
Abstract
Background:
Acetabular subchondral cysts are commonly identified signs of joint degeneration and arthritis. This pathology is generally considered a relative contraindication for hip preservation surgery.
Purpose:
To investigate the effect of arthroscopic bone grafting for the treatment of acetabular subchondral cysts.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
We completed a retrospective analysis of hip arthroscopies performed by the senior author between 2013 and 2021. Patients with radiologic evidence of acetabular cysts who underwent arthroscopic bone grafting, with or without subsequent periacetabular osteotomy (PAO) and/or derotational femoral osteotomy with a minimum of 2-year follow-up, were included in the analysis. Patients undergoing surgical treatment for diagnoses of slipped capital femoral epiphysis, Legg-Calves-Perthe disease, osteochondromatosis, or postdislocation syndrome, as well as patients who refused to participate in the study, were excluded. We compared the patient-reported outcomes (PROs) for patients who underwent arthroscopic bone grafting with a case-matched control group without acetabular cysts with the same surgical route (hip arthroscopy or hip arthroscopy followed by PAO). An “inside-out” arthroscopic bone grafting technique was utilized, which allowed for precise access to the cystic cavity through the articular side. We analyzed postoperative PROs at a minimum of 2 years postoperatively using the international Hip Outcome Tool (iHOT-12) and Nonarthritic Hip Score (NAHS).
Results:
In total, there were 44 hips in the experimental group and 78 hips in the control group. The mean PRO interval in the experimental group was 3.4 years (range, 2-5 years postoperatively), with 20 patients reaching PROs 5 years postoperatively. The experimental group reported significant improvement of iHOT-12 and NAHS scores postoperatively (both P < .001). Postoperative iHOT-12 and NAHS scores did not significantly differ between groups over a 5-year follow-up interval (P = .26 and .17, respectively). Radiographic evidence of cyst healing was achieved in all 7 patients who underwent postoperative magnetic resonance imaging, with 3 cases of complete resolution.
Conclusion:
Acetabular subchondral cysts treated with an inside-out method of arthroscopic bone grafting in the setting of hip preservation surgery with or without PAO was associated with a significant improvement in midterm PROs, comparable with a control group of patients without acetabular cysts who did not undergo bone grafting. Our results support the use of arthroscopic grafting in appropriately selected patients and suggest that hip preservation is not contraindicated in patients with acetabular subchondral cysts.
Acetabular subchondral cystic changes are commonly identified early signs of joint degeneration, biomechanical failure, and early arthritis in young adults with mechanical hip pathologies such as femoroacetabular impingement (FAI) or hip dysplasia.10,15 The presence of these cysts in symptomatic patients has been shown to correlate with the presence and severity of pain, as well as the speed of joint deterioration. 2
In more advanced stages of disease, acetabular cysts can be identified on plain radiographs. However, they are often difficult to detect in their early stages; thus, advanced imaging modalities, such as magnetic resonance imaging (MRI), are often employed for enhanced cyst visualization.2,5 Additionally, computed tomography (CT) enables more detailed identification of cyst location and size and can better investigate the location and extent of their communication with the joint space. 7
For many surgeons, subchondral cysts pose a relative contraindication for hip preservation surgery, as the presence of subchondral edema with an acetabular cyst on MRI has been shown to predict lower success rates and inferior patient-reported outcomes. 15 Acetabular subchondral cysts are relatively common in patients with FAI and/or dysplasia.10,15 Further, Hartigan et al 9 reported that patients with subchondral cysts undergoing hip arthroscopy converted to total hip arthroplasty (THA) in 36% of cases. The relative preclusion of this cohort from hip preservation surgery may force patients to choose between enduring chronic hip dysfunction or electing to undergo premature THA. The purpose of this study was to investigate the effect of arthroscopic bone grafting for the treatment of acetabular subchondral cysts. We hypothesized that an “inside-out” technique of arthroscopic bone grafting would be associated with significantly improved midterm outcomes in appropriately selected patients, even in the setting of hip dysplasia.
Methods
After institutional review board approval was obtained, the authors performed a retrospective analysis of prospectively collected data on a cohort of patients undergoing hip preservation surgery (hip arthroscopy with or without periacetabular osteotomy [PAO] and/or derotational femoral osteotomy [DFO]) with the senior author (O.M.D.) between April 2013 and August 2021 who met the following inclusion criteria: (1) persistent hip pain and mechanical symptoms refractory to nonoperative treatment (physical therapy, nonsteroidal anti-inflammatory drugs, activity modifications, corticosteroid or platelet-rich plasma injections) lasting ≥3 months, (2) reproducible clinical examination findings suggestive of intra-articular pathology, (3) joint-space width exceeding 3 mm on all views of plain radiography and cross-sectional imaging, (4) the presence of ≥1 acetabular intraosseous cyst as noted on preoperative MRI and CT, and (5) minimum 2-year follow-up (Figure 1). Patients undergoing surgical treatment for diagnoses of slipped capital femoral epiphysis, Legg-Calves-Perthe disease, osteochondromatosis, or postdislocation syndrome, as well as patients who refused to participate in the study, were excluded.

