
Abstract
Background:
Biomechanical studies have shown that the transosseous equivalent suture bridge (TOE-SB) rotator cuff repair technique improves contact areas and pressure between the tendon and footprint, which may facilitate healing. However, few studies have directly compared its outcomes with traditional double-row (DR) repair.
Purpose/Hypothesis:
The primary objectives of this study were to (1) compare the functional outcomes of DR with TOE-SB fixation in patients undergoing arthroscopic rotator cuff repairs and (2) compare healing rates between the 2 groups and investigate whether any factors were associated with healing. It was hypothesized that arthroscopic rotator cuff repair using DR repair would demonstrate no difference in disease-specific quality of life, patient-reported outcomes, or healing rates compared with TOE-SB repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a cohort study conducted as a subanalysis of 2 larger randomized controlled trials. Patients ≥18 years old with degenerative rotator cuff tears confirmed by magnetic resonance imaging who had persistent symptoms of pain and functional impairment after 6 months of nonoperative management were enrolled in prospective randomized controlled trials and underwent either a traditional DR repair or a TOE-SB rotator cuff repair. Functional outcomes were assessed using the Western Ontario Rotator Cuff index, the American Shoulder and Elbow Surgeons score, and the Constant score at baseline and 3, 6, 12, and 24 months postoperatively. Healing rates were determined using ultrasound at 24 months postoperatively.
Results:
A total of 184 patients were included in this study; 34 patients underwent conventional DR repair and 150 underwent TOE-SB repair. Postoperative changes in the outcome measures from baseline were statistically significant for all outcomes in both groups (P < .0001). No statistically significant differences were found between outcomes at any of the follow-up times, except a significant difference in the Constant score at 24 months in favor of the DR group (mean ± SE, 80.5 ± 1.1 [95% CI, 78.4-82.7]) and TOE-SB and DR, respectively (mean ± SE, 85.7 ± 2.2 [95% CI, 81.2-90.1]) (P = .041). Healing rates were 77.8% for DR and 83% for TOE-SB (odds ratio, 1.34 [95% CI, 0.53-3.38]; P = .53). Multivariable regression analysis showed a positive correlation between nonhealing rates and the rotator cuff tear size in the sagittal plane (odds ratio, 1.97 (95% CI, 1.02-3.78); P = .042).
Conclusion:
No difference was found between DR and TOE-SB rotator cuff repair in the Western Ontario Rotator Cuff index, the American Shoulder and Elbow Surgeons score, Constant strength subscore, or the healing rate. The Constant score at the 24-month follow-up favored DR repair but did not reach the minimal clinically important difference. An association was found between higher healing rates and smaller sagittal plane tear sizes.
Rotator cuff tears are a common clinical entity, with tears present in <25% of patients <50 years old, and <50% of those <80 years old.35,39 While some tears remain asymptomatic, rotator cuff pathology is a common source of shoulder complaints and accounts for a considerable economic burden.21,25,27,34,38 For those who have failed nonoperative management, rotator cuff repair has been shown to be associated with improvement in pain, function, and quality of life.2,18,21,30 While repair may be performed through open, mini-open, and arthroscopic means, arthroscopic repair has become the predominant form.11,40 The trend toward increasing the use of arthroscopic rotator cuff repair is in part due to innovation in arthroscopic surgical techniques and instrumentation. 36 In the evolution of rotator cuff surgery, multiple repair configurations have been described—including single-row (SR), double-row (DR), and a transosseous equivalent suture bridge (TOE-SB).
