model ANOVA a

ANOVA, analysis of variance; MTSS, medial tibial stress syndrome. Bold values refer to values that are significant at P < .05.
Significant between-group difference at P < .05.

Standardized effect size related to between-group comparisons for each dependent variable (A) at week 6 and (B) at week 12. DAI, dynamic arch index; FPI, foot posture index; MTSS, medial tibial stress syndrome; PI, pain intensity; QoL, quality of life.
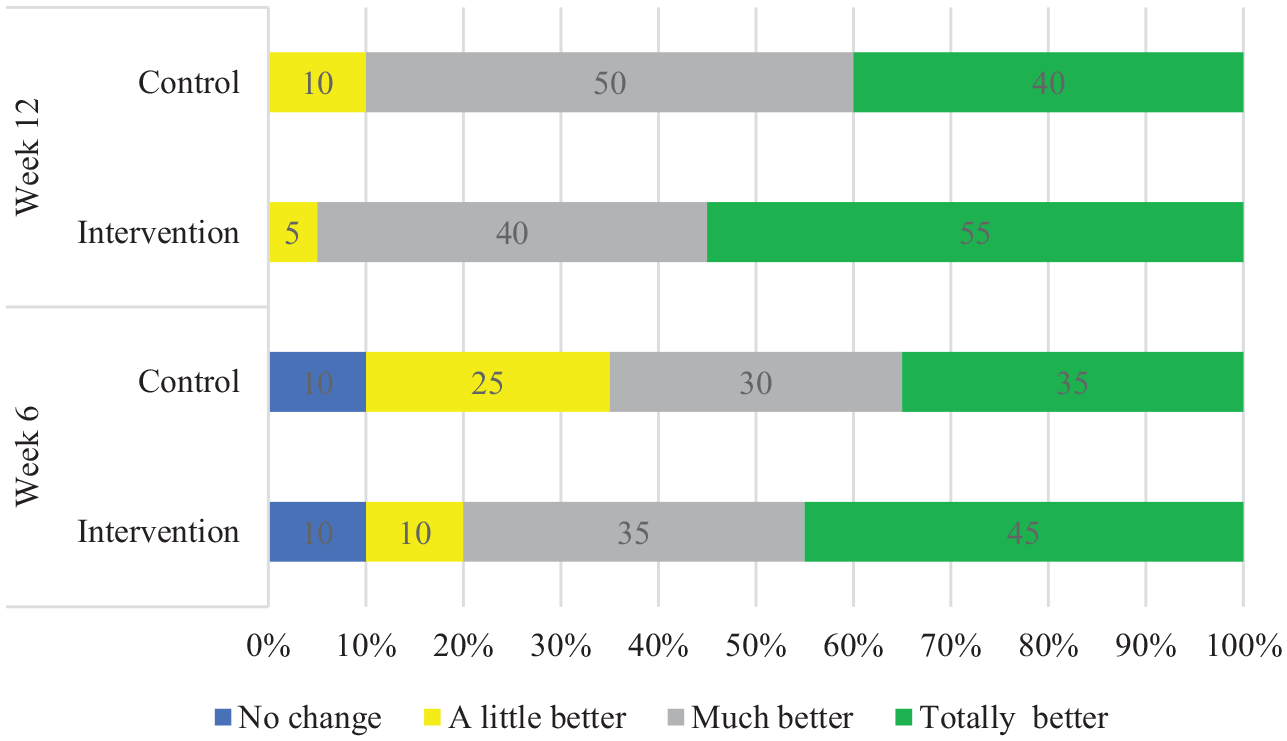
Perceived treatment effect by participants of each group at the 6th and 12th weeks.