Flowchart outlining patient selection and study group formation. DFO, derotational femoral osteotomy; PAO, periacetabular osteotomy; SCFE, slipped capital femoral epiphysis.
Applying the same inclusion and exclusion criteria as outlined above, a matched-pair control group of patients undergoing hip preservation surgery without the presence of acetabular cysts was selected based on demographic characteristics (patient sex and age) and similar surgical course (did or did not undergo PAO and/or DFO). This group was used as a reference point for the expected improvement in outcome scores. Demographic variables including age, clinical diagnosis, sex, height, weight, and body mass index were recorded for all patients.
The experimental cohort was then stratified into 2 groups: (1) patients who underwent hip arthroscopy with bone grafting and subsequently underwent PAO surgery and (2) patients who underwent hip arthroscopy with bone grafting without PAO surgery. The international Hip Outcome Tool (iHOT-12) scores at ≥2 years postoperatively were analyzed and compared between the 2 groups. This subanalysis was conducted to investigate the efficacy of inside-out arthroscopic bone grafting specifically in patients with acetabular dysplasia.
All patients who underwent PAO underwent routine hip arthroscopy 3 to 10 days prior to address intra-articular pathology, such as cartilage or labral pathology and FAI that may worsen after increasing femoral head coverage following PAO. Hip arthroscopy was performed prior to PAO (rather than during the same anesthetic) in order to (1) avoid prolonged anesthesia time, (2) avoid fluid from hip arthroscopy in the surgical field during the PAO, (3) enable stationary bicycle use prior to PAO, which reduces the rate of capsulolabral adhesion formation by reducing the development of pooled blood, and (4) allow the surgeon and patient to discuss possibly opting out of the PAO if substantial articular cartilage damage is seen during arthroscopy. 20
Imaging Protocol and Measurements
After a comprehensive history and physical examination, patients underwent a standardized series of preoperative plain radiographs (including weightbearing anteroposterior [AP], cross-table lateral, and AP pelvic views), MRI, and, if indicated for surgical planning, CT scans with 3-dimensional surface-rendered reconstruction of the entire pelvis, proximal femurs, and knees.
Clinical diagnosis of acetabular dysplasia was determined according to accepted pathomorphologic signs and measurements.14,26 In addition to well-established physical examination findings, radiographic evidence of frank or borderline hip dysplasia (lateral center-edge angle [LCEA] of ≤25°, sourcil angle of ≥10°), excessive acetabular version and/or femoral antetorsion, interruption of the Shenton line on the weightbearing AP pelvic radiograph, and MRI findings of labral hypertrophy and tears, articular cartilage thickening and/or inside-out chondral flaps, or a ligamentum teres tear all aided in establishing a diagnosis of symptomatic hip instability.14,25,26
In addition to suggestive physical examination findings, the clinical diagnosis of FAI was determined according to accepted pathomorphologic measurements on radiographic and magnetic resonance imaging.12,24 Confirmative findings of pincer-type FAI included features corresponding to focal acetabular overcoverage (crossover sign or ischial spine sign), an LCEA exceeding 40°, and/or acetabular inclination of <0°. Cam-type FAI was diagnosed based on an alpha angle exceeding 50° on radial sequences of the head-neck junction and a femoral head-neck offset ratio of <0.18. 24 Mixed-type FAI diagnosis was diagnosed by the coexistence of pincer-type and cam-type morphologies. An LCEA between 20° and 25° indicates borderline dysplasia, whereas an LCEA of <20° represents frank dysplasia. 14
Acetabular intraosseous cysts were identified on preoperative noncontrast MRI (Figure 2) and were evaluated for size, consistency, and location. On MRI, acetabular subchondral cysts present as hyperintense foci underlying subchondral bone on fat-suppressed T2-weighted or short tau inversion recovery sequences, with fat-suppressed T1-weighted postcontrast imaging demonstrating peripheral enhancement when contrast is indicated for other reasons. 2 Bone marrow edema on fluid-sensitive sequences usually preceded the formation of the cysts and was considered a strong predictor of their development. 5 Follow-up CT scans allowed for more accurate sizing and localization of the cyst (Figure 3), with its higher spatial resolution also allowing for evaluation of location and extent of intra-articular breach. A cyst size of ≥0.5 cm3, contained within stable borders, was required for treatment with bone grafting, measured on coronal, axial, and sagittal CT views. Acetabular cysts of all locations were treated with bone grafting. Cysts that measured <0.5 cm3 were treated with microfracture without bone grafting. Patients with fluid signal or other masses that could not be definitively characterized as cysts were referred to an orthopaedic oncologist for evaluation of potential malignancy.

