
Abstract
Background:
Magnetic resonance imaging (MRI) measurement parameters—the standard noninvasive diagnostic method for rotator cuff tears (RCTs)—have been used to compare groups with and without RCTs. Arthroscopy is used in definitive diagnosis and treatment.
Purposes:
To evaluate the association between RCT and shoulder angles and distances on MRI in patients with and without arthroscopically validated RCT and to determine whether the degree of rotator cuff fatty degeneration affects the MRI measurements.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Shoulder measurements on MRI were compared between patients with and without RCT as confirmed by shoulder arthroscopy performed by a single surgeon between 2019 and 2024, and non-RCT patients without arthroscopic confirmation. Interobserver reliability (Fleiss kappa coefficient) was calculated for the measurements. The groups were compared using the independent t test or the Mann-Whitney U test. The RCT group was further divided according to the level of fatty degeneration (Goutallier types 0-1-2 vs types 3-4) for subanalysis.
Results:
In addition to the 368 RCT and 55 non-RCT patients with arthroscopic confirmation, there were 92 non-RCT patients without arthroscopic confirmation. The sagittal acromiohumeral interval (AHI) (8.32 vs 9.24 mm), coronal AHI (7.87 vs 8.96 mm), and coronal AHI/glenoid height ratio (22.63% vs 24.88%) were significantly lower in the patients with RCT (P < .001, P < .001, and P = .001, respectively). In contrast, the critical shoulder angle (CSA) (33.17° vs 31.92°) and the glenoid width/humeral head coverage ratio (57.52% vs 55.7%) were significantly higher in the patients with RCT (P = .037 and P = .017, respectively). Higher rotator cuff fatty degeneration levels (Goutallier types 3-4) further increased these differences within the patients with RCT (P < .001 for all). When the arthroscopically validated and nonvalidated non-RCT patients were compared, coronal AHI and AHI/glenoid height ratio values were found to be significantly lower in the nonvalidated group (P = .034 and P = .047, respectively).
Conclusion:
In this study, RCT was associated with decreased sagittal AHI, coronal AHI, and coronal AHI/glenoid height ratios and increased CSA and glenoid width/humeral head coverage ratios.
Rotator cuff injuries are common shoulder pathologies. The incidence of injury increases with age and has been reported to increase from 9.7% in patients aged <20 years to 62% in those aged >80 years. 25 Magnetic resonance imaging (MRI) is used as the standard noninvasive diagnostic method for rotator cuff tears (RCTs). 24 With additional measurements made on MRI, the effect of RCTs on shoulder angles and distances or the effect of measurements on RCTs can also be evaluated. ‡ In some studies, MRI measurement parameters were evaluated on patients without arthroscopic validation, and groups with and without RCT were compared.2,8,15,17,19,22,26 In their meta-analysis, Smith et al 23 reported that the sensitivity and specificity values for MRI were 0.80 and 0.95 for partial-thickness RCTs, respectively, and 0.91 and 0.97 for full-thickness tears, respectively. In their meta-analysis, Malavolta et al 16 showed that the sensitivity of MRI in subscapularis ruptures was 0.68.
İncesoy et al 13 compared critical shoulder angle (CSA), acromial index (AI), acromion angle (AA), and glenoid version angle (GVA) between arthroscopically validated RCT and nonvalidated non-RCT groups and found that these parameters were significantly related to RCTs. However, to our knowledge, arthroscopic validation has not been performed in studies other than İncesoy et al.
In this study, we aimed to evaluate the association between RCT and shoulder angles and distances on MRI in patients with and without arthroscopically validated RCT and to determine whether the degree of rotator cuff fatty degeneration affects the MRI measurements. We hypothesized that the accuracy of the results could be increased by eliminating the false-negative effects of MRI with the help of arthroscopy.