Original arthroscopic repair descriptions consisted of SR repair, where the rotator cuff tendons were fixed to an SR of suture anchors along the lateral aspect of their bony insertion. 1 Lo and Burkhart 20 designed the DR repair in 2003 as a means to better approximate the medial to the lateral width of the rotator cuff footprint, thereby increasing the area of the tendon-bone contact area of the repair in hopes of improving healing. Their modification consisted of a medial row of anchors placed along the lateral aspect of the articular margin of the humeral head and a second lateral row of anchors placed along the lateral aspect of the bony bed, just medial to the drop off of the greater tuberosity of the humerus. The tendon repair is secured to the medial row of anchors by mattress sutures tied over a tendon bridge, while the lateral aspect of the tendon repair is performed through independent sutures drawn from the lateral row of anchors. 20
The DR repair was further modified by Park et al 28 in 2006 by building on the concepts of transosseous tunnel repair performed in open rotator cuff surgery. In their technique, a medial row of anchors is placed along the lateral articular margin, and suture strands are passed through the rotator cuff tendon 10 to 12 mm medial to the lateral edge of the tendon stump. It differs from the traditional DR in that the suture limbs from the medial row are then used to create a suture bridge over the remaining rotator cuff tendon that is anchored to bone through the lateral row anchors placed 1 cm off the distal-lateral aspect of the greater tuberosity. 28 Biomechanical analysis has shown this to result in greater contact pressures under cyclic loading; however, there is a paucity of clinical research comparing the 2 techniques. 22
The purpose of this multicenter retrospective cohort study was to compare the functional outcomes and healing rates of DR versus TOE-SB fixation in patients undergoing arthroscopic rotator cuff repair, as well as to investigate whether any factors were associated with healing. We hypothesized that arthroscopic rotator cuff repair using DR fixation would demonstrate no difference in disease-specific quality of life, patient-reported outcomes, or healing rates when compared with TOE-SB repair.
Methods
Study Design
This was a subanalysis of 2 previous randomized controlled trials (RCTs) conducted at 3 academic-level hospitals in Canada: The Ottawa Hospital in Ottawa, Ontario; The Pan Am Clinic in Winnipeg, Manitoba; and The Glen Sather Sports Medicine Clinic in Edmonton, Alberta. Our sample population was taken from treatment arms of 2 different RCTs completed at these institutions.17,18 Enrollment occurred between 2007 and 2009, and 2013 and 2018, respectively, with follow-ups having been completed by 2012 and 2020 for each enrollment group, respectively. Patient follow-up was conducted at 3, 6, 12, and 24 months.
The cohort undergoing DR repair was derived from an RCT completed in 2012 in which patients were allocated to undergo either SR or DR repair. 18 All patients who have been included in the present study were drawn from the DR repair arm. Patients undergoing TOE-SB repair were derived from the second study completed in 2020. These patients were randomized at the time of the surgery to undergo either intraoperative bone channeling or standard repair without channeling. 17 Both original studies employed similar inclusion and exclusion criteria, patient populations, surgical teams, and study methods, making direct comparisons between groups valid and practical. Institutional review board approval was granted for both source studies.
Inclusion Criteria
The inclusion criteria were as follows: (1) age ≥18 years; (2) degenerative rotator cuff tears confirmed by magnetic resonance imaging (MRI) and intraoperative findings confirming a full-thickness rotator cuff tear; (3) ability to understand and adhere to rehabilitation protocols and testing procedures; and (4) persistent pain and functional disability for at least 6 months with failure of 6 months of conservative treatment.
Exclusion Criteria
The exclusion criteria were as follows: (1) characteristics of the cuff tear that rendered the cuff irreparable: rotator cuff muscle fatty infiltration of Goutallier grade ≥3 (involving 50% of the cross sectional area),6,7 superior subluxation of the humeral head, retraction of the cuff to the level of the glenoid rim12,16; (2) partial-thickness cuff tears; (3) traumatic tears (based on patient history); (4) significant shoulder comorbidities (eg, Bankart lesion, osteoarthritis, rotator cuff arthropathy, or Charcot arthropathy); (5) previous surgery on the affected shoulder (eg, previous rotator cuff repair); (6) active joint or systemic infection; (7) significant medical comorbidity that could alter the effectiveness of the surgical intervention (eg, cervical radiculopathy, polymyalgia rheumatica); (8) major medical illness (life expectancy <1 year or unacceptably high operative risk); (9) inability to speak or read English or French; (10) psychiatric illness that precludes informed consent; and (11) unwilling to be observed for 24 months.
Surgical Technique
All surgeries were performed by fellowship-trained shoulder surgeons (P.L., J.W.P., P.M., M.B.) with patients in either the beach-chair position or the lateral position under either general anesthesia or regional nerve block. In both techniques, the medial row of anchors was placed at the bone-cartilage junction at the medial aspect of the rotator cuff footprint. The torn tendon was repaired to the bone using mattress sutures with sliding locking knots, followed by alternating half hitches. Biceps pathology (tears, subluxation) was managed with a biceps tenodesis in both groups.
