
Abstract
Background:
Previous research has reported higher rates of both injury and illness among Paralympic athletes compared with Olympic athletes during the Winter Olympic and Paralympic Games, but no studies have directly compared injury and illness incidence between Olympic and Paralympic athletes competing in a Summer Games.
Purpose:
To compare injury and illness rates between Olympic and Paralympic Team USA athletes competing in the Tokyo 2020 Olympic and Paralympic Games.
Study Design:
Descriptive epidemiology study.
Methods:
All injuries and illnesses that occurred among the Team USA athletes competing in the Tokyo 2020 Summer Olympic or Paralympic Games were documented. A total of 701 Team USA athletes (53.6% female) competed in the Tokyo 2020 Summer Olympic Games, across 34 different sports. For the Tokyo 2020 Summer Paralympic Games, a total of 245 athletes (51.6% female) competed across 20 sports. Incidence rates (IRs) per 1000 athlete-days were calculated according to sex, sport, anatomic location, and illness type. IR ratios (IRRs) were calculated to compare IRs between male and female athletes and between Olympic and Paralympic athletes.
Results:
Overall, there were no differences in injury incidence (IRR, 1.18; 95% CI, 0.84-1.68) or illness incidence (IRR, 0.68; 95% CI, 0.41-1.15) between Olympic and Paralympic athletes. Male Paralympic athletes were less likely to sustain an illness compared with female Paralympic athletes (IRR, 0.35; 95% CI, 0.11-0.90).
Conclusion:
There were no differences in injury or illness rates between Olympic and Paralympic Team USA athletes competing at the Tokyo 2020 Summer Games, contrary to previous comparisons among winter sport athletes. These results challenge the prevailing notion that Summer Paralympic athletes are at greater injury and illness risk, suggesting that factors beyond Olympic or Paralympic Games participation influence health concerns.
Multinational epidemiological data from both Summer and Winter Olympic and Paralympic Games have helped characterize common injuries and illnesses across sports during this unique competitive setting.7,9,18-21 Through these efforts, the risk of injuries and illness occurring during the Games periods has become better quantified, which allows for the development and implementation of effective injury and illness prevention strategies and resource planning.10,18,20-22 While there is an improved understanding of the overall (global) injury and illness risk during both the Summer and the Winter Olympic and Paralympic Games, identifying these risks among a single country's delegations is vital to consider, as there are a variety of factors that may differ among countries and predispose their athletes to unique patterns of injury and illness. While some single-country epidemiological data exist for both Olympic and Paralympic Games, these reports have either profiled countries that field relatively small delegations3,4,11,12,23 or have focused only on Olympic and Paralympic athletes competing in Winter Games.2,14 Single-nation data from larger and more diverse delegations, such as Team USA, are severely lacking. These types of data may reveal differences in injury and illness risks that can potentially be generalized to other athlete delegations of similar size and resources.
Despite the widespread reporting of multinational epidemiological data from both Olympic and Paralympic Games, and some limited reports of single-delegation data, there is little understanding of the differences in injury and illness burden during a Games period between Olympic and Paralympic athletes. While it is largely assumed that Paralympic athletes have an increased risk of injury and illness compared with Olympic athletes secondary to their impairments or associated medical conditions, this assumption has been based on comparisons of separately published Olympic and Paralympic Games data.5,8-10,17-21,25 For example, multinational data from prior Summer Paralympic Games (SPG) have reported rates ranging between 5.8 to 10.0 injuries5,8,25 and 4.2 to 13.2 illnesses5,9,17 per 1000 athlete-days. These rates range from being equivalent to rates reported during Olympic Games to being approximately twice or 3 times as high as Olympic rates.10,18,21 To date, there has only been 1 study 2 that has directly compared injury and illness rates between Olympic and Paralympic athletes during a Games period (the Beijing 2022 Winter Games); these authors reported rates among Paralympic Team USA athletes (29.1 injuries and 16.5 illnesses per 1000 athlete-days) compared with Olympic Team USA athletes (16.5 injuries and 6.8 illnesses per 1000 athlete-days). However, there is no research directly comparing injury and illness rates between Olympic and Paralympic athletes during a Summer Games.