Pre- and postoperative magnetic resonance imaging (MRI) scans of the right hip. (A) Preoperative coronal T2 MRI arthrogram demonstrating an acetabular bone cyst (white asterisk) in the superior weightbearing portion. (B) Preoperative axial T2 MRI arthrogram demonstrating an acetabular bone cyst (white asterisk) with the loculated pattern. (C) Preoperative sagittal T2 MRI arthrogram demonstrating an acetabular bone cyst (white asterisk) with articular cartilage breach. (D) Postoperative coronal T2 MRI scan demonstrating complete cyst healing and remodeling (yellow asterisk) with excellent fibrocartilage fill of articular cartilage defect. (E) Postoperative axial T2 MRI scan demonstrating complete cyst healing and remodeling (yellow asterisk) with resolution of loculations. (F) Postoperative sagittal T2 MRI scan demonstrating complete cyst healing and remodeling (yellow asterisk) with excellent fibrocartilage fill of articular cartilage defect. a, acetabulum; AIIS, anterior inferior iliac spine; FH, femoral head; L, labrum; Post Op, postoperative; Pre Op, preoperative.

Preoperative radiographic studies. (A) Anteroposterior radiograph of the right hip demonstrating a large acetabular complex subchondral cyst complex (yellow arrow) with articular communication (yellow asterisk). (B) Coronally reformatted computed tomography (CT) scan of the right hip demonstrating a loculated acetabular subchondral cyst with clear articular communication (yellow asterisk). (C) Axial CT scan of the right hip demonstrating an acetabular subchondral cyst with loculated appearance (yellow asterisk). (D) Sagittal CT scan of the right hip demonstrating a loculated acetabular subchondral cyst in the superior weightbearing region (yellow asterisk). a, acetabulum; AIIS, anterior inferior iliac spine; FH, femoral head; PW, posterior wall.
Surgical Technique
The senior author’s (O.M.D.) preferred techniques for hip arthroscopy 19 and cyst grafting 7 have previously been described, but the device used was improved over the course of this study (Figure 4; Supplemental Video 1, available separately). During central compartment evaluation, the area of the suspected intra-articular breach was inspected for change in color or texture. If the cyst opening was not fully exposed visually, the suspected area, based on CT and MRI findings, was gently probed with a blunt instrument to reveal the accurate localization of the intra-articular breach. The damaged cartilage alone was then sharply excised using angled curettes, and the underlying articular breach was exposed. Next, a curved microfracture pick was introduced into the cystic cavity to remove the soft tissue lining and other contents. After this, microfracture was performed into the internal cystic walls (Phoenix; Stryker) to stimulate release of bone marrow elements. Labral treatment (debridement/repair/reconstruction) was then performed as indicated.
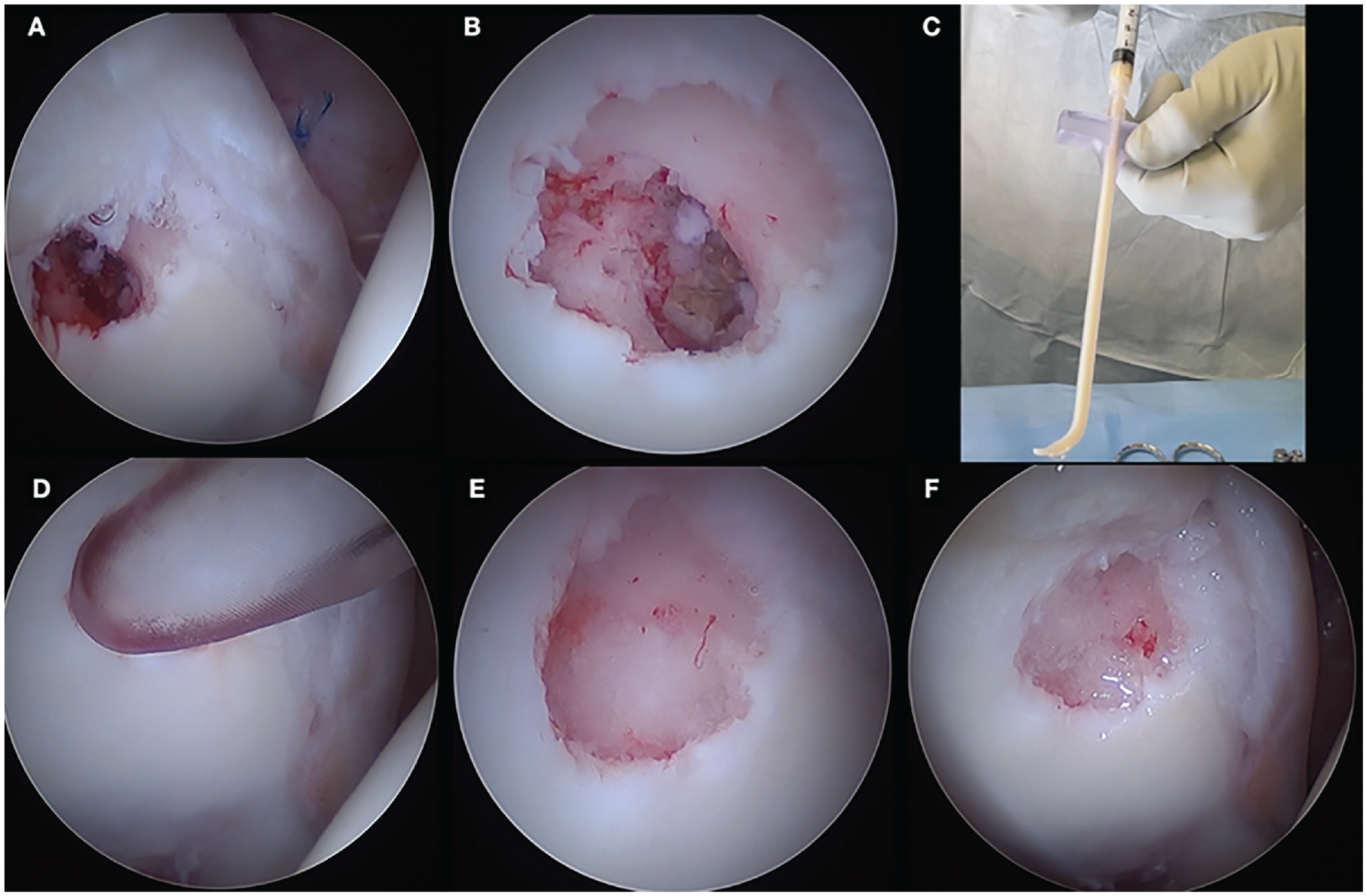