In the DR group, the lateral row of anchors was placed along the lateral aspect of the tendon footprint, and mattress or inverted mattress sutures were used to repair the tendon to bone. Sutures from the medial row of anchors were not tied or linked to the sutures of the lateral row of anchors (Figure 1). The repair was performed using either Super Revo (CONMED Linvatec) or poly-l-lactic acid Duet anchors, loaded with Hi-Fi suture (CONMED Linvatec).
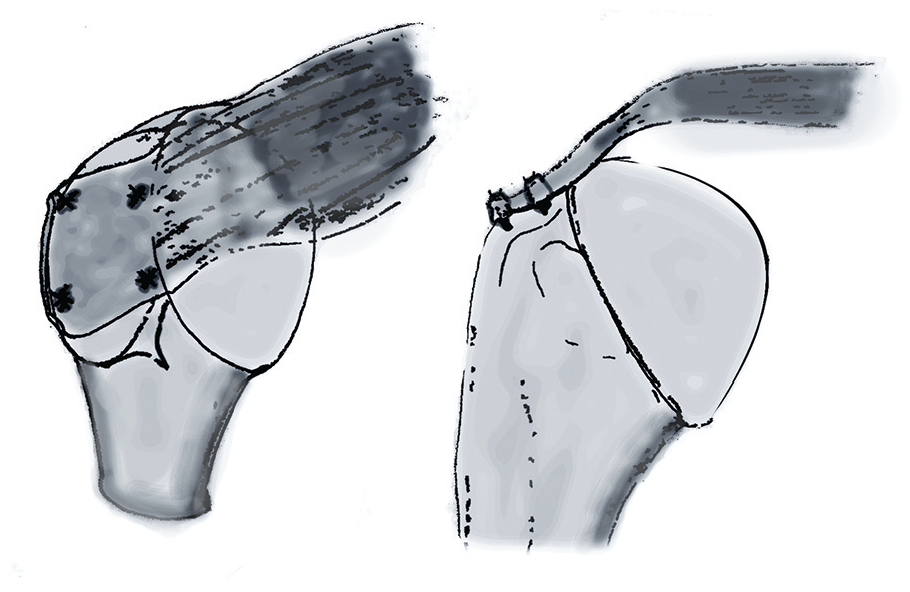
Double-row fixation suture pattern.
In the TOE-SB group, the suture strands of the medial row were then loaded into the lateral row anchor, which was secured within the bone with the sutures under tension just distal to the greater tuberosity (Figure 2). Medial row fixation was performed with polyetheretherketone vented 4.5 mm CrossFT (CONMED Linvatec) or nonvented 5 mm TwinFix (Smith+Nephew) double loaded with high-tensile strength suture (HiFi; CONMED Linvatec). Lateral row fixation was performed with knotless 4.5 mm PopLock anchors (CONMED Linvatec).

Suture bridge fixation suture pattern.
The number of suture anchors used was determined at the surgeon’s discretion and was based on the size and complexity of the tear. All patients were discharged on the same day as their surgery.
Rehabilitation
Pendulum exercises were initiated on the first postoperative day. Patients were advised to maintain sling use until 6 weeks postoperatively, at which time supervised physical therapy was initiated with active-assisted range of motion exercises. Active motion began between 8 and 12 weeks postoperatively and strengthening and reintegration into normal routine began at 12 weeks postoperatively. Surgical techniques and postoperative rehabilitation plans were standardized across centers. The supervised physical therapy program was continued for 4 to 6 months postoperatively.
Outcomes Measures and Assessment
The primary outcome of the study was the disease-specific quality of life, as measured by the Western Ontario Rotator Cuff (WORC) index, 14 which is a validated and highly responsive disease-specific measure for disorders of the rotator cuff. 33 Secondary patient-reported outcome measures included the Constant Score 4 and the American Shoulder and Elbow Surgeons (ASES) standardized assessment of shoulder function. 32 All 3 scores range from 0 to 100 points, with 100 points representing a perfect score. Each score was documented at baseline and 3, 6, 12, and 24 months postoperatively. Patients were assessed by 2 research coordinators (K.M. and S.A.) who were blinded to group randomization in outpatient orthopaedic clinics.