Methods
Patient Selection
After obtaining institutional review board approval for the study protocol, we retrospectively reviewed the records of patients who underwent arthroscopic shoulder surgery by the lead author (G.I.) between January 2019 and February 2024. Patients aged ≥18 years who underwent shoulder arthroscopy were included in the study. The exclusion criteria were age <18 years; presence of bony Bankart lesion, adhesive capsulitis, and inflammatory disease; previous surgery on the same shoulder; partial-thickness RCT; isolated subscapularis tear; or preoperative MRIs that were unavailable or unreadable. The presence of a bony Bankart lesion was an exclusion criterion because glenoid distances will vary depending on the size of the fractured bone fragment. In partial-thickness RCTs, the side of the tendon on which the tear occurred and its depth may affect the results, and thus they were excluded from the study. Since the angles and distances where the incidence of subscapularis tears is high or low and the measurement parameters in the present study are different, isolated subscapularis tears were excluded from the study. However, they were included in cases where they accompanied superior RCTs and were determined as an additional evaluation criterion.
Study Groups
Patients with arthroscopic validation were categorized into 2 groups: (1) those with RCTs and (2) those with isolated labral pathology without RCT. An additional control group was created from patients with no RCT or bony Bankart lesion detected on MRI who did not undergo arthroscopic validation. In addition to the arthroscopically nonvalidated non-RCT control group, the arthroscopically validated non-RCT group was added as a control group to prevent the false-negative effects of MRI. The RCT group was further divided according to the Goutallier classification 7 of fatty degeneration: low (types 0-1-2) or high (types 3-4).
Measurement Parameters
A total of 16 measurement parameters were examined in this study to ensure the evaluation of their effects on each other in RCTs. These parameters included acromion type (according to the Bigliani classification 1 ), AA, acromial thickness (AT), sagittal and coronal acromiohumeral interval (AHI) (Figure 1, A and B), superior glenoid inclination (SGI), 3 acromion-greater tuberosity impingement index (ATI), 14 coracoacromial ligament length (CAL), coronal AHI/glenoid height ratio (Figure 1C), AI, lateral acromial angle (LAA), acromial lateral downslope angle (ALDA), CSA (Figure 2), GVA (according to the Friedman method), 6 humeral translation (HT), and glenoid width/humeral head (HH) coverage ratio (Figure 3). As Sgroi et al 21 showed MRI could measure glenoid bone loss as accurately as computed tomography, the use of MRI in the glenoid evaluation was deemed appropriate in the present study.

(A) The sagittal AHI, measured as the narrowest distance between the inferior surface of the acromion and the superior surface of the humeral head on T1-weighted oblique sagittal MRI. (B) The coronal AHI (a), measured as the narrowest distance between the lower surface of the acromion and the upper surface of the humeral head on T1-weighted oblique coronal MRI. (C) On T1-weighted oblique coronal MRI passing through the center of the glenoid, the distance between the upper and lower corners of the glenoid gives the glenoid height (b), and the coronal AHI/glenoid height ratio is measured as a/b. In the presented case example, this ratio is 8.07/35.84 = 23%. AHI, acromiohumeral interval; MRI, magnetic resonance imaging.

The critical shoulder angle. (A) The acromion’s most lateral and inferior point is determined and marked with the cursor (a). (B) A line connecting the upper and lower corners of the glenoid is drawn in the T1-weighted oblique coronal MRI section passing through the center of the glenoid. The angle between the glenoid lower corner of the drawn line and the first cursor gives the critical shoulder angle (b). MRI, magnetic resonance imaging.