Surgical steps for inside-out bone grafting. (A) The cystic opening after clearing the soft tissue liner viewed through an arthroscope. (B) The cystic opening after removing the surrounding unstable cartilage and microfracturing in and around the cavity. (C) Loaded bone graft into the delivery tool before delivery. (D) Delivery of the bone graft under minimal water pressure. (E) Arthroscopic image of the acetabular cyst after grafting under wet conditions. (F) Arthroscopic image of the acetabular cyst under dry conditions.
Next, bone graft was delivered into the cystic cavity using a designated device before attention was directed to the peripheral compartment. The bone graft material used was based on availability and location of the surgery: PROGENIX Demineralized Bone Matrix (DBM) Putty, DuPuy Synthes DBM Bone Putty, or BioMet DBM in a lipid carrier. Excess graft, if any, was evacuated from the joint using a shaver placed away from the cyst region, and traction was then released.
Postoperative Rehabilitation
Postoperative precautions were predicated on the size and location of the cyst as well as any underlying dysplastic characteristics. In patients with dysplasia or cysts >1 cm3, we recommended limited weight bearing to “toe touch” for 4 to 6 weeks post-operatively. 3 Smaller cysts in patients with FAI were treated with weightbearing as tolerated using crutches for stability for 2 weeks post-operatively, provided that extensive microfracture was not performed and cartilage was overall healthy around the cyst opening. Standard hip arthroscopy rehabilitation was then commenced with return to play allowed 4 to 6 months postoperatively, depending on the duration of limited weightbearing and ability to regain muscle strength and control. Follow-up radiographs were obtained at 6 weeks postoperatively and at later intervals, especially if a staged realignment procedure, such as a PAO, was performed subsequently.
Outcome Measures
Detailed demographic data were collected for all patients who underwent bone grafting. Patient-reported outcomes (PROs) were assessed via the Nonarthritic Hip Score (NAHS) 4 and the iHOT-12. 8 Outcome scores were obtained via questionnaire preoperatively and postoperatively at 1.5-, 3-, 6-, and 12-month follow-up, followed by annual intervals.
Postoperative MRI was usually obtained for imaging of the contralateral hip. These studies were available at variable intervals and, when available, were evaluated for evidence of cyst healing. Evidence of cyst healing was defined as decreased intracystic T2 hyperintense signal reflecting decreased intracystic fluid and increased graft maturation and bone healing, a loss of margin conspicuity on T1 images reflecting incorporation of graft with native bone, and interval progression of appearance toward normal bone (Figure 2). 13 Further, resolution was defined as a lack of hyperintense T2 signal with near complete to complete change incorporation of the cyst resulting in the resemblance of normal bone.