The rotator cuff tear size at baseline was determined by preoperative MRI measurements. The retear rate was measured at 24 months postoperatively by ultrasound, which has been shown to be highly accurate at detecting full-thickness rotator cuff tears in the postoperative setting. 29 A blinded fellowship-trained musculoskeletal radiologist (T.H.) determined the retear. The repair was considered healed if the ultrasound showed that tendons were in continuity with no evidence of full-thickness tearing. The thickness of the supraspinatus tendon at 10 mm from the lateral edge of the tendon footprint at the final follow-up was also measured as an indication of tendon integrity.
Statistical Analysis
Baseline characteristics were reported for the 2 groups using the mean and standard deviation or the median and interquartile range for continuous and count variables and frequency and proportion for categorical variables. Statistical comparisons were conducted to compare these characteristics between the 2 groups by conducting a t test or the Wilcoxon signed-rank test for comparing means and medians or by performing a chi-square test or the Fisher exact test for categories, and P values for 2-sided tests were reported. Repeated-measures linear regression analysis was conducted to model ASES, WORC, Constant strength, and Constant total, and comparisons were performed between the 2 groups at each time point and within groups over time, after adjusting for covariates of age and coronal and sagittal tear size. The least-squares mean and standard error, along with 95% CIs, were reported for outcomes in each group at different time points.
Results
Participants
A total of 184 patients from the 2 previous RCTs were included in the study. A total of 42 patients were allocated to DR repair and 8 patients were lost to follow-up by the 24-month follow-up interval, yielding 34 patients for analysis (Figure 3). Regarding the patients who underwent TOE-SB repair, of 168 patients allocated to TOE-SB repair, 9 patients were lost to follow-up by the 24-month mark in each of the trephination and no trephination groups. This totaled 18 patients who did not complete the follow-up, leaving 150 patients who completed the study. Overall, 34 patients in the DR group and 150 in the TOE-SB group were included in the final analysis for the primary outcome measure.

Flowchart of patient inclusion criteria.
Baseline descriptive data are summarized in Table 1. Groups were well balanced with respect to age, sex, affected shoulder, and sagittal tear size. Differences between groups reached statistical significance for coronal tear size (DR mean tear size 2.6 cm ± 1.2 cm vs TOE-SB mean tear size 2 cm ± 0.9 cm; P = .009). The mean number of anchors was not significantly different between the 2 groups (2.7 ± 1.2 and 2.8 ± 1.2 in the DR and TOE-SB groups, respectively; P = .6067).
Baseline Demographic Data of Patients a

Data are presented as mean (SD) and n (%). DR, double-row; TOE-SB, transosseous equivalent suture bridge.
The bold P value indicates significance.
Patient-Reported Outcomes
Baseline ASES scores were worse in the TOE-SB group. Both DR and TOE-SB repair groups demonstrated statistically significant improvements in all outcomes scores from baseline to 24 months (Table 2, Figures 4–6). No difference was detected between groups in the primary outcome measure (WORC) at any time point.
Comparison of Between Group Outcome Scores by Time Point a

ASES, American Shoulder and Elbow Surgeons; DR, double-row; TOE-SB, transosseous equivalent suture bridge; WORC, Western Ontario Rotator Cuff.
The bold P values indicate significance.

WORC progression over time. DR, double-row; TOE-SB, transosseous equivalent suture bridge; WORC, Western Ontario Rotator Cuff Index.
