
Abstract
Background:
Ramp lesions (RLs) associated with anterior cruciate ligament (ACL) injury increase knee instability. However, whether RLs should be treated surgically remains unclear.
Purpose/Hypothesis:
This study aimed to investigate the presence of RLs and compare the knee stability between patients who underwent surgical repair for unstable RLs and those who received nonoperative management for stable RLs. It was hypothesized that there would be a correlation between RLs and knee instability and that RL repair would improve postoperative knee stability.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Overall, 180 patients who underwent primary ACL reconstruction using hamstring tendon graft were included in this study. The decision to perform surgical intervention for RLs was based on the size and instability of the RL. Knee stability was evaluated using the KT-1000 arthrometer for side-to-side difference at the manual maximum, as well as the Lachman and pivot-shift tests. Linear and logistic regression analyses were employed to examine factors associated with knee instability.
Results:
Arthroscopy confirmed RLs in 59 patients (32.8%), with a higher prevalence among women; of this total, 33 patients (55.9%) were treated nonoperatively and 26 (44.1%) underwent repair. Although the preoperative side-to-side difference in laxity in the patients with RL was significantly greater than that in patients without RL (P = .01), no significant clinical differences were observed for the preoperative Lachman test (P = .50) and pivot-shift test (P = .36). No secondary meniscal injuries occurred during the follow-up period. There were no significant differences in postoperative laxity between patients with and without RLs.
Conclusion:
Although the presence of RLs was associated with preoperative knee instability, contrary to the hypothesis, RLs were not associated with postoperative knee instability. Stable RLs are clinically benign lesions that may tend to heal spontaneously after appropriate anatomic ACL reconstruction. Therefore, RLs may not require aggressive treatment if they are small and stable.
Medial meniscal ramp lesions (RLs) were initially described by Hamberg et al 13 in 1983 and later termed by Strobel. 29 An RL is a peripheral longitudinal tear of the medial meniscal posterior horn around the meniscocapsular junction and is frequently associated with anterior cruciate ligament (ACL) injury. 29 The reported incidence of RLs in patients with ACL-deficient knees ranges from 9% to 41.7%, demonstrating considerable variability.21,26 Notably, Sonnery-Cottet et al 27 reported that the incidence of RLs was 40% and found that 42% of RLs were “hidden” beneath a membrane-like tissue, potentially affecting the rate of diagnosis. Similarly, the detection rate of RLs on preoperative magnetic resonance imaging (MRI) exhibits significant variation, ranging from 27.3% to 84.6%,5,33 with unknown diagnostic accuracy.
Biomechanically, RLs have been associated with knee instability, including anterior tibial translation and rotational instability, as reported in cadaveric2,11,20,28 and clinical studies.24,30 Therefore, RLs have received increased attention as a treatment target for improving ACL reconstruction outcomes. Many studies have reported excellent results in RL repair.1,10,13,15 However, RLs may heal without surgical intervention, 3 given their location in the red-red zone, a highly vascularized area. 12 Consequently, a lack of consensus persists regarding the surgical indications for RL repair and the repair approach. 1
In the current study, we aimed to investigate the presence of RLs and compare knee instability between patients who underwent surgical repair for unstable RLs and those who received nonoperative management for stable RLs. The hypothesis was that RLs would be related to knee instability and that RL repair would improve postoperative knee stability.
Methods
Study Patients
This retrospective study was approved by our institution’s ethics committee and adhered to the 1964 Helsinki Declaration and its subsequent amendments; all included participants provided informed consent. Data were collected from 376 patients who underwent ACL reconstruction between 2017 and 2020 at a single institution, Hirosaki University. These patients were diagnosed with ACL injury based on clinical and MRI findings. Of these initial patients, 196 patients were excluded for the following reasons: revision ACL reconstruction (n = 56), ACL reconstruction using grafts other than hamstring tendon (n = 35), skeletally immature cases (physeal-sparing ACL reconstruction; n = 7), chronic cases (reconstruction performed >6 months after ACL injury; n = 33), follow-up <2 years (n = 48), reinjury during follow-up (n = 14), and incomplete data (n = 3). Thus, 180 patients were ultimately included in the study. The patients were divided into 2 groups, RL− and RL+, based on the absence or presence of RL. The RL+ group was further subdivided into 2 groups: patients who underwent surgical repair and those who did not (Figure 1).

Flowchart of patient inclusion in the study. ACL, anterior cruciate ligament; HT, hamstring tendon; RL, ramp lesion.
Surgical Technique
All patients underwent anatomic double-bundle ACL reconstruction using hamstring tendon graft, as detailed in a previous report. 25 The semitendinosus tendon was harvested and divided into 2 portions for grafts on the anteromedial and posterolateral bundles. An additional gracilis tendon was harvested and added to the graft if the harvested semitendinosus was insufficiently long or thick.