Statistical Analysis
Descriptive statistics were performed, including a comparison of percentages, means, and standard deviations of patient (age, sex, Beighton score), radiographic, and procedural characteristics between the experimental and control groups. Linear mixed models (LMMs) were used to model differences in iHOT-12 and NAHS scores between the experimental and control groups over time. For all models, Akaike and Bayesian information criteria were calculated. A heterogeneous-autoregressive covariance structure was determined to be the most appropriate for both iHOT-12 and NAHS models. For ease of interpretability, analysis of variance is reported for each time point comparison. Estimated marginal means were calculated to evaluate differences in preoperative and latest follow-up scores between groups. Tukey P value correction was utilized to minimize type 1 error rate. All tests used alpha = .05 unless otherwise stated. All analysis was conducted in R Version 4.3.2 (R Foundation). 21
Results
A total of 38 patients (44 hips) underwent arthroscopic bone grafting during the study period (Table 1). For the bone grafting cohort, the mean (±SD) LCEA for the subgroup that underwent PAO was 16.0° (±7.0°) and 29.5° (±5.1°) for the non-PAO group (P < .001). Diagnostic, surgical, and follow-up information can be seen in Tables 2 and 3.
Patient Demographics a
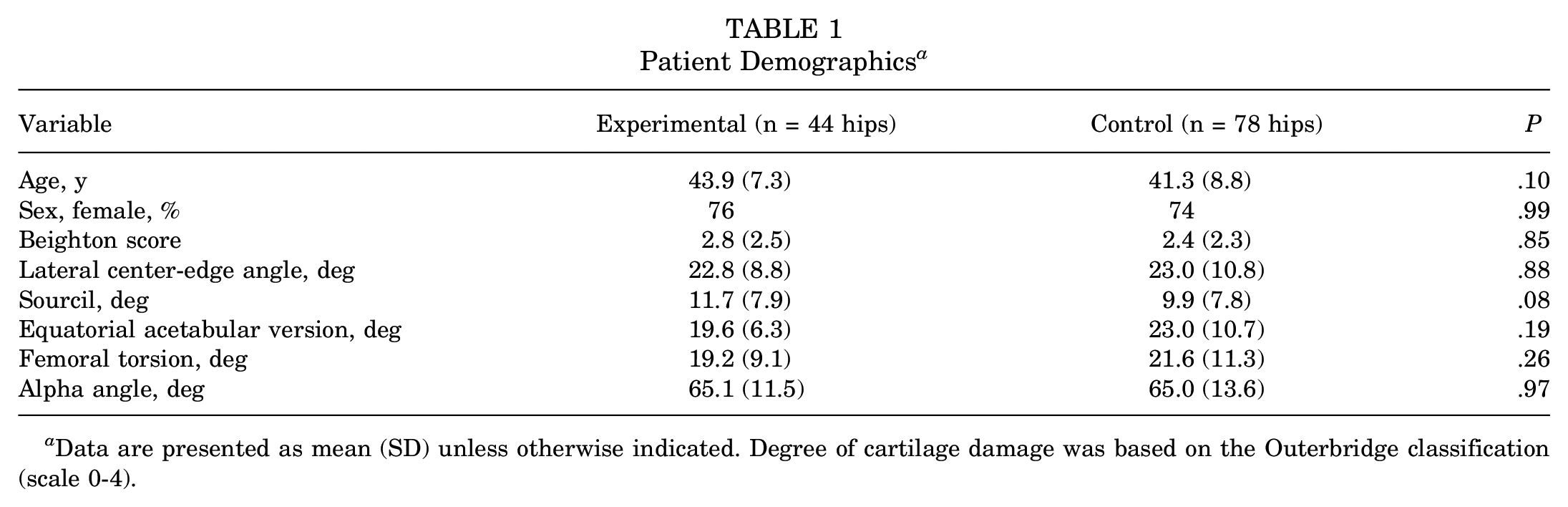
Data are presented as mean (SD) unless otherwise indicated. Degree of cartilage damage was based on the Outerbridge classification (scale 0-4).
Breakdown of FAI Types a

Data are presented as % (number of hips).. FAI, femoroacetabular impingement.
Surgical and Follow-up Information a

Data are presented as % (number of hips) unless otherwise indicated. DFO, derotational femoral osteotomy; PAO, periacetabular osteotomy; PRO, patient-reported outcome.
Indicates significance at P < .05.