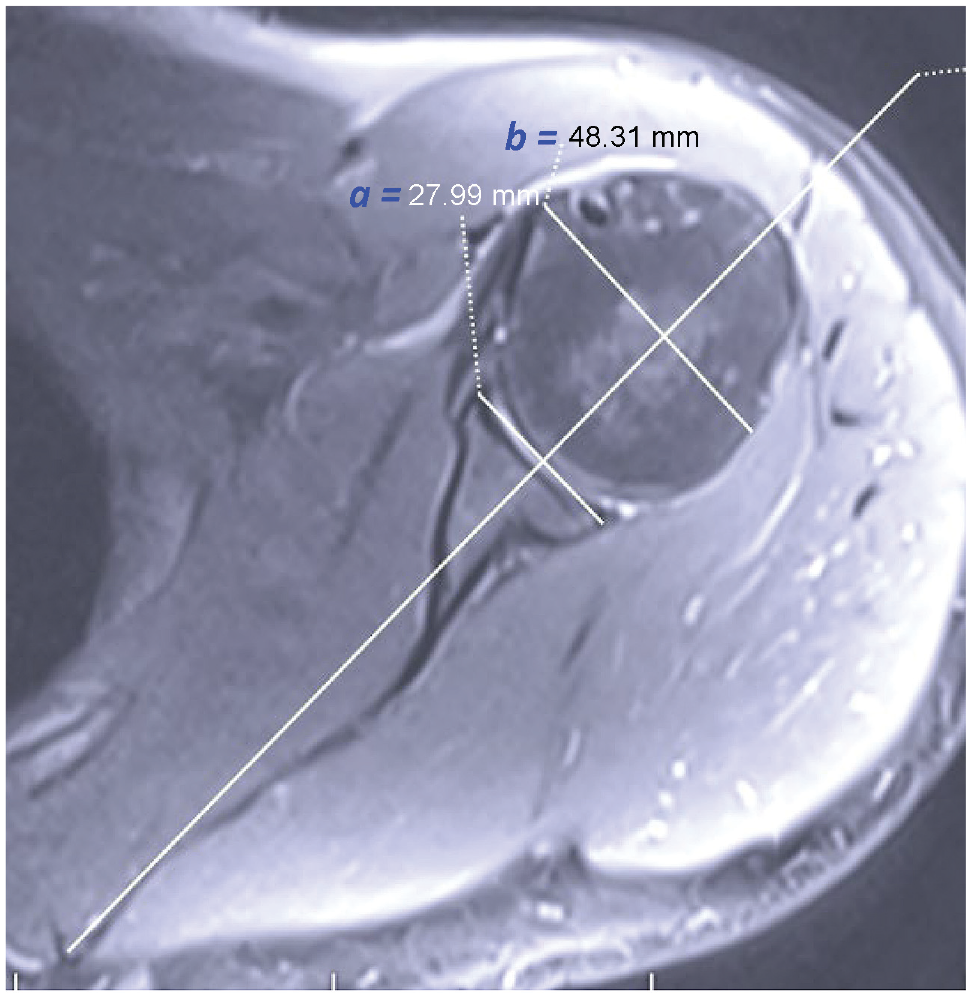
The glenoid width/humeral head coverage ratio. On axial MRI passing through the center of the glenoid, the ratio of the distance between the anterior and posterior bone corners of the glenoid (a) and the distance between the anterior and posterior humeral head (b) gives the glenoid width/humeral head coverage ratio (a/b). In the presented case example, a ratio of 27.99/48.31 = 58% was found. MRI, magnetic resonance imaging.
Two observers (E.E. and F.B.I.) reviewed all parameter measurements using the same picture-archiving communication system. All MRI scans were performed at 2-mm intervals, in the neutral position, with a 1.5-T unit (Siemens Magnetom Aera). Measurements were performed on the existing Fonet Dicom Viewer v4.1 (Fonet Bilgi Teknolojileri); no additional software was needed. While making measurements, T1- and T2-weighted axial, oblique coronal, and oblique sagittal sections were used. MRI views that were not at the appropriate angle were excluded from the study. Interobserver reliability was evaluated, and cutoff values were calculated for parameters that provided adequate agreement in interobserver evaluations (κ > 0.6) and were significantly different between groups.
Statistical Analysis
SPSS (Statistical Package for the Social Sciences) Version 24 (IBM Corp) was used for the statistical analysis. The chi-square and Fisher exact tests were applied to categorical data. Depending on the results of normality analysis with the Shapiro-Wilk test, an independent t test or the Mann-Whitney U test was used for comparisons between the study groups (RCT group, a non-RCT group with arthroscopic validation, and the non-RCT group without arthroscopic validation). P < .05 was considered statistically significant. The Fleiss kappa (κ) coefficient was used to calculate the interobserver reliability of the MRI measurements. The κ values were interpreted as slight (0-0.2), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), and almost perfect (0.81-1).
