
Abstract
Background:
Because of growing concerns regarding repeated head trauma, in 2016, the United States Soccer Federation (USSF) banned headers for athletes aged ≤10 years and limited athletes aged 11 to 13 years to practicing headers for 30 minutes per week.
Purpose:
To assess whether the USSF header policy was associated with fewer soccer-related concussions after the 2015 season.
Study Design:
Descriptive epidemiology study.
Methods:
A retrospective cohort from the National Electronic Injury Surveillance System database was assessed. Age, sex, and injury type were extracted for all soccer-related emergency department visits between January 1, 2012, and December 31, 2023. Univariate and multiple regression analyses were used to assess concussions as a percentage of all soccer-related injuries based on sex, age group (6-9, 10-13, and 14-17 years), and year. The following time frames were assessed: 2012-2015, 2016-2019, and 2020-2023.
Results:
The proportion of concussions decreased from 8.2% of all soccer-related injuries in 2012-2015 to 6.1% in 2020-2023 (P < .01). The relative risk reduction for soccer-related concussions presenting to an emergency department in 2020-2023 compared with 2012-2015 was 25.6%. Overall, the proportion of concussions among 10- to 13-year-old and 14- to 17-year-old players was higher than for 6- to 9-year-old players (6.6% and 8.9% vs 4.9%, respectively; P < .01). Despite having a lower frequency of soccer-related injuries overall, female players had a greater proportion of concussions than male players (9.6% vs 6.2% of all soccer-related injuries; P < .01). In the multiple regression analysis, injuries that occurred in 2020-2023 were associated with lower odds of concussion compared with 2012-2015 (odds ratio [OR], 0.75 [95% CI, 0.69-0.81]). Compared with 6- to 9-year-old and male players, the 10- to 13-year-old (OR, 1.30 [95% CI, 1.16-1.45]), 14- to 17-year-old (OR, 1.79 [95% CI, 1.61-1.99]), and female players (OR, 1.53 [95% CI, 1.43-1.63]) were associated with higher odds of concussion.
Conclusion:
A 25.6% reduction in the relative risk of presenting to the emergency department with a soccer-related concussion was found when comparing 2020-2023 (after USSF header policy implementation) with 2012-2015 (before policy implementation). The USSF youth soccer header policy may improve player safety by reducing head impacts in the pediatric population.
Soccer is one of the most popular youth sports in the United States and worldwide. 21 It is estimated that 17.6 to 24.5 million adults 25 and 3.9 million children 46 play organized soccer in the United States each year. The overall incidence of pediatric soccer injuries is 5.70 injuries per 1000 hours in male players and 6.77 injuries per 1000 hours in female players, with the most common injuries being muscle and joint injuries in the lower extremities. 42 The concussion incidence in youth soccer is estimated to be 0.19 to 0.28 per 1000 athletic-exposures 39 or 0.5 concussions per 1000 playing hours. 37 Soccer-related concussion injury mechanisms include accidental contact with another player or field equipment, such as a goal post or the field, and intentional contact between the head and the ball in a technique called a header. The most common soccer-related concussion mechanism for male players is contact with another player, and for female players, it is nonplayer contact events. 8 However, among male and female players, 19% to 30% of concussions in youth soccer are attributed to headers.13,26,37
Although concussion sequelae are incompletely understood, several chronic concussion-related health conditions have been identified. Postconcussion symptoms occur in approximately one-third of pediatric patients who sustain a concussion and may persist for months to years.4,48 These symptoms include headache, fatigue, and sound sensitivity and are associated with a reduced quality of life across several domains.20,38 Those who sustain a second concussion before full recovery from an initial concussion are at risk for second impact syndrome, which can result in cerebral edema and death. 34 Pediatric concussions are associated with an increased risk of mental health complaints, psychiatric hospitalizations, and self-harm behaviors compared with other sports injuries. 30 Pediatric patients who sustain a concussion may have a higher risk of developing or exacerbating symptoms of anxiety, depression, conduct problems, and mental health difficulties compared with those without concussion. 19 Repetitive mild traumatic brain injury has also been identified as a risk factor for neurodegenerative diseases—including dementia and chronic traumatic encephalopathy.18,24
Beginning in 2016, the United States Soccer Federation (USSF) implemented the United States Soccer Concussion Initiative to ban headers for all athletes aged ≤10 years and limited athletes aged 11 to 13 years to performing headers in practice only, for a maximum of 30 minutes per week. 43 Compliance with this ban has reportedly been successful. Among youth soccer club survey respondents, 92.5% of clubs adopted the guidelines, 72% avoided headers in practice, and 49% avoided headers in games. 23
This study aimed to assess whether the USSF header policy was associated with fewer soccer-related concussions that presented to an emergency department after the 2015 season. We hypothesized that the odds of sustaining a pediatric soccer-related concussion in 2016-2019 and 2020-2023 would be decreased compared with 2012-2015.