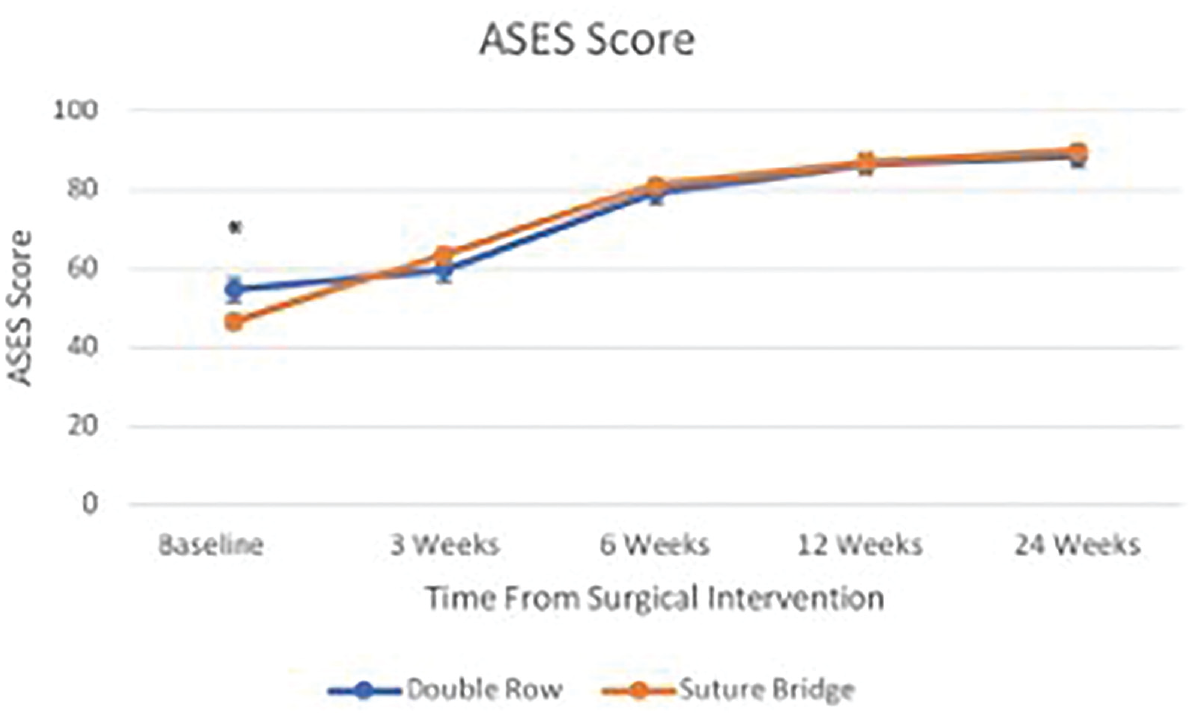
ASES score progression over time. ASES, American Shoulder and Elbow Surgeons; DR, double-row; TOE-SB, transosseous equivalent suture bridge. The asterisk denotes statistical significance.

Constant Score (total) progression over time. DR, double-row; TOE-SB, transosseous equivalent suture bridge. The asterisk denotes statistical significance.
At the 24-month follow-up, the total Constant score was significantly higher in the DR group (85.7 ± 2.2 [95 % CI, 81.2-90.1]) compared with the TOE-SB group (80.5 ± 1.1 [95% CI, 78.4-82.7]) (P = .04). No significant differences between the DR and TOE-SB groups were found for the remaining patient outcome measures at any time point (Table 2).
Healing Rates
At the 24-month follow-up, an ultrasound was obtained to evaluate the integrity of the rotator cuff repair in 150 patients (81%)—including 346 (100%) in the DR repair group and 114 (76%) in the TOE-SB group. The overall healing rate was 81.3%. The healing rate was 78% in patients who underwent DR repair and 83% in those who received TOE-SB repair. This difference was not statistically significant (odds ratio [OR], 1.34 [95% CI, 0.53-3.38]; P = .53).
Multiple Variable Logistic Regression Analysis
Multiple variable logistic regression analysis was performed to assess the effect of known prognostic variables—such as randomization group, age, sex, number of anchors, and tear size—in both coronal and sagittal planes with retear rates as the dependent variable (Table 3). A strong positive correlation was found between nonhealing rates and the rotator cuff tear size in the sagittal plane (OR, 1.97 (95% CI, 1.02-3.78); P = .042). No other significant correlation was found.