Preoperative iHOT-12 and NAHS scores did not differ between the experimental and control groups (P = .53 and .83, respectively). Twenty hips (45.5%) in the grafting cohort and 26 hips (33.3%) in the control reached 5 years of postoperative PROs. Compared with preoperative values, both cohorts demonstrated a significant improvement in both iHOT-12 and NAHS scores at latest follow-up (P < .001 for both). Both the iHOT-12 (Figure 5) and the NAHS (Figure 6) LMMs did not reveal a significant difference between the experimental and control group scores over a 5-year postoperative follow-up interval (P = .26 and .17, respectively). Mean iHOT-12 scores at each time point for the experimental and control groups are demonstrated in Table 4.
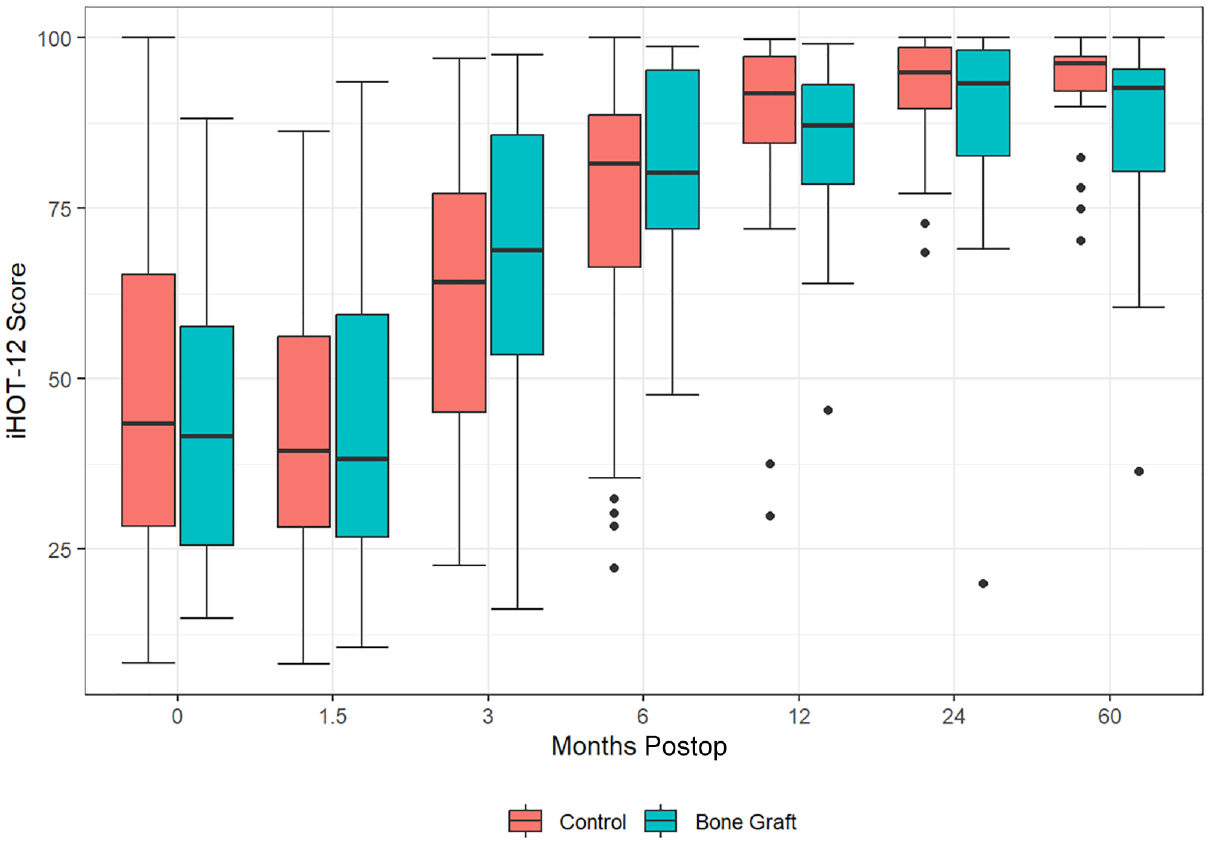
Linear mixed model of the international Hip Outcome Tool (iHOT-12) scores over time. 21 Postop, postoperative.

Linear mixed model of the Nonarthritic Hip Score (NAHS) over time. 21 Postop, postoperative.
Mean iHOT-12 Scores for the Experimental and Control Groups a

iHOT-12, international Hip Outcome Tool; Postop, postoperative.
When the acetabular cyst cohort was subdivided into PAO versus no PAO groups, both groups reported a significant increase in iHOT-12 score at latest follow-up (P < .001). Preoperative and postoperative iHOT-12 and NAHS scores for the treatment group are displayed in Table 5. The analysis of both iHOT-12 and NAHS scores over a 5-year postoperative interval did not reveal a statistically significant difference between the subgroups at any time point (P > .05).