Methods
Data Source
An exemption was granted from institutional review board approval for this preconstructed database-specific study, which utilized a publicly available, deidentified dataset. The National Electronic Injury Surveillance System (NEISS) is a database maintained by the United States Consumer Product Safety Commission to collect data about injuries related to consumer products in the United States. 14 There are approximately 100 NEISS hospitals, which are a stratified sample of all hospitals in the United States that offer 24-hour emergency services and have at least 6 beds; urgent care centers are not included. The NEISS hospitals report patient information for emergency department visits involving all injuries and consumer products, such as sporting equipment or furniture, and these data are used to derive national estimates. The NEISS dataset includes patient information such as age, sex, ethnicity, diagnosis, and product code.
Cohort Selection
The NEISS database was queried for soccer-related injuries from January 1, 2012 to December 31, 2023 (product code 1267). We chose this time frame because 2023 was the most recent year for which data were available, and this 12-year range included 4 years leading up to the implementation of the USSF header policy. The dataset was filtered to include pediatric patients aged 6 to 17 years. This age range was chosen because the ban directly affected players aged ≤13 years, but it may have continued to influence the athletes’ style of play as they aged. Patients with any soccer-related injury were included to measure concussions as a proportion of the total soccer-related injury burden. Patients with a diagnosis code of 52 were defined as having a concussion. Age groups were defined as 6-9, 10-13, and 14-17 years to differentiate athletes who were affected by the header ban. Three separate time frames were analyzed: 2012-2015, 2016-2019, and 2020-2023. The years after the implementation of the 2016 policy were divided because some players in the 14- to 17-year age group had played under the new policy at a younger age between 2016 and 2019. By 2020, all of the athletes who consistently played soccer had been exposed to the new policy.
Statistical Analyses
All data manipulation and statistical analyses were performed in R Version 4.3.3 (R Core Team). Univariate analyses were performed. Patients with concussions were compared with the rest of the cohort and were assessed by sex, age, and year using the chi-square test. Absolute risk reduction and relative risk reduction were reported given that soccer-related concussions are rare events. Statistical significance was set at P < .05. A second univariate analysis was performed according to age group (6-9, 10-13, and 14-17 years) to determine the effects of the USSF header policy on players who were directly affected by it (players aged ≤13 years) and those who were not. A multiple regression model was constructed to predict the odds of concussion compared with all other soccer injuries based on sex, age group, and time frame (2012-2015, 2016-2019, and 2020-2023). The 2012-2015 time frame, which was before the implementation of the USSF header policy, was considered the reference group. Odds ratios (ORs) were reported with corresponding 95% CIs.
Results
Concussions According to Time Frame
From 2012 to 2015, a total of 21,013 soccer-related injuries presented to an emergency department participating in the NEISS database, of which 1729 were concussions (8.2%). From 2016 to 2019, there were 21,267 soccer-related injuries, of which 1614 were concussions (7.6%), and from 2020 to 2023 there were 16,695 total injuries and 1012 concussions (6.1%) (Table 1). The relative risk reduction for soccer-related concussions presenting to an emergency department setting in 2020-2023 compared with 2012-2015 was 25.6%.