Medial and lateral meniscal lesions were carefully identified by arthroscopy, and RLs were assessed by standard anterior visualization through the anterolateral portal and the modified Gillquist technique (transnotch view) using a 30° or 70° arthroscope. We defined RL as a longitudinal tear of the medial meniscal posterior horn peripheral attachment at the meniscocapsular junction. 15 RLs <10 mm long or those considered stable by probing were left unrepaired.22,31 For RLs >10 mm or unstable by probing,22,31 an inside-out vertical repair was performed using a Henning meniscal repair system (Stryker Japan), or an all-inside suture repair was performed using a curved suture passer through the posteromedial portal.
Postoperative Rehabilitation
The postoperative rehabilitation protocol was similar to that described in a previous study. 25 Weightbearing gait with crutches was allowed from the day after surgery. If combined meniscal repair was performed, the knee joint was immobilized with a brace for 1 week. Running, open kinetic chain exercises, and jump-landing training were allowed 3 months postoperatively. Patients were cleared to return to their previous sports level after 6 to 9 months, contingent on sufficient muscle recovery and balance training.
Data Collection
Demographic data, including age, sex, height, weight, body mass index (BMI), Tegner activity score, and time from injury to surgery were collected for all patients. Preoperative clinical examinations included knee stability measured as the side-to-side difference (SSD) in anteroposterior laxity using a KT-1000 arthrometer (MEDmetric Corp), the Lachman test, and the pivot-shift test, all at the manual maximum. The Lachman and pivot-shift tests were graded from 0 to 3 under anesthesia immediately before ACL reconstruction. Intraoperative data included medial and lateral meniscal tears, the presence of RL, and treatment for RL. Postoperative clinical examinations were recorded, including SSD and pivot-shift test at 24-month follow-up. The clinical examinations were performed by 2 senior orthopaedic surgeons with >20 years of experience (Y.K. and E.S.). The postoperative pivot shift was categorized as positive if the grade was ≥1.
Statistical Analysis
Demographic data for each group were reported as means with standard deviations. Due to the nonnormal distribution of some demographic parameters determined by the Shapiro-Wilk test, the Mann-Whitney U test and chi-square test were performed to compare the RL− and RL+ groups. The chi-square test or Fisher exact test was performed to examine the impact of RL presence or repair on knee instability at 1 year postoperatively.
To investigate the relationship between postoperative knee instability and preoperative presence of RL, a regression model was established, with age, female sex, BMI, Tegner score, time from injury to surgery, pivot-shift test, medial meniscal tears, lateral meniscal tears, and presence of RL as independent variables. Linear regression analysis was performed with 1-year postoperative SSD as the dependent variable, and logistic regression analysis was applied with positive postoperative pivot shift (grade ≥1) as the dependent variable and these same independent variables. Similar logistic and linear regression models were applied in the RL+ group to investigate the association among postoperative knee laxity, RL repair, and RL healing. Data inputs and analyses were performed using SPSS Version 29.0 (IBM Corp). Statistical significance was set at P < .05.
Results
Among the 180 study patients (mean age, 25.8 ± 13.0 years), RLs were observed in 59 patients (32.8%; RL+ group). Postoperative instability (positive pivot-shift grade ≥1) was seen in 10.6% of patients. No secondary meniscal injury requiring surgery occurred during the follow-up period. When comparing demographic data between the RL− and RL+ groups, no significant differences were found in age, weight, BMI, Tegner activity score, or time from injury to surgery; however, there were more women in the RL+ group compared with the RL− group (72.9% vs 57.0%, respectively; P = .77), and the RL− group was significantly taller than the RL+ group (165.3 ± 8.3 vs 162.3 ± 8.3 cm, respectively; P = .04) (Table 1).
Demographic Data of Patients According to Presence of Ramp Lesions a

Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). BMI, body mass index; RL−, no ramp lesion; RL+, presence of ramp lesion.
Notably, a significant difference in the preoperative SSD in laxity (P = .01) existed between the RL− and RL+ groups, while no significant group differences were observed on the preoperative Lachman test or pivot-shift test (P = .50 and .36, respectively) (Table 2). Among the 59 patients with RLs, 26 patients (44.1%) underwent surgical repair, while 33 patients (55.9%) were in the no-repair group. No significant differences were observed in preoperative SSD in laxity, Lachman test, or pivot-shift test between the repair and no-repair groups (P = .06, .98, and .89, respectively) (Table 2).