Treatment Group PROs Separated by PAO a

Data presented as mean (SD). The postoperative score is a mean score based on latest follow-up date with a minimum postoperative follow-up of 2 years. iHOT-12, international Hip Outcome Tool–12; NAHS, Nonarthritic Hip Score; PAO, periacetabular osteotomy; Postop, postoperative; Preop, preoperative; PRO, patient-reported outcome.
During the study period, 7 of the patients who underwent grafting returned for an MRI at a mean of 19.4 (±8.7) months postoperatively. All 7 patients demonstrated evidence of cyst healing on MRI, with 3 achieving complete resolution with full graft incorporation. In some cases, susceptibility artifact from current or prior PAO hardware made assessment of the region impossible, but visualization was possible in some cases. While there was insufficient postoperative imaging in the current cohort to make a conclusive statistical statement, the expected changes were routinely seen in the subset of patients where postoperative imaging allowed adequate visualization of the cyst cavity.
Finally, there were no instances of intra- or postoperative patient safety events while utilizing this surgical technique for acetabular bone grafting. No patients in the experimental or control cohorts converted to THA during the study period.
Discussion
The most important finding of our study was that arthroscopic bone grafting, utilizing an inside-out technique, was efficacious for the management of acetabular cysts, with statistically equivalent midterm outcomes in comparison with a case-matched control group of patients without acetabular cysts. To emphasize our clinical outcomes, we demonstrated MRI evidence of at least partial cyst healing following bone grafting in 100% of patients with postoperative MRIs available. Furthermore, we reported successful patient outcomes using this technique in patients who underwent subsequent PAO. The experimental PAO cohort achieved significantly improved outcomes compared with preoperative PROs, comparable with patients who had a PAO without bone grafting. We believe our results may encourage surgeons to utilize this inside-out technique and consider pursuing hip preservation surgery in select patients with acetabular cysts.
Acetabular intraosseous cysts are frequently encountered in young adults with FAI or dysplasia and are commonly associated with the development of early and advanced arthritis.3,10,15 In the microinjury theory of subchondral cyst development, microtrauma (as caused by conditions such as FAI or dysplasia) creates fissures in articular cartilage. 22 Subsequently, increased intra-articular pressure leads to intrusion of synovial fluid into the subchondral bone through these fissures. A second, macroinjury theory states that cyst development is the product of bone necrosis resulting from the violent impact of 2 joint surfaces that have lost their articular cartilage. 22 Hartigan et al 9 demonstrated that 59% of patients with an acetabular cyst had an associated grade 3 or 4 cartilage defect of the femoral head and the acetabulum, which was not commonly found on the femoral head in our cohort. Despite this, there is a proportion of patients who present with acetabular cystic changes without substantial arthritis, as in our cohort. For these patients, with maintained joint space and overall healthy femoral head and acetabular cartilage, consideration of hip preservation is important, as we show that carefully selected patients can maintain their native hip following this treatment. Mechlenburg et al 18 revealed the need for bone grafting alongside PAO in cases of hip dysplasia with concomitant acetabular cysts, as they reported that 7 of 13 patients with acetabular cysts demonstrated increased cyst volume 10 years after PAO.
Kumar et al 16 demonstrated that patients with acetabular cysts have increased pain, symptoms, disability, and functional impairment when compared with patients without cysts, which was not supported by our findings, as we demonstrated insignificant differences in preoperative iHOT-12 and NAHS scores between the experimental and control groups. Other authors have shown an association between the presence of subchondral cysts and worse surgical outcomes. 15 In a cohort study of 104 patients undergoing hip arthroscopy for FAI, without treatment of acetabular subchondral cysts, Krych et al 15 reported an overall success rate of 67% for patients with subchondral edema or cystic changes, compared with 85% in the control group. Additionally, they reported significantly lower 2-year postoperative mean Harris Hip Score and Hip Outcome Score results for patients with subchondral cystic changes when compared with control. Contrary to this, we demonstrated that favorable outcomes are attainable, comparable with patients without acetabular cysts, even in patients with concomitant hip dysplasia. The need for bone grafting to treat subchondral lesions is further emphasized by outcome studies in other joints, especially osteochondral defects of the talus.17,23
There are a variety of surgical methods described in the literature to manage acetabular cysts.1-3,6,11,16 Field et al 6 described the utilization of an outside-in technique for management of cystic changes of the acetabular roof in 4 patients. The authors utilized fluoroscopic guidance to access the cystic space through the ilium. The cystic cavity was then filled with a synthetic osteochondral plug, flush with the acetabular articular surface. While all 4 patients reported improvement in symptoms and function at latest follow-up, 1 patient had persistent groin and buttock pain and required revision arthroscopy at 5 months postoperatively. Jamali et al 11 described an all-arthroscopic technique for bone grafting of acetabular rim cysts at the conclusion of arthroscopic acetabuloplasty and/or femoroplasty for FAI. When recontouring the acetabular rim, the authors were able to gain visualization and debride and graft the cyst utilizing a slotted cannula. Alwood and Giordano 1 detailed acetabular cyst grafting through a hole drilled in the acetabular rim, utilizing a mixture of autologous bone marrow aspirate from the femoral metaphysis, bone marrow aspirate concentrate, and cartilage-derived graft. However, these approaches all use an outside-in technique, which complicates the ability to locate and clear the contents of the cystic lesion found deeper toward the center of the acetabulum due to its complex 3-dimensional structure. Further, outside-in techniques result in significant collateral damage to healthy tissue surrounding the cyst and utilize excess radiation. We believe the utilization of an outside-in method fails to provide simple and direct cyst access. Further, this technique can delay healing due to increased iatrogenic bony cavities around the cyst, preventing compaction and consolidation of bone graft material, which may result in persistent pain or cyst recurrence.