The purpose of this study was to describe the incidence of injuries and illnesses sustained by Team USA athletes during the Tokyo 2020 Summer Olympic and Paralympic Games and to directly compare injury and illness rates between Olympic and Paralympic Team USA athletes. We hypothesized that Paralympic Team USA athletes would demonstrate higher rates of both injury and illness compared with Olympic Team USA athletes.
Methods
This retrospective descriptive study assessed the findings of the US Olympic & Paralympic Committee's injury and illness surveillance program during the Tokyo 2020 Summer Olympic Games (SOG) and the Tokyo 2020 SPG. To capture the entire range of time that Team USA athletes were in Tokyo for training/practice/competition and therefore at-risk for sustaining an injury or illness, the precompetition, competition, and postcompetition periods were combined and analyzed for both the SOG and the SPG. The 30-day SOG period consisted of an 11-day precompetition period, 16-day competition period, and 3-day postcompetition period (July 13-August 11, 2021). The 26-day SPG period consisted of an 11-day precompetition period, 12-day competition period, and a 3-day postcompetition period (August 13-September 8, 2021). The study protocol received institutional review board approval.
Data Collection
Medical providers delivering care to Team USA athletes during the Tokyo 2020 SOG and SPG documented all medical encounters into an electronic medical record (GE Centricity; General Electric). Medical encounters were defined as medical services (ie, consultation/evaluation, treatment, and preventive/recovery services) provided by Team USA–credentialed health care providers across all clinics. Medical providers (SOG, n = 148; SPG, n = 39) consisted of physicians (SOG, n = 37; SPG, n = 6), athletic trainers (SOG, n = 46; SPG, n = 12), physical therapists (SOG, n = 18; SPG, n = 9), chiropractors (SOG, n = 15; SPG, n = 6), massage therapists (SOG, n = 14; SPG, n = 3), mental health providers (SOG, n = 11; SPG, n = 3), physician assistants (SOG, n = 3), veterinarians (SOG, n = 3), and equine physical therapists (SOG, n = 1). Following the completion of the Tokyo 2020 SOG and SPG, the research team conducted a quality control process whereby all documented medical encounters were individually reviewed by the research team to ensure accuracy of each respective record. All consultations/evaluations indicative of new injuries or illnesses or exacerbations of existing injuries or illnesses occurring during the above-mentioned Games period were extracted for analysis.
Definition of Injury and Illness
Definitions of injury and illness were derived according to the 2020 International Olympic Committee (IOC) Consensus Statement for recording and reporting sport epidemiological data. 13 The Orchard Sports Injury and Illness Classification System (OSIICS) 14 was used to classify all injuries and illnesses. Specifically, an injury was defined as “tissue damage or other derangement of normal physical function due to participation in sports, resulting from rapid or repetitive transfer of kinetic energy.” The onset of injury was classified as either “acute” or “gradual” onset. Acute onset was defined as an injury with a sudden onset during sport participation. Gradual onset was defined as an injury that did not have an identifiable precipitating event or was an exacerbation of a previous injury. The mechanism of acute onset was further classified as either “contact acute” or “noncontact acute.” Contact injuries were defined as either direct (“mechanisms directly leading to the health problem in an immediate and proximal manner”) or indirect (“mechanisms stemming from contact with other athletes or an object, but with the force not applied directly to the injured area”). Noncontact injuries were defined as “mechanisms that lead to health problems without any direct or indirect contact from another external source.” Finally, injuries were also classified by anatomic location (eg, head/face, neck, shoulder).
Illness was defined as “a complaint or disorder experienced by an athlete, not related to injury. Illnesses include health-related problems in physical (eg, influenza), mental (eg, depression) or social well-being, or removal or loss of vital elements (air, water, warmth).” Illnesses were further classified by the involved body system (eg, respiratory, dermatologic, etc). For the purposes of this study, medical diagnoses associated with the SARS-CoV-2 virus were not included in the analyses, due to <1% of Team USA athletes and staff being diagnosed with COVID-19 during either the Tokyo 2020 Summer Olympic or the Paralympic Games and to make these data more generalizable to other delegations and Games periods that occurred outside of the COVID-19 pandemic. 1 Mental health encounters were also not included within this analysis, for several reasons. These included the lack of specific diagnostic classifications within the OSIICS coding system for mental health conditions, 15 the lack of standardized methods to conduct surveillance of mental health conditions within athletes at the time of data collection (the mental health supplement to the IOC surveillance consensus statement was published in July 2023), 13 and the specific methods by which Team USA psychological service providers delivered mental health support for athletes.