Post hoc analysis was performed using the G*Power 3.1.9.7 program (Heinrich-Heine-Universität).
Results
Patient Characteristics
A total of 612 patients who underwent arthroscopic shoulder surgery and 223 patients who did not have arthroscopic validation were reviewed within the scope of the study. Following the exclusion criteria, 423 (69%) patients with arthroscopic validation were categorized into 2 groups; there were 368 patients with full-thickness RCTs and 55 patients with labral pathology but no RCT in the non-RCT with arthroscopic validation group. In addition, 92 (41%) patients were included in the non-RCT without arthroscopic validation group. A flow chart of the patient inclusion process is shown in Figure 4.

A flowchart of patient inclusion in the study. MRI, magnetic resonance imaging; RCTs, rotator cuff tears; Ss, subscapularis.
The mean age of the RCT group (n = 368) was 53.4 ± 13.7 years, the mean age of the arthroscopically validated non-RCT group (n = 55) was 49 ± 16.2 years, and the mean age of the nonvalidated non-RCT group (n = 92) was 50.5 ± 15.9 years; no significant difference between the groups was detected in terms of personal characteristics or acromion type according to the Bigliani classification (Table 1).
Patient Characteristics and Acromion Morphology Overall and According to Study Group a

Data are presented as mean ± SD (range) or No. of patients. RCT, rotator cuff tear.
According to the Bigliani classification. 1