Relationship Between Ramp Lesion and Pre- and Postoperative Instability, and the Effect of Ramp Lesion Repair a
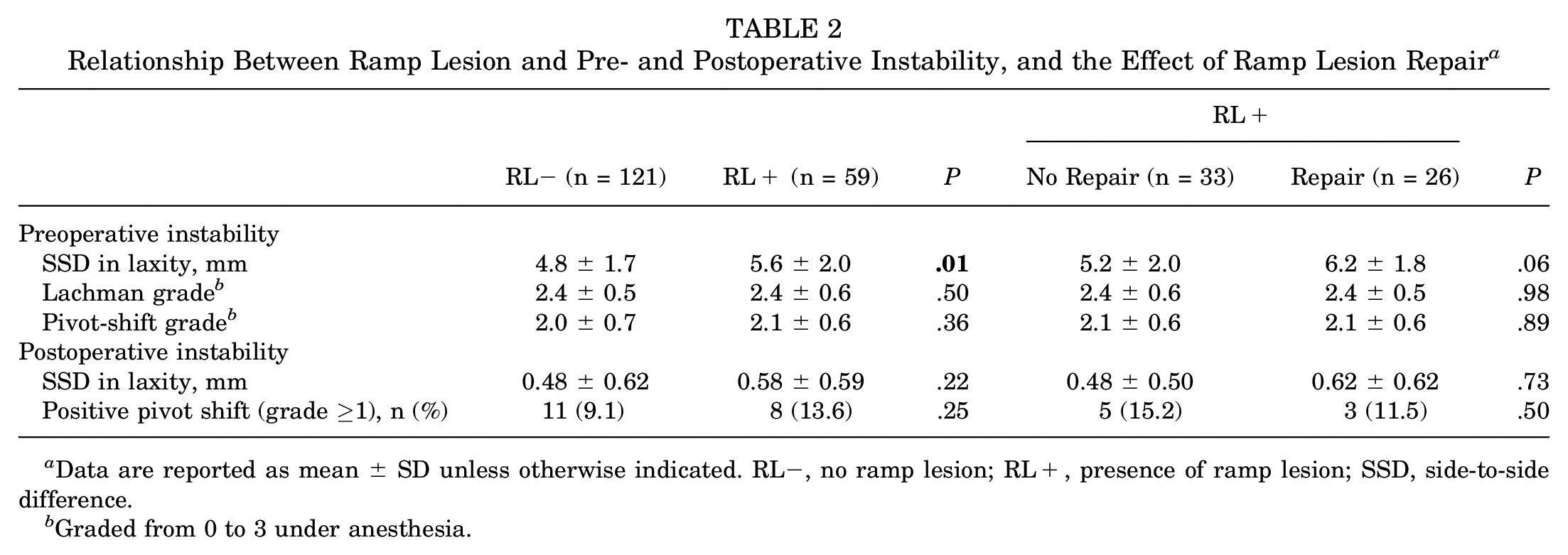
Data are reported as mean ± SD unless otherwise indicated. RL−, no ramp lesion; RL+, presence of ramp lesion; SSD, side-to-side difference.
Graded from 0 to 3 under anesthesia.
Logistic and linear regression analyses showed no association between the presence of RL and postoperative knee instability in any of the collected data (Table 3). The regression models within the RL+ group also found no association between undergoing surgical repair for RL and postoperative knee instability (Table 4).
Association Between Presence of Ramp Lesions and Postoperative Knee Instability a

Linear regression analysis was performed with 1-year postoperative SSD as the dependent variable, and logistic regression analysis was performed with 1-year postoperative pivot-shift grade ≥1 as the dependent variable. OR, odds ratio; SSD, side-to-side difference.
Defined as grade ≥1.
Association Between Ramp Lesion Repair and Postoperative Knee Instability in Patients With Ramp Lesion a

Linear regression analysis was performed with 1-year postoperative SSD as the dependent variable, and logistic regression analysis was performed with 1-year postoperative pivot-shift grade ≥1 as the dependent variable. OR, odds ratio; SSD, side-to-side difference.
Defined as grade ≥1.