Calculation of Athlete Exposure
Individual athlete exposure was calculated as the number of days an athlete was in Japan during the respective Games period. Flight manifest data detailing the date of arrival and date of departure from Tokyo were obtained from the US Olympic & Paralympic Committee for all Team USA athletes competing in the Tokyo 2020 SOG or SPG. The total number of days that each individual athlete remained in Japan was summed to determine the total number of athlete-days, both within the total athlete sample and within each subgroup of interest. This served as the measure of exposure for calculating injury and illness epidemiology data.
Statistical Analysis
Per regulations from the approving institution's institutional review board to maintain athlete confidentiality, for sports where <10 athletes competed for Team USA during either the SOG or the SPG in Tokyo 2020, sports were grouped based on relative similarities and are shown in the Results.
The number of athletes participating, total number of athlete-days, frequency of injuries and illnesses, sports represented, and athlete ages were all summarized using descriptive statistics. The incidence rate (IR) was calculated per 1000 athlete-days using the formula (total number of injuries or illnesses/total number of athlete-days) × 1000 for both injury and illness, as well as by sex, sport, anatomic location, and illness type. IR ratios (IRRs) were calculated to compare injury and illness rates between male and female athletes and between Olympic and Paralympic athletes. For comparisons between Olympic and Paralympic sports, a subset of analogous sports was chosen: athletics and para athletics, basketball and wheelchair basketball, cycling and para cycling, rugby and para rugby, swimming and para swimming, and volleyball and sitting volleyball. These analogous sports were chosen based on similarities in the underlying sport as well as having >10 participants due to the regulations of our institutional review board. Finally, injury and illness proportions (IPs) were calculated as (number of injuries or illnesses/number of athletes) × 100. The 95% CIs were calculated for IP, IR, and IRR values. All analyses were performed using R statistical software (Version 4.3.2, R Foundation for Statistical Computing 16 ), and all IRs, IRRs, and 95% CIs were calculated as described above using the epiR package. 24
Results
A total of 701 athletes (53.6% female) competed for Team USA across 34 sports at the Tokyo 2020 SOG. For the Tokyo 2020 SPG, a total of 245 athletes (51.6% female) competed across 20 sports. There were no differences in overall injury incidence (IRR, 1.20; 95% CI, 0.86-1.70) or illness incidence (IRR, 0.69; 95% CI, 0.42-1.17) between Olympic and Paralympic athletes.