When patients in the RCT group were subgrouped according to the Goutallier classification, there were 172 patients with low fatty degeneration (types 0-1-2) and 196 patients with high fatty degeneration (types 3-4). The mean number of affected rotator cuff tendon injuries in the low-fatty degeneration group was 1.19, compared with 2.25 in the high-fatty degeneration group. Supraspinatus tears were detected in 319 (87%) patients in the RCT group. All patients in the high-fatty degeneration group were found to have supraspinatus tears; in addition, teres minor pathology was not detected in any patient in the low-fatty degeneration group (Figure 5).

The number of tendon tears in the RCT subgroups according to the Goutallier fatty degeneration type. RCT, rotator cuff tear.
Measurement Parameters, Reliability, and Cutoff Values
Sagittal AHI, coronal AHI, AT, AI, CSA, GVA, coronal AHI/glenoid height ratios, and glenoid width/HH coverage ratios had sufficient interobserver reliability (substantial or almost-perfect agreement), but SGI, ATI, CAL, HT, AA, LAA, and ALDA coverage ratios did not have sufficient reliability (slight to moderate agreement) (Table 2).
Interobserver Reliability Values a
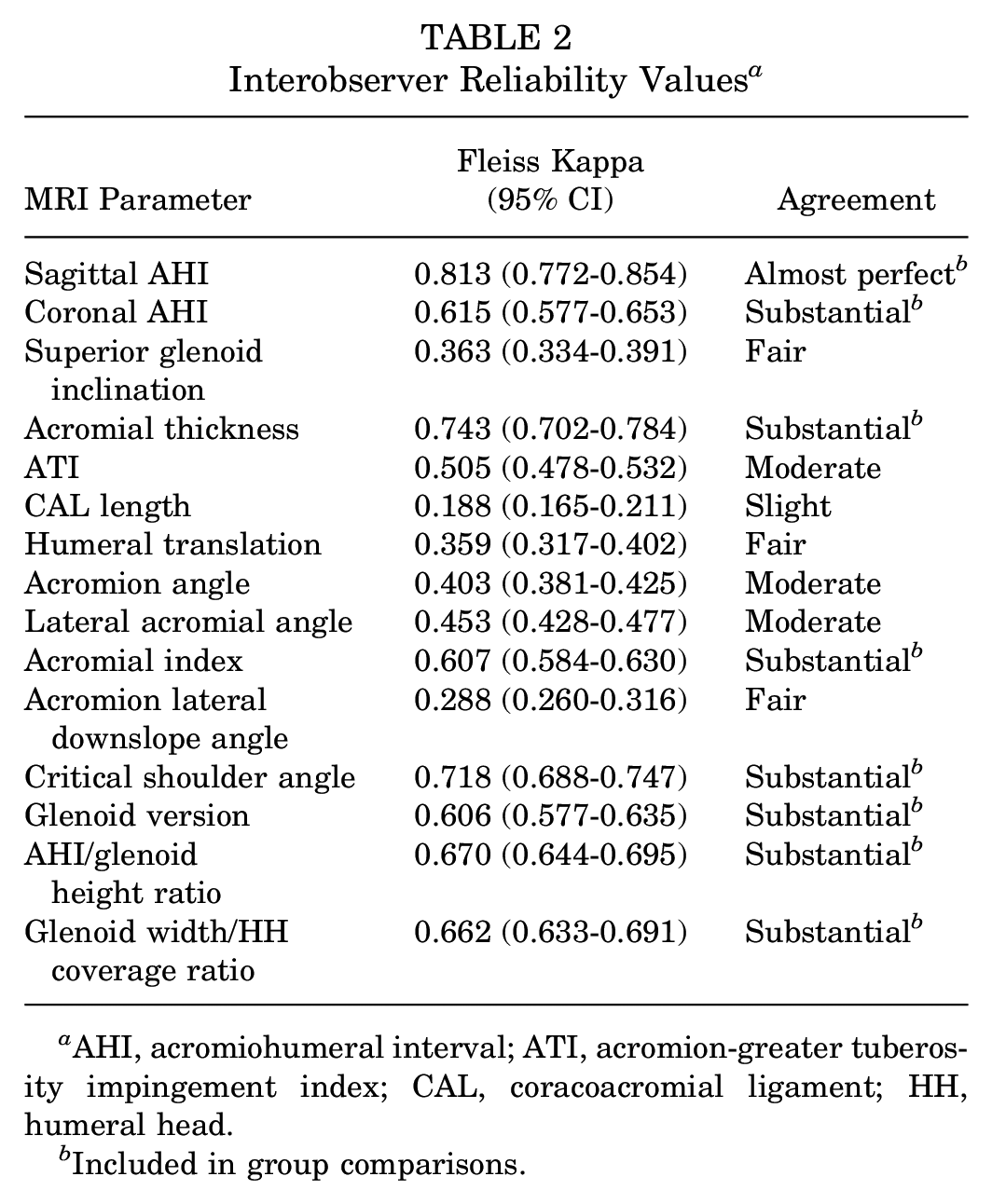
AHI, acromiohumeral interval; ATI, acromion-greater tuberosity impingement index; CAL, coracoacromial ligament; HH, humeral head.
Included in group comparisons.
The 8 MRI parameters with sufficient interobserver reliability were included in the group comparisons. When the RCT and arthroscopically validated non-RCT groups were compared, sagittal AHI, coronal AHI, and coronal AHI/glenoid height ratios were found to be significantly lower in the RCT group (P < .001, P < .001, and P = .001, respectively), while CSA and glenoid width/HH coverage ratios were significantly higher (P = .037 and P = .017, respectively). No significant difference was found between the groups in terms of AT, AI, and GVA (Table 3).