Soccer-Related Concussions Presenting to US Emergency Departments, 2012-2023 a
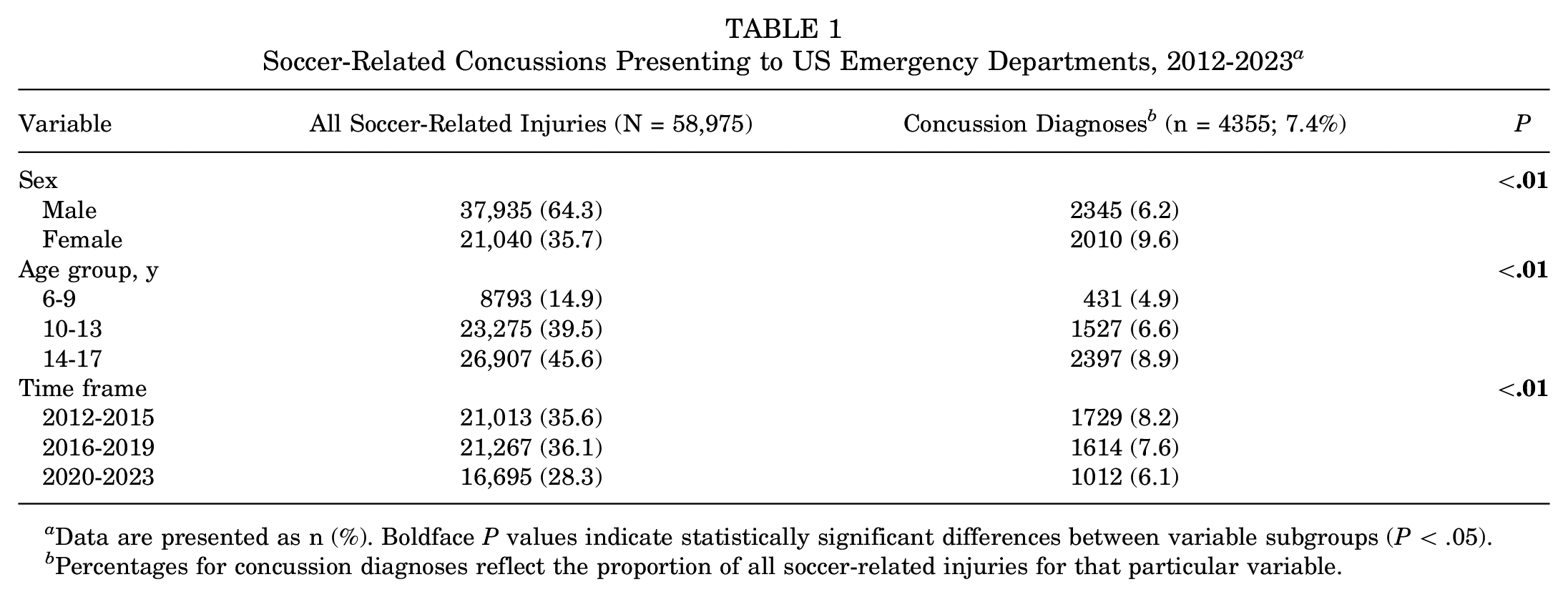
Data are presented as n (%). Boldface P values indicate statistically significant differences between variable subgroups (P < .05).
Percentages for concussion diagnoses reflect the proportion of all soccer-related injuries for that particular variable.
No statistically significant difference was observed between concussions that occurred between 2012-2015, 2016-2019, and 2020-2023 in the 6- to 9-year age group. In this age group, concussions comprised 5.1% of soccer-related injuries in 2012-2015, 4.9% in 2016-2019, and 4.6% in 2020-2023 (P = .66) (Table 2 and Figure 1). In the 10- to 13-year age group, concussions accounted for 7% of soccer-related injuries in 2012-2015, 7.1% in 2016-2019, and 5.3% in 2020-2023 (P < .01) (Table 2 and Figure 1). In the 14- to 17-year-old age group, concussions accounted for 10.3% of soccer-related injuries in 2012-2015, 8.9% in 2016-2019, and 7.2% in 2020-2023 (P < .01) (Table 2 and Figure 1).