Injury and Illness by Sex
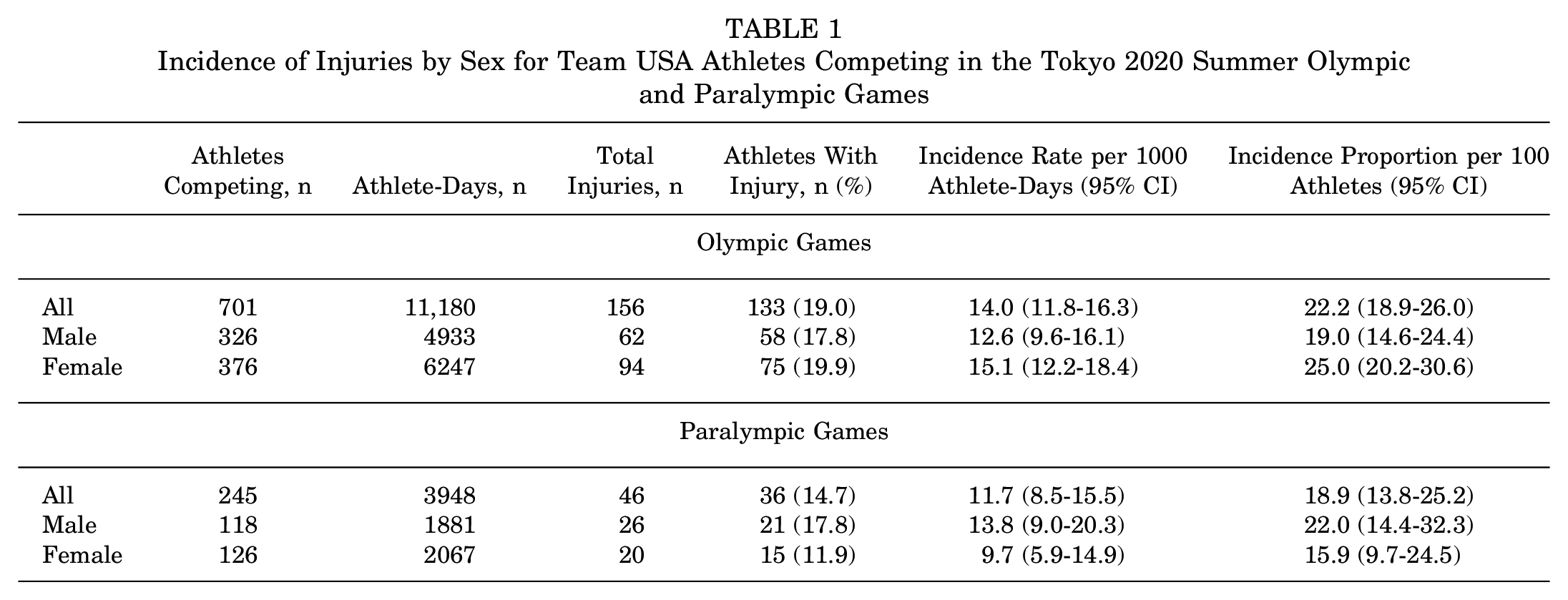
Incidence of injury or illness by sex for both Olympic and Paralympic athletes are presented in Tables 1 and 2, respectively. There were no differences in injury incidence between male and female Olympic athletes (IRR, 0.84; 95% CI, 0.60-1.16), between male and female Paralympic athletes (IRR, 1.43; 95% CI, 0.77-2.70), between male Olympic and Paralympic athletes (IRR, 0.91; 95% CI, 0.57-1.50), or between female Olympic and Paralympic athletes (IRR, 1.56; 95% CI, 0.95-2.66).
Incidence of Injuries by Sex for Team USA Athletes Competing in the Tokyo 2020 Summer Olympic and Paralympic Games
Incidence of Illness by Sex for Team USA Athletes Competing in the Tokyo 2020 Summer Olympic and Paralympic Games

Significant difference vs male Paralympic athletes.
Similarly, there were no differences in illness incidence between male and female Olympic athletes (IRR, 0.67; 95% CI, 0.35-1.25), between male Olympic and Paralympic athletes (IRR, 1.08; 95% CI, 0.41-3.35), or between female Olympic and Paralympic athletes (IRR, 0.56; 95% CI, 0.31-1.04). However, male Paralympic athletes were significantly less likely to sustain an illness compared with female Paralympic athletes (IRR, 0.35; 95% CI, 0.11-0.90).
Injury and Illness by Sport
The incidence of injury and illness by sport for both Olympic and Paralympic athletes is presented in Appendix Tables A1 to A4. The 3 Olympic sports with the highest incidence of injury were tennis (IR, 51.3 [95% CI, 18.8-111.6], per 1000 athlete-days), gymnastics (IR, 49.5 [95% CI, 30.7-75.7], per 1000 athlete-days), and rugby (IR, 42.0 [95% CI, 25.7-64.9], per 1000 athlete-days). The 3 Paralympic sports with the highest incidence of injury were goalball (IR, 30.7 [95% CI, 12.3-63.3], per 1000 athlete-days), wheelchair rugby (IR, 25.6 [95% CI, 7.0-65.7], per 1000 athlete-days), and cycling (IR, 24.6 [95% CI, 9.0-53.5], per 1000 athlete-days). For illness, the 3 Olympic sports with the highest incidence were fencing (IR, 13.5 [95% CI, 5.8-26.6], per 1000 athlete-days), diving (IR, 10.9 [95% CI, 1.3-39.5], per 1000 athlete-days), and rowing (IR, 9.3 [95% CI, 3.4-20.3], per 1000 athlete-days), while the 3 Paralympic sports with the highest illness incidence were swimming (9.3 [95% CI, 3.4-20.3], per 1000 athlete-days), cycling (IR, 8.2 [95% CI, 1.0-29.6], per 1000 athlete-days), and triathlon (IR, 6.8 [95% CI, 0.2-37.9], per 1000 athlete-days).