Discussion
The present study found no significant differences in pain levels, MTSS severity, or perceived therapeutic effects between the intervention and control groups among recreational runners with MTSS. However, the intervention group demonstrated significant improvements in the FPI, DAI, and QoL (PCS) compared with the control group. Specifically, the intervention group had lower DAI scores at 6 weeks (Cohen d = 0.69) and 12 weeks (Cohen d = 0.79). Additionally, at week 12, they exhibited higher QoL scores (Cohen d = 0.43) and lower FPI scores (Cohen d = 0.41), indicating meaningful benefits from the lower-leg exercises.
One of the findings from the present study was that incorporating lower-leg exercises in the multimodal therapeutic intervention resulted in an additional effect ranging from 10.5% to 12.8% on dynamic foot posture and 12% to 35% on static foot posture when comparing the intervention group with the control group during the follow-up period at the end of weeks 6 and 12. In line with our study, Mulligan and Cook 26 showed that engaging in foot muscle exercises for 8 weeks can decrease navicular drop by 2.2 mm and result in reduced excessive foot pronation by 29% in students with excessive foot pronation. Similarly, Andreasen et al 2 reported a reduction of 2 mm in navicular drops for patients with excessive pronation and chronic pain conditions. Electromyographic studies have demonstrated the critical role of both intrinsic and extrinsic foot muscles in maintaining the medial longitudinal arch and foot posture.26,32,38 Muscle fatigue and weakness in these muscles have been identified as the causes of excessive foot pronation during running.18,20 Therefore, engaging in lower-leg exercises can potentially enhance muscle endurance and strengthen the lower-leg muscles, leading to improvements in both dynamic and static foot posture. Considering that these exercises have the ability to affect static and dynamic foot posture in recreational runners with MTSS, serving as potential indicators of their effectiveness in preventing MTSS recurrence. The notion of MTSS potentially evolving into a tibial stress fracture suggests a continuum between the 2 conditions, 45 highlighting the need for further research to explore the long-term effectiveness of integrating lower-leg exercises in preventing MTSS recurrence and its progression to a full tibial stress fracture.
The present study revealed another significant finding regarding the effectiveness of lower-leg exercises when combined with other therapeutic interventions for individuals with MTSS. These additional exercises have been shown to enhance the overall QoL for these individuals, likely through their effects on the PCS rather than the MCS of the QoL. This observation suggests that the effects of therapeutic exercises on the QoL of individuals with musculoskeletal pain extend beyond just pain levels. Therefore, exercise therapy for individuals with MTSS may not directly reduce pain, but its multifaceted benefits, including enhancing lower-limb function, increasing muscle strength, improving psychological well-being, enhancing mobility, and preventing further exacerbation collectively contribute to an improved overall QoL.
An interesting finding from our study was that the addition of foot exercise to a multimodal therapeutic intervention did not have an additional effect on the management of pain level and MTSS-related symptoms, as confirmed by the perceived treatment effect. This result is consistent with a study by Andreasen et al, 2 who suggested that adding lower-leg exercises to other interventions resulted in a 2-mm decrease in navicular drop in patients with excessive pronation and chronic pain conditions, but did not have an incremental effect on reducing pain and symptoms in these patients. Moen et al 23 also compared 3 MTSS treatment methods (graded running protocol, graded running protocol with ankle exercises, and graded running protocol combined with a compression garment) and did not observe a significant difference in terms of the effect on the physical function and overall satisfaction with the treatment. Two theories have been proposed regarding the pathophysiology of MTSS: the tibial fascial–traction theory 9 and the tibial stress reaction theory. 19 According to the tibial fascia–traction theory, the eccentric contraction of the plantarflexor and invertor muscles of the lower leg, particularly the soleus, tibialis posterior, and flexor digitorum longus, during the stance phase of running, applies a strong traction force to the junction of these muscles. This force eventually leads to periostitis or fasciitis. 9 Proponents of the tibial stress reaction theory believe that MTSS, similar to a tibial stress fracture, is a bone stress reaction resulting from repetitive loading and subsequent deformation of the tibial structure. 43 We hypothesized that by incorporating lower-leg exercises into a multimodal therapeutic intervention, we can enhance the damping capacity of the lower leg, strengthen the lower-leg muscles, increase endurance, and reduce compensatory contractions of the antipronatory muscles during the stance phase of running. This, in turn, would lead to a reduction in tibiofascial traction and the ground-reaction force applied to the tibia, potentially resulting in a faster or improved recovery from MTSS. However, the results did not align with our expectations, as the incorporation of lower-leg exercises into a multimodal therapeutic intervention had no incremental effect on pain levels and MTSS symptoms.