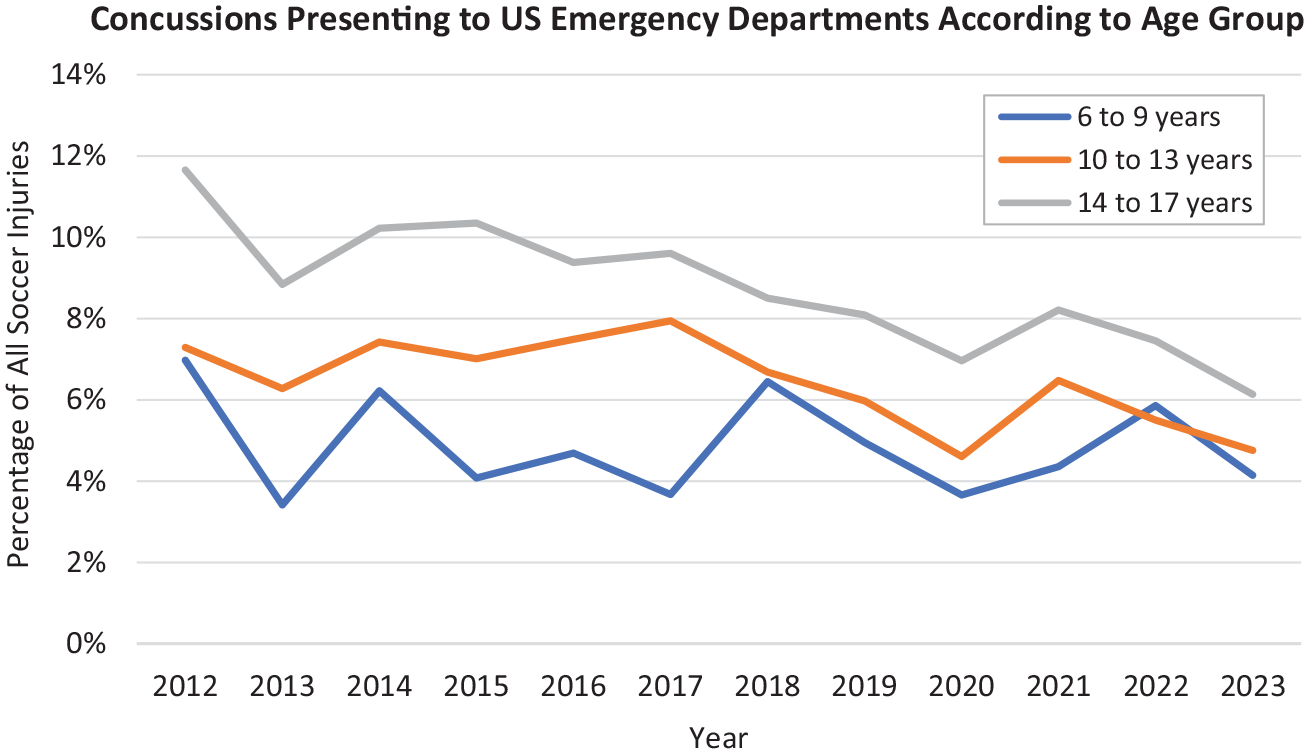
Concussions presenting to US emergency departments as a percentage of total soccer injuries, stratified by age group. US, United States.