When limiting the sample of athletes to those competing in analogous sports only (Olympics, n = 307; Paralympics, n = 163), there were still no differences in overall injury incidence (IRR, 1.57; 95% CI, 0.97-2.62) or illness incidence (IRR, 0.61; 95% CI, 0.28-1.33) between Olympic and Paralympic athletes. Similarly, none of the comparisons between specific analogous sports revealed any differences in injury or illness incidence (Figure 1).

Incidence of (A) injury and (B) illness by analogous sports for Team USA athletes competing in the Tokyo 2020 Summer Olympic and Paralympic Games. Dots represent incidence rate values, and bars indicate 95% CIs.
Injury and Illness by Anatomic Location and Body System
For Olympic athletes, the body region with the greatest injury incidence was the lower limb (IRR, 5.5 [95% CI, 4.3-7.1], per 1000 athlete-days), while for Paralympians, injury incidence was greatest for injuries to the upper limb (IRR, 5.4 [95% CI, 3.3-8.3], per 1000 athlete-days) (Table 3). The specific anatomic location with the greatest injury incidence was the ankle (IRR, 2.3 [95% CI, 1.5-3.4], per 1000 athlete-days) for Olympic athletes, and for Paralympic athletes, injury rates were equivalent for the shoulder and wrist/hand (both IRR, 1.8 [95% CI, 0.7, 3.7], per 1000 athlete-days). Infections were the most common illness category for both Olympic (IRR, 1.1 [95% CI, 0.6-1.9], per 1000 athlete-days) and Paralympic (IRR, 2.6 [95% CI, 1.2-4.7), per 1000 athlete-days] athletes (Table 4).
Incidence of Injury by Anatomic Location for Team USA Athletes Competing in the Tokyo 2020 Summer Olympic and Paralympic Games a

NA, not applicable.
Significant difference versus Paralympic athletes (P < .05).
Incidence of Illness by Body System for Team USA Athletes Competing in the Tokyo 2020 Summer Olympic and Paralympic Games

Discussion
While previous data from the Beijing 2022 Winter Games reported significantly higher rates of both injury and illness among Paralympic athletes compared with Olympic athletes, 2 we found no differences in either injury or illness IR between Team USA Paralympians and Olympians, even when stratifying by sex or sport. The only differences in IR observed in this cohort were for illness among male and female Paralympians, with male Paralympic athletes at decreased risk of sustaining an illness compared with female Paralympic athletes.
Evidence regarding differences in injury and illness rates between Olympic and Paralympic athletes is mixed, as most data on this topic have been drawn from separately analyzed and published studies from previous Olympic and Paralympic Games, without direct statistical comparison.5,6,8,9,18,21 For example, multinational data reported separately from the Rio de Janeiro 2016 SOG and SPG suggest that Paralympic athletes were at much greater risk compared with Olympic athletes of sustaining an injury (IR: 10.0 [Paralympics 8 ] vs 5.7 [Olympics 21 ] per 1000 athlete-days) or illness (IR: 10.0 [Paralympics 9 ] vs 3.2 [Olympics 21 ] per 1000 athlete-days). In contrast, the multinational data reported from the Tokyo 2020 Summer Games suggest that while there was little to no difference in injury rates (IR: 5.8 [Paralympics 6 ] vs 5.4 [Olympics 18 ] per 1000 athlete-days), Paralympians may have been more likely to sustain an illness compared with Olympians (IR: 4.2 [Paralympics 5 ] vs 2.3 [Olympics 18 ] per 1000 athlete-days). However, without making direct statistical comparisons, it is difficult to make statistically sound, and thus evidence-based, conclusions regarding potential differences in injury and illness burden experienced by Olympic and Paralympic athletes during a Games period.
To date, there have only been 2 attempts to make direct comparisons of injury or illness burden between Olympic and Paralympic athletes.2,4 Clarsen et al 4 monitored Norwegian Olympic and Paralympic athletes over 5 consecutive Summer and Winter Games cycles, including training and non-Games periods, and found that Paralympic athletes reported a higher incidence of health problems (consisting of both injuries and illnesses) compared with Olympic athletes (7.5 cases per athlete per year [95% CI, 7.0-8.0] vs 6.1 cases per athlete per year [95% CI, 5.9-6.3]). Similarly, Anderson et al 2 reported significantly lower rates of both illness (IRR, 0.41; 95% CI, 0.22-0.76) and injury (IRR, 0.56; 95% CI, 0.37-0.87) among Team USA Olympians compared with Team USA Paralympians competing at the Beijing 2022 Winter Games. In contrast, we found no differences in either injury (IRR, 1.18; 95% CI, 0.84-1.68) or illness (IRR, 0.68; 95% CI, 0.41-1.15) rates when directly comparing Paralympic and Olympic athletes competing for Team USA at the Tokyo 2020 Summer Games, even when stratifying by sport or sex.