Recent studies have sought to address the shortcomings of an outside-in approach, describing techniques that enter the damaged cartilage at the chondral interface.3,7 Bessa et al 3 described treatment of acetabular subchondral cysts with the technique of an acetabular subchondroplasty with injection of bone substitute material using fluoroscopic and arthroscopic guidance. While less invasive than previously described techniques, the authors were not able to decompress the cyst and place the graft under direct visualization, which may result in incomplete decompression and suboptimal placement of the graft.
As previously described by Garabekyan et al, 7 we performed an inside-out method, utilizing a curved delivery device to access the cyst space for grafting (Figure 4; Supplemental Video 1, available separately). Contrary to previous approaches, an inside-out technique enables direct visualization of the cyst space for decompression and graft placement. Further, we allowed for preservation of the extra-articular cyst wall, enabling increased cyst pressurization with the graft and foregoing the need for additional rim trimming for cyst access. Obviating the need for acetabular rim trimming is advantageous when treating patients with concomitant hip dysplasia or borderline dysplasia because it allows for preservation of the acetabular volume and maintains capsulolabral junction integrity, reducing adhesion rates. 27 Given the propensity for dysplastic hips to develop subchondral cysts,10,15 this technique is advantageous in these cases.
While we typically relied on clinical course to monitor postoperative progression, 7 patients in the experimental cohort underwent postoperative MRI. All 7 patients demonstrated evidence of graft incorporation and partial cystic healing, with 3 demonstrating evidence of complete healing, at a mean follow-up of <2 years postoperatively. Kang et al 13 previously published data indicating that similar grafts often take up to 3 years for full incorporation on MRI. While the percentage of our cohort that underwent postoperative MRI was small, we believe these favorable imaging findings provide further evidence, in conjunction with our clinical data, supporting the efficacy of arthroscopic inside-out acetabular cyst grafting.
For optimal management of acetabular cysts, it is important to address both the cysts and the underlying mechanism—that is, the FAI and/or dysplasia contributing to cartilage damage and subsequent cyst development. When compared with other surgical options, we believe an inside-out method to be advantageous, given the ability for articular-sided access, direct cyst visualization, and management of contributing FAI or dysplasia.
Limitations
The limitations of this study should be noted. First, this was a retrospective review of prospectively collected data without a multivariate analysis or a control group of patients with acetabular cysts who did not undergo bone grafting. Further, our cohort consisted of a heterogeneous group of patients with dysplasia and FAI. PAO may result in a change of weightbearing distribution through the acetabulum, possibly contributing to cyst healing. In addition, we included a relatively small sample size of patients who underwent hip arthroscopy with a single high-volume hip preservation surgeon (O.M.D.). Acetabular cyst treatment was not randomized; therefore, it was difficult to determine the proportional degree of improvement due to cyst grafting. Only 7 patients underwent postoperative MRI, and imaging findings may have been affected by metal artifact. Finally, several potential confounders (demographic data, biometric data, etc) were not analyzed in the study.
Conclusion
Acetabular subchondral cysts treated with an inside-out method of arthroscopic bone grafting in the setting of hip preservation surgery with or without PAO was associated with a significant improvement in midterm PROs, comparable with a control group of patients without acetabular cysts who did not undergo bone grafting. Our results support the use of arthroscopic grafting in appropriately selected patients and suggest that hip preservation is not contraindicated in patients with acetabular subchondral cysts.
Footnotes
Final revision submitted August 27, 2024; accepted August 30, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.N.M. holds stock or stock options in Pfizer and Roche and is a board or committee member for the Radiological Society of North America. O.M-D. owns stock or stock options in HeapSI and MITA, receives IP royalties from Stryker, and has received consulting fees from Stryker. J.H.L. has received hospitality payments from Smith+Nephew, Stryker, and Heraeus Medical and education payments from Gemini Mountain Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Colorado Multiple Institutional Review Board (IRB No. CRV006-1).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.