Soccer-Related Concussions Presenting to US Emergency Departments Stratified by Age Group, 2012-2023 a
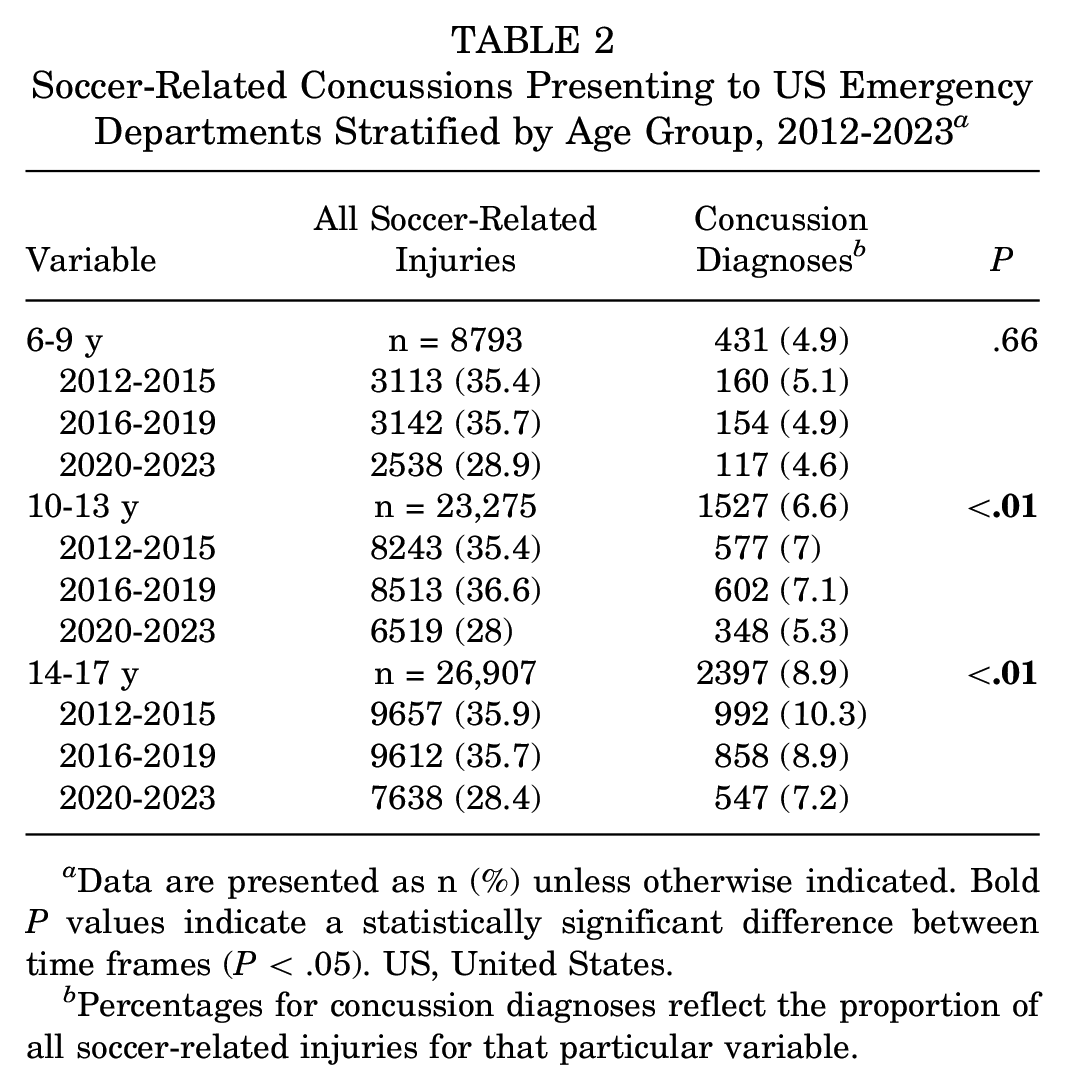
Data are presented as n (%) unless otherwise indicated. Bold P values indicate a statistically significant difference between time frames (P < .05). US, United States.
Percentages for concussion diagnoses reflect the proportion of all soccer-related injuries for that particular variable.