The reasons underlying the lack of differences observed in this Team USA cohort are unclear but may be related to differences in the risk profile of Summer and Winter Paralympic sports, as our study is the first to focus solely on summer sport athletes. Specific winter sports may place Paralympic athletes at greater risk of injury or illness and thus drive the differences in incidence that have been observed among Paralympic athletes. For example, Anderson et al 2 reported in their study that the higher risk of illness observed among Paralympic athletes was primarily driven by a large number of illnesses among Paralympic athletes competing in biathlon (IR: 33.9 illnesses per 1000 athlete-days). In contrast, we found no differences in injury or illness incidence when comparing specific summer Olympic and Paralympic sports, even when we also compared similar analogous sports. Our data suggest that the differential risk profile that has been observed between Olympic and Paralympic winter sports may not also exist for summer sports, and this lack of sport risk differences may be a major reason behind the similar injury and illness incidence observed between Summer Olympic and Paralympic athletes. However, our data cannot rule out other potential explanations for the difference between our results in summer sport athletes and previous results in winter sport athletes. These potential explanations include the timing of the Olympic and Paralympic Games, which take place in the same geographical location but typically several weeks apart, which may introduce different risk factors related to weather or spread of illness. Additionally, as medical staffs are often quite different between Games, there may be differences in observed injury/illness incidence that are actually related to differences in comfort of reporting depending on the medical staff present during that Games.
Additionally, while we observed no overall differences in injury incidence between Olympic and Paralympic athletes, we did observe differences in the location of injuries between these populations. Among Paralympic athletes, the highest incidence of injury was for the upper limb, while the lower limb had the highest injury incidence for Olympic athletes. These specific differences are possibly a result of some attributes more commonly observed in Paralympic compared with Olympic athletes, such as the increased use of the upper limb for mobility (and thus increased injury risk) in many Paralympic sports, such as wheelchair-based sports.
The overall injury rates for Team USA athletes (Olympics, 14.0 per 1000 athlete-days; Paralympics, 11.7 per 1000 athlete-days) were both much higher than the injury rates reported in the multinational data from the Tokyo 2020 Summer Games (Olympics, 5.4 per 1000 athlete-days 18 ; Paralympics, 5.8 per 1000 athlete-days 6 ). There are several potential explanations for the higher injury incidence among Team USA athletes compared with the larger athlete field, including differences in athlete reporting of injuries and illnesses, access to medical providers during training and competition, differences in risk due to athlete training or profiles, or even clinician-specific factors related to injury and illness evaluation and documentation. While the overall illness IR for Team USA athletes (Olympics, 4.4 per 1000 athlete-days; Paralympics, 6.3 per 1000 athlete-days) were also higher than the reported illness IR for the full athlete field (Olympics, 2.3 per 1000 athlete-days 18 ; Paralympics, 4.2 per 1000 athlete-days 5 ), these illness rates were lower than what has been typically reported from previous Olympic/Paralympic Games,9,10,17,21 which likely represents the increased infection control and prevention strategies put in place for the Tokyo 2020 Summer games as a result of the COVID-19 pandemic.
Limitation
While this study is the first to our knowledge to directly compare injury and illness rates between Olympic and Paralympic athletes competing in a Summer Games, there are some key limitations to note. While the research team implemented a quality control step into the methodological approach and data collection procedures, we were reliant upon the medical providers, (1) documenting all medical encounters observed during the Tokyo 2020 SOG and SPG, and (2) completing the relevant fields regarding diagnosis, injury event/location, and injury mechanism. While our quality control process involving a post hoc review of all medical encounters from the Tokyo 2020 SOG and SPG allowed us to ensure an accurate diagnosis of injury or illness, we were unable to determine time loss as a metric of injury severity due to limitations of our electronic medical record system. However, this limitation within the surveillance system has been corrected to allow for reporting of injury severity and burden during future Games periods. The epidemiological data presented in this study represent the experience of a cohort of Olympic and Paralympic athletes from a single country's delegation, during a single cycle (Tokyo 2020 SOG and SPG). Future research is needed to evaluate whether differences in injury and illness rates exist between Paralympic and Olympic athletes from countries and delegations that differ in characteristics from Team USA, and if there are variations over time between Games. Last, the reported data on injury and illness by specific sport are limited by the ability to maintain athlete confidentiality. Based on the approving institutional review board, sports with <10 competitors could not be individually reported, which is why several sports are combined in our results. This limits the ability to draw conclusions on individual sports with low numbers of participants. Similarly, the overall sample was reduced by approximately 50% when conducting the analogous sport comparisons, so these analyses may have been underpowered for finding differences in incidence between Olympic and Paralympic athletes in analogous sports.