Multivariable Regression Analysis a
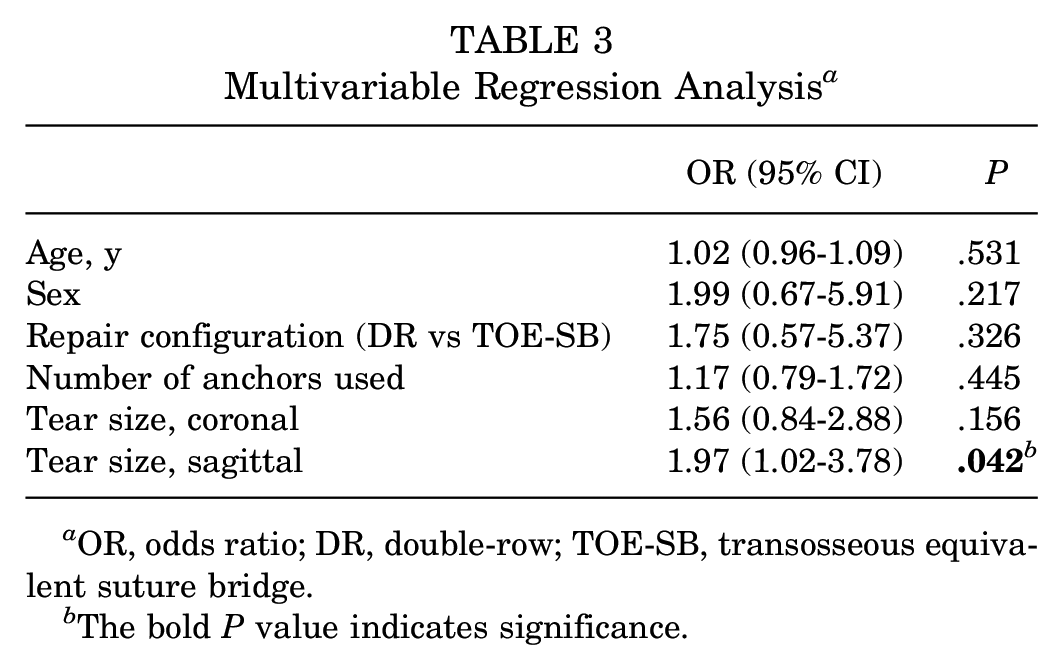
OR, odds ratio; DR, double-row; TOE-SB, transosseous equivalent suture bridge.
The bold P value indicates significance.
Discussion
No difference at follow-up was found between the DR and TOE-SB repair groups in the WORC score, ASES, or Constant strength subscore. A statistically significant difference in the final total Constant score was found at the final follow-up. This difference did not reach the minimal clinically important difference of 10.1 for rotator cuff tears. 15 Furthermore, no difference in healing rate was detected between groups. Multivariable linear regression analysis demonstrated a positive correlation between healing and the tear size in the sagittal plane but no differences with age, sex, repair configuration, number of anchors used, or tear size in the coronal plane.
There is conflicting evidence in the existing literature comparing independent DR and TOE-SB rotator cuff repairs. The results of the present study are in keeping with the findings of Kim et al 13 and Lee et al 19 with respect to ASES scores. The independent DR group showed a significantly higher Constant score at the 24-month follow-up, which is in contrast with the findings of Chen et al, 3 Lee et al, 19 Kim et al, 13 Hashiguchi et al, 8 and McCormick et al. 23 The present study was in agreement with most of the published comparative literature in finding no difference in healing rates between techniques.10,19,23 There are 2 published exceptions to this finding, which both found lower retear rates with TOE-SB repair.8,24
Aggregated results of DR repair and TOE-SB repair published in systematic reviews and meta-analyses depend on the outcome measured and the inclusion and exclusion criteria of the analysis. Four systematic reviews and meta-analyses have previously compared clinical outcomes after DR and TOE-SB rotator cuff repairs.5,9,31,37 Hein et al 9 published a systematic review in 2015 as a follow-up to the study published by Duquin et al 5 in 2010, comparing healing rates between SR, DR, and TOE-SB rotator cuff repair. Their study included 648 patients who underwent a DR repair and 705 patients who underwent a TOE-SB repair. Of note, their systematic review and meta-analysis were not restricted to comparative studies and only 2 of the included studies directly compared DR and TOE-SB techniques. They found no difference in retear rates between DR and TOE-SB repairs in tears <1 cm (4% vs 0%; P = .929), tear sizes 1 to 3 cm (10% vs 12%; P = .562), or tear sizes >3 cm (34% vs 31%; P = .556).
Ren et al 31 published a systematic review and meta-analysis of 7 studies comparing DR and TOE-SB repair. Their study consisted of 1 randomized control trial, 3 retrospective studies, and 3 comparative cohort studies comprising 295 patients treated with DR repair and 290 patients treated with the TOE-SB technique. No differences were reported between techniques as measured by the Constant, ASES, and visual analog scale for pain scores, whereas the University of California Los Angeles shoulder score favored TOE-SB repair. They found that the retear rate favored DR repair with an OR of 0.31. This is in contrast with the findings of the present study in which no differences were detected between groups.