On multiple regression analysis, injuries that occurred in 2020-2023 were associated with lower odds of concussion compared with 2012-2015 (OR, 0.75 [95% CI, 0.69-0.81]) (Table 3). The odds of soccer-related concussion in 2016-2019 were not significantly different than in 2012-2015 (OR, 0.94 [95% CI, 0.88-1.01]) (Table 3).
Results of Multiple Regression Predicting Soccer-Related Concussion Compared With All Other Soccer Injuries a

Dashes indicate areas not applicable. Bold P values indicate statistical significance (P < .05). OR, odds ratio.
Concussions According to Age
Soccer players aged between 14 and 17 years experienced more soccer-related injuries and a higher proportion of soccer-related concussions than players aged 10 to 13 years, who in turn experienced more injuries and concussions than players aged 6 to 9 years. There were 8793 total soccer-related injuries and 431 concussions (4.9%) in 6- to 9-year-old players. A total of 23,275 soccer-related injuries were reported in 10- to 13-year-old players, of which 1527 were concussions (6.6%). A total of 26,907 soccer-related injuries were reported in 14- to 17-year-old players, of which 2397 were concussions (8.9%). Univariate analysis showed a statistically significant higher proportion of concussions in the 2 older cohorts compared with the 6- to 9-year-old players (P < .01) (Table 1). Compared with the 6- to 9-year-old players, the 10- to 13-year-old players (OR, 1.30 [95% CI, 1.16-1.45]) and 14- to 17-year-old players (OR, 1.79 [95% CI, 1.61-1.99]) had higher odds of being diagnosed with a soccer-related concussion on multiple regression analysis (Table 3).
Concussions According to Sex
Female players experienced fewer overall soccer-related injuries than male players, but a greater proportion of their injuries were concussions. Female players presented to the emergency department for 21,040 soccer-related injuries between 2012 and 2023, of which 2010 were concussions (9.6%). Male players were seen for 37,935 soccer-related injuries, of which 2345 were concussions (6.2%). On univariate analysis, male soccer players had fewer concussions as a percentage of soccer-related injuries than female soccer players (P < .01) (Table 1). The proportion of concussion diagnoses for both male and female players was lowest in 2023, at 4.3% and 7.8%, respectively. The highest annual proportion of concussion diagnoses was 8.4% for male players and 10.5% for female players, both in 2012 (Figure 2). On multiple regression analysis, female sex was a slightly significant predictor of increased odds of concussion (OR, 1.53 [95% CI, 1.43-1.63]) (Table 3).

Concussions presenting to US emergency departments as a percentage of total soccer injuries, stratified by sex. US, United States.
Discussion
The main finding of this study was a 25.6% relative risk reduction in concussions as a percentage of all soccer-related injuries that presented to the emergency department in 2020-2023 compared with 2012-2015. The decrease in the proportion of soccer concussion injuries per total soccer injuries presented to the emergency department coincided with the adoption of the USSF policy that banned headers in players aged ≤10 years and limited headers in players aged 11 to 13 years to a maximum of 30 minutes of practice a week. While this finding does not prove that the policy caused a decrease in concussion injuries among youth soccer players, our study establishes an association between policy implementation and a decrease in the proportion of soccer-related concussions. Further, this finding remained significant after accounting for differences because of age and sex.