The intervention group participants experienced a decrease in tibial pain intensity of 2.4 cm at the end of the 6th week, which was higher compared with the control group that had a decrease of 1.8 cm in tibial pain intensity. Moreover, the decrease observed in the intervention group exceeded the minimal clinically important difference threshold of 2.2 cm for pain visual analog scale in orthopaedic studies. 34 However, the reduction in MTSS score was nearly the same in the control group (1.6) and the intervention group (1.7) in the 6th week. It is worth noting that any change exceeding 0.69 in the MTSS score is considered the smallest significant detectable change for patients with MTSS. 44 Additionally, based on the 7-point scale used, the mean perceived treatment effect by participants in the intervention group at the end of the 6th and 12th weeks was rated as "much better." However, for the control group, it was rated as "better" and "much better" at the respective time points. The trend of reducing analgesic use was almost the same for both groups, which is consistent with the observed trend in the variables of MTSS-related pain and symptoms. This suggests that the treatments effectively reduced analgesic dependence.
Strengths and Limitations
This study is the first to investigate the effects of lower-leg exercises on runners with MTSS, focusing on pain level, MTSS severity, QoL, foot posture, and perceived therapeutic effects. However, there are several limitations to consider. The small sample size, focused on recreational runners, may limit the generalizability of findings to other athlete populations. The study’s reliance on self-reported measures, such as pain and QoL, introduces potential biases that could be mitigated in future trials by incorporating objective methods such as bone scanning and kinematic analysis. While MTSS can be reliably diagnosed through patient history and physical examination, 42 using imaging techniques could help rule out tibial stress fractures, particularly in cases of extensive pain. Although participants’ running volumes and terrains were not strictly controlled, both the intervention and the control groups reported similar running times, distances, and terrains at baseline, potentially minimizing injury-related differences. Participant blinding was not feasible due to the study’s nature and protocols, but implementing it would have ensured equal treatment and unbiased outcome assessment. Ethical concerns prevented the inclusion of a control group that solely rested, limiting the ability to draw definitive conclusions about the intervention’s effectiveness compared with rest. Moreover, the study did not analyze the participants’ energy availability, which may directly influence MTSS progression, 6 or the type of footwear worn, which could affect biomechanics and injury risk. 39 The 12-week follow-up period may not adequately capture long-term outcomes, given that recovery from MTSS can extend up to 18 months. Future research should consider these factors to provide a more comprehensive understanding of their effects on MTSS management.
Conclusion
The high recurrence rate of MTSS, along with its enduring impact on physical and sometimes daily activities, underlines the need to explore the sustained effectiveness of incorporating to mitigate these consequences. The primary findings suggest that incorporating lower-leg exercises into a multimodal therapeutic intervention improved foot posture and QoL (physical aspects) but didn’t offer additional benefits in pain relief, MTSS severity, or perceived therapeutic effects in recreational runners with MTSS. Therefore, health care providers are encouraged to integrate these exercises into rehabilitation programs to improve foot posture and QoL for individuals with MTSS. However, future research should focus on larger sample sizes, objective measures, resting control groups, and longer follow-up periods to enhance the understanding of the effects of lower-leg exercises on MTSS management.
Footnotes
Final revision submitted August 6, 2024; accepted August 30, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Shahroud University of Medical Sciences (IR.SHMU.REC.1396.168).