Clinical Implications
Epidemiological data provide important information on the distribution and causes of injuries and illnesses within an athletic population. This study serves as a benchmark for a large single-nation's delegation and highlights potential opportunities to develop and implement targeted injury and illness reduction programs among Olympic and Paralympic athletes. In particular, our data suggest that targeted injury prevention programs should be developed for high-risk sports. Some of these sports are intuitively high risk, such as rugby/wheelchair rugby, gymnastics, and goalball, but our data also suggest a high risk of injury within the sport of tennis during the Olympic Games. For illness, given the higher incidence of illnesses in female Team USA Paralympic athletes, there is a need for enhanced health monitoring and preventive health care services for this group. Additionally, with infections being the most common illness category, implementing robust infection control should be a priority during future Games. However, for injury and illness reduction programs to be most effective, a better understanding of how injury and illness burden among Olympic and Paralympic athletes are affected by sport, season (summer vs winter), and specific impairment types is necessary.
Conclusion
To our knowledge, this is the first study to directly compare injury and illness incidence between Olympic and Paralympic athletes competing in a Summer Games. In contrast to previous results from winter sport athletes, we found no differences in overall injury or illness rates between Olympic and Paralympic Team USA athletes, even when stratified by sex or sport. The continued surveillance of injury and illness among Team USA Olympic and Paralympic athletes is important to establish trends and assist in the development and implementation of targeted injury and illness prevention programs.
Footnotes
Appendix
Incidence of Illness by Sport for Team USA Athletes Competing in the Tokyo 2020 Summer Paralympic Games a

| Sport | Athletes Competing, n | Athlete-Days, n | Total Illnesses, n | Athletes With Illness, n (%) | Incidence Rate per 1000 Athlete-Days (95% CI) |
|---|---|---|---|---|---|
| All | 245 | 3948 | 25 | 24 (9.8) | 6.3 (4.1-9.4) |
| Athletics | 66 | 1244 | 5 | 5 (7.6) | 4.0 (1.3-9.4) |
| Cycling | 16 | 244 | 2 | 2 (12.5) | 8.2 (1.0-29.6) |
| Goalball | 12 | 228 | 0 | 0 (0.0) | 0.0 (0.0-0.0) |
| Sitting volleyball | 12 | 152 | 1 | 1 (8.3) | 6.6 (0.2-36.7) |
| Swimming | 33 | 643 | 6 | 5 (15.2) | 9.3 (3.4-20.3) |
| Triathlon | 17 | 147 | 1 | 1 (5.9) | 6.8 (0.2-37.9) |
| Wheelchair basketball | 24 | 456 | 2 | 2 (8.3) | 4.4 (0.5-15.8) |
| Wheelchair rugby | 12 | 197 | 0 | 0 (0.0) | 0.0 (0.0-0.0) |
| Club/racket/gun sports | 26 | 323 | 7 | 7 (26.9) | 21.7 (8.7-44.7) |
| Combat/power/speed sports | 12 | 127 | 0 | 0 (0.0) | 0.0 (0.0-0.0) |
| Water/horse sports | 15 | 187 | 1 | 1 (6.7) | 5.3 (0.1-29.8) |
Club/racket/gun sports: archery, shooting, table tennis, wheelchair tennis; Combat/power/speed sports: judo, powerlifting, taekwondo, wheelchair fencing; Water/horse sports: canoe, equestrian, rowing.
Final revision submitted June 3, 2024; accepted June 20, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded in part by a research center grant from the International Olympic Committee. J.T.F. has received consulting fees from Sanofi-Aventis US. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of North Carolina at Greensboro (reference No. IRB-FY22-218).