Comparison of Parameters With Sufficient Interobserver Reliability Values Between Groups a
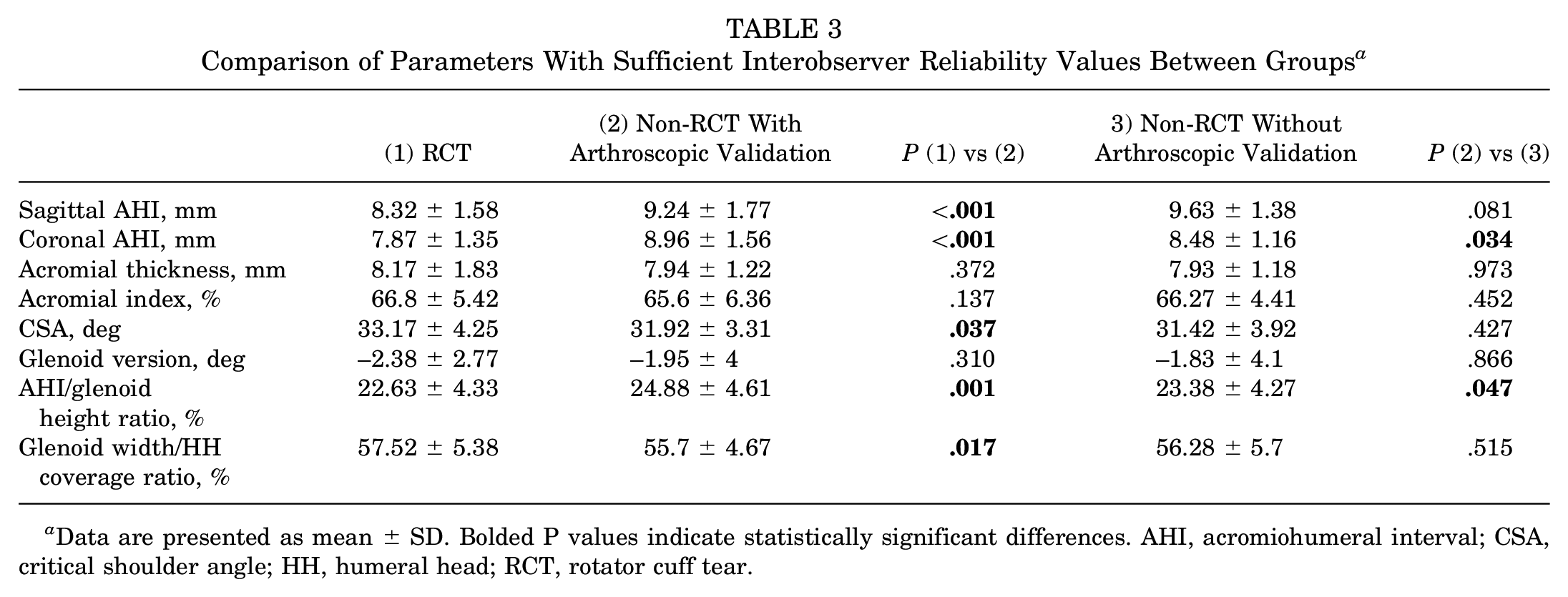
Data are presented as mean ± SD. Bolded P values indicate statistically significant differences. AHI, acromiohumeral interval; CSA, critical shoulder angle; HH, humeral head; RCT, rotator cuff tear.
Although no differences were detected in many values when the arthroscopically validated and nonvalidated non-RCT groups were compared, coronal AHI and AHI/glenoid height ratio values were found to be significantly lower in the nonvalidated group (P = .034 and P = .047, respectively) (Table 3).
Cutoff values of the parameters that were found to be significantly different between the RCT and non-RCT groups were calculated. A sagittal AHI of <8.59 mm, a coronal AHI of <8.2 mm, and an AHI/glenoid height ratio of <23.4% were in favor of damage to the rotator cuff. However, a CSA of <32.5° and a glenoid width/HH coverage ratio of <56.1% were in favor of an intact rotator cuff (Table 4).
Cutoff Values of Parameters With Significant Differences Between the RCT and Non-RCT Groups a

AHI, acromiohumeral interval; AUC, area under the curve; CSA, critical shoulder angle; HH, humeral head; RCT, rotator cuff tear.
Effect of Fatty Degeneration on MRI Parameters
When the 5 parameters with significant differences between the groups with and without tears were compared within the subgroup of patients with RCT according to the Goutallier stage, sagittal AHI, coronal AHI, and AHI/glenoid height ratios showed lower values as fatty degeneration increased (P < .001 for all), but CSA and glenoid width/HH coverage ratios showed higher values (P < .001 for both) (Table 5). When the group containing Goutallier type 3-4 patients was compared with the non-RCT group, the AI value was found to be significantly higher in the tear group (P = .022).