Discussion
This study showed a correlation between the presence of RLs and preoperative SSD in laxity. However, RLs did not correlate with preoperative knee instability, including the Lachman and pivot-shift tests, as well as postoperative knee instability. Patients who underwent repair of a large, unstable RL did not show any difference in postoperative stability compared with patients who had a conservatively treated, small, stable RL. Notably, no secondary meniscal lesions requiring surgery occurred during the minimum 2-year postoperative follow-up period, whether or not the RLs were repaired. These results suggest the importance of stable anatomic ACL reconstruction, as RLs may be capable of natural healing.4,10,32
Although the frequency of RL associated with ACL injury has been reported,6,26 recent studies suggest a relatively high incidence.9,27 RLs were found in one-third of our patients, comparable with the findings of recent studies. The use of the posteromedial portal for systematic observation has not been consistent. 27 However, adequate evaluation was achieved through a step-by-step arthroscopic diagnosis. 30 Systematic reviews and previous studies have suggested that RLs are more prevalent in men, those <30 years, individuals with concomitant lateral meniscal tears, and those with contact injuries.19,23,26 In this study, RLs were more common in women than in men (P = .04). This might be due to the exclusion of ACL reconstructions using bone–patellar tendon–bone grafts. Since the graft type affects postoperative stability, ACL reconstructions using grafts other than hamstring tendon were excluded in this study. While we speculate that joint laxity in women may be a potential factor, the exact cause remains unelucidated.
The medial meniscus is a secondary restraint against anterior tibial translation. 8 Biomechanical cadaveric studies demonstrated that RL, in conjunction with ACL injury, amplified anterior tibial translation and tibial rotation and that repair of RL decreased these instabilities.2,11,20,28 Furthermore, longer RLs were correlated with increased anterior tibial and rotational instabilities. 21 Clinical studies have also shown that patients with ACL injuries combined with RL often exhibit a high-grade pivot shift compared with those with isolated ACL injuries.24,30 Thaunat et al 30 found that complete RLs (types 1, 4, and 5) correlated with a greater pivot shift and higher SSD. Also in the current study, the RL+ group had a greater preoperative SSD in laxity than the RL− group (P = .01). However, this difference was not significant after ACL reconstruction, since the effect of the RL was not as great as that of the ACL injury. Additionally, the patients who underwent surgical repair, potentially having larger RL, tended to show greater SSD compared with the nonrepair group (P = .06). Regarding the pivot-shift test, no significant difference was observed between the RL− and RL+ groups, contrary to our hypothesis. Hatayama et al 15 reported that anterior knee laxity in the RL-healed group was significantly lower than that in the RL-unhealed group. Although similar results were found, the difference was not statistically significant (P = .05).
The natural course of the untreated RL during ACL reconstruction remains unclear. Some authors have left stable RLs untreated, showing that conservative treatment does not negatively affect clinical and functional outcomes.4,7,22 In our series, untreated stable RLs also did not result in secondary damage, nor did it affect the clinical outcomes. Given the stability and relatively small size of RLs in the nonrepair group, spontaneous healing was presumably facilitated. Admittedly, the reliability of this healing rate is questionable because of the MRI’s limited diagnostic accuracy for RL.14,16,27 However, previous studies and ours suggest that stable RLs have the potential to heal spontaneously, and surgeons may not necessarily need to treat stable lesions.4,7,22 In a long-term study, Tuphé et al 31 found that nearly one-third of patients developed meniscal complications, primarily occurring 8 years after ACL reconstruction. Therefore, our minimum 2-year follow-up period may not adequately capture the natural course of RLs. However, it is important to perform early anatomic ACL reconstruction after injury before the meniscal conditions deteriorate. 17
MRI is the standard imaging modality for intra-articular lesions, such as ACL and meniscal injuries. However, meta-analyses and systematic reviews have shown that the sensitivity and specificity for detecting RL are not as high as expected. 18 Therefore, diagnostic arthroscopy has been considered the gold standard for RL diagnosis.27,30 The accuracy of MRI for the preoperative diagnosis of RL was not examined because this was a retrospective study, and the surgeon might have known the results of the arthroscopy. However, because the only way to confirm postoperative RL healing is through a second-look arthroscopy or MRI, a previous study has used MRI to determine the healing of RL. 22
Limitations
This study has a few limitations. First, the sample size was small, making it difficult to evaluate treatments using a detailed classification of RL. 30 In this retrospective study, stable RLs were left untreated, and all unstable RLs were repaired without the inclusion of prospective randomized controlled trials. Furthermore, various repair techniques were not compared. Although second-look arthroscopy is the optimal method for confirming meniscal healing, MRI was used to evaluate RL healing. While the natural course of unstable RLs is interesting, leaving it untreated is clinically difficult. Another limitation lies in the absence of long-term observation to determine the natural history and healing rate of RL. 31 To address these limitations, randomized studies with larger sample sizes should be conducted.
Conclusion
Although the presence of RLs was associated with preoperative SSD, contrary to our hypothesis, RLs were not associated with postoperative knee instability. Stable RLs are clinically benign lesions that may tend to heal spontaneously following appropriate anatomic ACL reconstruction. Therefore, RLs may not require aggressive treatment if they are small and stable.
Footnotes
Final revision submitted July 8, 2024; accepted July 23, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hirosaki University (ref No. 2023-077).