Finally, Xu et al 37 performed a network systematic review and meta-analysis of arthroscopic rotator cuff repair techniques—including papers comparing SR, DR, and TOE-SB repairs. They included 21 studies with a total of 1815 shoulders in their analysis. They did not detect a difference in Constant scores between SR, DR, or TOE-SB repair in pairwise or network analysis. While both DR and TOE-SB repairs outperformed SR repairs, no difference was detected in the retear rate between the DR and TOE-SB repairs.
Given that the 2 surgical approaches yielded similar clinical effectiveness, either technique appears to be acceptable. Factors to be considered in deciding on which approach to use include ease of technique, time, and cost. We generally considered the TOE-SB technique faster and simpler given that less suture passing was required in this technique. The relative cost of lateral row anchors is another important factor and will vary by manufacturer.
Our findings in the multivariable linear regression model are partly in keeping with those of Kwon et al 16 in their work in creating the Rotator Cuff Healing Index. They performed a univariate and multivariate analysis of previously known or suggested factors affecting cuff integrity after surgical repair. A numerical scoring system was created using clinical and radiographic factors that demonstrated a positive correlation with retear. Their scoring system included the sagittal tear width, which was consistent with the findings of the present study, as well as age, which was not found to have a significant contribution to nonhealing in the present study. Scored from 0 to 15, they showed the Rotator Cuff Healing Index to have a high specificity and positive predictive value for retear prediction.
Strengths and Limitations
The present study is technically retrospective because the study question was formulated after the outcome data were collected; however, the study derives its data from 2 randomized control trials. This unique feature confers several advantages that are considered strengths of the study. The data were prospectively collected; the practices of a high-level RCT were followed in the collection of study data—including blinding of patients and assessors to ensure minimization of detection bias and the use of standardized surgical techniques and rehabilitation protocols to limit performance bias. 26
This study has certain limitations. The retrospective design may be associated with selection bias. However, we only included patients enrolled in prospective randomized trials with strict inclusion and exclusion criteria, which should greatly reduce this possibility. Another limitation of the study is the loss to follow-up rate that occurred in measuring retears. Also, 19% of the patients included in the study did not undergo follow-up imaging at the 24-month mark. No difference was detected between groups in retear rate; however, the strength of this finding is limited by the absence of results in these patients. While treatment groups were relatively well balanced, there was noted heterogeneity between groups with respect to tear characteristics. The mean coronal plane tear size in the DR group was greater than that of the TOE-SB group (2.6 ± 1.2 cm vs 2 ± 0.9 cm, respectively; P = .0097). However, this factor was controlled for in the analysis. A further limitation of the study is the difference in time over which enrollment and treatment took place between the 2 groups. The patients who underwent a DR repair were enrolled between 2007 and 2009, in contrast with the TOE-SB group, who were enrolled between 2013 and 2018. This gap in time allows for further experience and refinement of the treating surgeons’ surgical technique that may confound outcomes between the 2 techniques alone. However, all surgeons involved in the study were fellowship-trained shoulder surgeons and had many years of experience in arthroscopic cuff repair techniques before the first clinical trial. Finally, half of the patients treated with a TOE-SB repair underwent bone channeling at the time of the repair, whereas the DR repair group did not undergo this adjunctive procedure. The addition of an adjunctive procedure in only 1 group leaves open the possibility of a potentially confounding effect. 17 However, the trial did not show any differences between the channeling and no-channeling groups in ASES, WORC, Constant scores, or healing rates at the 2-year follow-up. 17
Conclusion
No difference was detected between the DR and TOE-SB rotator cuff repair groups in the WORC, ASES, Constant strength subscore, or healing rates. The statistically significant difference in the Constant score favoring DR repair may warrant further study. Finally, an association was found between higher healing rates and smaller sagittal plane tear sizes.
Footnotes
Final revision submitted July 22, 2024; accepted July 29, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.L. is a paid consultant and performs educational talks with Stryker (previously Wright Medical), related to shoulder arthroplasty work. J.W.P. is a paid consultant and performs educational talks with Stryker and CONMED. P.M. is a paid consultant and performs educational talks with Stryker and CONMED. M.B. performs paid educational talks with Stryker and Smith+Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Ottawa Hospital (7966).