Comparison of Parameters Showing Significant Differences Between Groups According to Goutallier Stage a

Data presented as mean ± SD. AHI, acromiohumeral interval; CSA, critical shoulder angle; HH, humeral head.
Post Hoc Analysis
In post hoc analysis, when the RCT group and the arthroscopically validated non-RCT group were evaluated, power (1 –β) was calculated as 0.958 (sample size [n1 = 368 – n2 = 55]; effect size d = 0.5; and an error probability = 0.05). When the non-RCT groups were evaluated between themselves, the power (1 –β) was calculated as 0.886 (sample size [n1 = 55 – n2 = 92]; effect size d = 0.5; and an error probability = 0.05).
Discussion
The major finding in the present study, which investigated whether RCTs and degree of fatty degeneration changed shoulder angles and distances, was that sagittal AHI (8.32 vs 9.24 mm), coronal AHI (7.87 vs 8.96 mm), and coronal AHI/glenoid height ratios (22.63% vs 24.88%) were significantly lower in the presence of RCTs (P < .001, P < .001, P = .001, respectively), while CSA (33.17° vs 31.92°) and glenoid width/HH coverage ratios (57.52% vs 55.7%) were found to be significantly higher in patients with RCTs (P = .037 and P = .017, respectively). Also, higher rotator cuff fatty degeneration levels (types 3-4) further increased these differences (P < .001 for all). In addition, when the arthroscopically validated and nonvalidated patients without rotator cuff pathology were compared, coronal AHI and AHI/glenoid height ratio values were found to be significantly lower in the nonvalidated group (P = .034 and P = .047, respectively). The reason for this situation might be that the MRIs showed false-negative results.
İncesoy et al 13 compared arthroscopically validated RCT and arthroscopically nonvalidated non-RCT patients on MRI. They found that in the RCT group, the mean AI was 70%, the CSA was 33.6°, and the GVA was –3.5°, while in the control group, the mean AI was 60%, the CSA was 31.5°, and the GVA was –2.2° (P < .001 for all). Cutoff values were calculated as 60% for the AI, 31.4° for the CSA, and –2.6° for the GVA. In the comparison between the arthroscopic validation groups with and without RCT, although it was observed that the AI was higher and the GVA was more retroverted in the tear group in the present study, no statistically significant differences were detected between the 2 groups (P = .137 and P = .31, respectively). Similar to the mentioned study, the CSA was found to be high in the tear group (P = .037), but the cutoff value was calculated as 32.5°. The reason for this difference may be that they did not separate the tear group according to the level of fatty degeneration in the mentioned study. In the present study, when the group containing Goutallier type 3-4 patients was compared with the non-RCT group, the AI value was found to be significantly higher in the tear group (P = .022).
When examining MRI studies that were not validated arthroscopically, similar and different evaluations than those in the present study were found. Gulcu et al 8 found that CSA, AI, ATI, and SGI increased statistically significantly in the RCT group compared with the control group, while LAA and AHI decreased. Çağlar et al 2 found that AI, CSA, ATI, and AA were higher in the RCT group, and AHI, LAA, and GVA were higher in the non-RCT group. What is noteworthy among these studies is that ATI varies between groups (0.82 vs 0.838, 0.83 vs 0.912). The reason for this difference may be that in the second study, the entire population consisted of full-thickness tears, whereas in the first study, a large portion of 36% consisted of partial tears. In the present study, CSA and AHI values were similar to those of the mentioned studies (P = .037 and P < .001, respectively). AI and GVA values did not create a statistically significant difference between the groups in the present study (P = .137 and P = .31, respectively). ATI, SGI, AA, and LAA evaluations were excluded from the study because of the low interobserver reliability (κ = 0.505, 0.363, 0.403, and 0.453, respectively). Schiefer et al 20 showed that CSA and AI had high intra- and interobserver agreement in MRI measurements. Substantial agreement was found for both measurements in the present study (κ = 0.718 and 0.607, respectively).
Ma et al 15 found that CSA and AI were higher in the RCT group. In another study, 19 similar to other MRI studies, AT and AI were found to be high in the RCT group, and AHI and LAA were found to be high in the control group.
Similarities were observed between the results of the MRI studies in other measurement parameters, but while the AI was similar between both groups in the study by Yılmazturk et al, 26 it was found to be high in the RCT group in other studies. In the present study, although the AI value did not create a statistically significant difference between the RCT and non-RCT groups (P = .137), when the RCT group was divided into subgroups according to the fatty degeneration level, a significant difference was observed with the progression of the stage (P = .022). Although CSA and AHI results were similar to MRI studies (P = .037 and P < .001, respectively), no difference was detected between groups for AT (P = .342), while interobserver reliability was found to be low for the LAA (κ = 0.453). The results of these MRI-based studies, which yielded different results from the present study in some parameters, might be due to the false negativity of MRI since arthroscopic confirmation was not performed.
In another arthroscopically nonvalidated MRI study that evaluated relatively different measurements than the others, Matcuk et al 17 determined that the AT and the ALDA were statistically higher in the RCT group, and the CAL and the AHI were higher in the non-RCT group (P < .01 for all). They found no statistical difference between the groups in terms of AA, HT, and GVA. In the present study, ALDA, CAL, AA, and HT values were excluded from the study because of the low interobserver reliability (κ = 0.288, 0.188, 0.403, and 0.359, respectively). While no statistically significant difference was detected for the AT (P = .372), other parameters were observed to be compatible with this study.
Siow et al 22 showed that the increase in the number of torn tendons in the rotator cuff was negatively correlated with the AHI distance. Moreover, it was shown that the decrease in AHI was greater in isolated infraspinatus lesions than in isolated supraspinatus tears (P = .047). In the present study, the mean number of ruptured tendons was 1.19 (205/172) in the group with low-fatty degeneration (Goutallier types 0-1-2) compared with 2.25 (441/196) in the group with high-fatty degeneration (types 3-4) (P < .001). It was observed that as fatty degeneration increased, sagittal AHI, coronal AHI, and AHI/glenoid height ratios decreased, while CSA and glenoid width/HH coverage ratios increased. Since no isolated infraspinatus tear was detected in the high-fatty degeneration group, a specific evaluation of the tendons could not be made.
Among studies conducted with conventional radiography, Cunningham et al 5 calculated the mean CSA angle as 36.7° in the RCT group and 32.1° in the non-RCT control group (P < .001). Similarly, Hsu et al 11 showed that CSA was higher in the supraspinatus tendinopathy group than in the control group (P < .001). Similarly, in the present MRI study, the CSA was found to be higher in the RCT group than in the non-RCT group (P = .037). However, the values were found to be lower compared with radiography studies (33.17°± 4.25° vs 31.92°± 3.31°). The reason for this difference might be that the measurement technique in the MRI study was different from radiography.
When comparing MRIs with conventional radiographs, 12 the AHI is smaller because MRIs are performed in the supine position. In the present study, no comparison was made with radiographs, but a comparison was made between shoulder MRIs of patients with and without RCT.
Limitations
The main limitation of the study is that since some parameters could not be determined on a single cross-section, measurements were made by marking them and transferring them to the other cross-sections. Another limitation was that measurements from MRI views were not compared with radiographs. In addition, since MRIs are performed at 2-mm intervals as a standard, a better measurement can be made with thinner section views. Another limitation is the lack of functional status evaluation and only morphological MRI evaluations with arthroscopic data. Although interobserver reliability was assessed, the lack of intraobserver reliability was a limitation. The fact that the patients underwent surgery at a single center and all surgeries were performed under the leadership of the lead author can be stated as a limitation, which can be prevented by conducting a multicenter study.
Conclusion
Our study demonstrated that RCTs are associated with decreased sagittal and coronal AHI and coronal AHI/glenoid height ratios and increased CSA and glenoid width/HH coverage ratios.
Footnotes
Final revision submitted July 11, 2024; accepted July 30, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Usak University (ref No. 318-318-17).