Our results conflict with previous findings from a 2020 study that suggested concussion rates increased after the USSF header policy and instead support the hypothesis that the odds of concussion decreased after the implementation of the USSF header policy. 29 However, the previously reported increase in concussion rates may be attributable to an overall increase in concussion awareness, which is supported by an increase in concussions in the general adult and pediatric populations during the same period.3,41,44 Another explanation for these contrasting findings may have been a delay between policy implementation and widespread policy adoption by soccer teams. Although behavioral data are not available, it is possible that youth players who were 10 years old in 2016 maintained some level of header avoidance for the rest of their youth career if policy-directed header avoidance during childhood had a long-term effect on play style. This change in style of play may have resulted in a larger decrease in the proportion of concussions in 2020-2023. This is supported by unchanged odds of concussion in 2016-2019 compared with 2012-2015 but decreased odds of concussion in 2020-2023 compared with 2012-2015. It is reasonable to theorize that the 25.6% relative risk reduction in concussions found in this study may be related to headers since headers account for approximately 19% to 30% of soccer concussions.13,26,37 Other mechanisms of injury, such as collisions with other players, are unlikely to have been affected by this policy, but our data were unable to specify the definitive cause for our findings. The use of headgear is not associated with reduced rates of soccer-related concussions, and no changes in equipment or technology were identified to explain this trend.1,31 No similar header policies have been identified in other countries to provide a comparison. A Canadian ice hockey policy to eliminate body checking reduced concussion risk nearly 3-fold in youth players, which supports the general efficacy of injury-prevention policy. 6 Overall, while the policy change may have contributed to a decrease in concussions, further system changes such as mandated injury reporting would help create a more accurate dataset to determine the effect of policy on injury prevention. Another strategy to improve player safety would be to enroll players in an injury prevention program, which has been effective in reducing overall injury risk and risk of concussion. 22 Although current equipment does not protect against concussion, this may be possible in the future as technology advances.1,31
Older athletes were more likely to sustain a concussion than younger athletes across all time points, yet the older age groups exhibited larger decreases in concussions as a percentage of total injuries after the header policy was implemented. Concussions comprised 8.9% of all soccer-related injuries in the 14- to 17-year-old players compared to 6.6% in the 10- to 13-year-old players and 4.9% in the 6- to 9-year-old players, and athletes who were 10 to 13 years old and 14 to 17 years old had increased odds of concussion. These results align with previous findings that among adolescent athletes, older age is associated with an increased incidence of concussion and increased head-impact exposure.11,12,26,27 This is likely due to a combination of factors, including a higher level of play among older athletes, increased contact forces between athletes, including head-to-head contact, and faster ball speed at which players head the ball. There was also an interaction between age and year, such that the older age groups experienced a significant decrease in concussions between 2012-2015 and 2020-2023 that the younger age group did not. This is inconsistent with previous findings from Lalji et al 29 that stated that the concussion rates among 10- to 13-year-old players increased after the USSF header policy, but their study analyzed data for only 2 years after the policy was implemented. 29 Their results may be due to poor compliance or delayed implementation of the new policy that improved in future years. Possible explanations for the findings in the present study may be that the USSF header policy increased awareness regarding head safety among adolescent soccer players and their guardians outside of the intended ≤13 age range or that as players who grew up with the USSF header policy became older, they continued to perform headers less frequently than those who grew up practicing headers. In addition, improved heading technique and mechanics as adolescents age may play a role. On the other hand, a time-based effect might be masked in the younger cohort because increased awareness of concussions may have led to increased reporting. While the effects of the USSF header policy cannot be directly determined from these data, these results suggest that limiting headers in 10- to 13-year-old players is more effective in reducing the frequency of soccer-related concussions that present to emergency departments than banning headers in 6- to 9-year-old players.
Female players were diagnosed with a higher proportion of concussions compared with all soccer-related injuries than male players and female sex was associated with increased odds of concussion. These results are concordant with previous findings that female sex is associated with increased sport-related concussion risk in pediatric patients and that female soccer players are exposed to head-impact forces of greater magnitude than male soccer players.8,11,12,47 Compared with male players, female players are more likely to sustain a concussion while performing a header as opposed to other mechanisms of injury, such as colliding with another player.8,15 Female athletes experience increased linear and rotational acceleration while performing a header, which could be attributed to reduced neck size and strength compared with male athletes.7,10 There are some suggestions that hormonal differences during the menstrual cycle also affect injury risk in female athletes, although there is limited research studying how these factors influence concussions.7,28,32 Concussions may present differently in males and females; males are more likely to report amnesia and disorientation, whereas females are more likely to report drowsiness, light and sound sensitivity, and headache.9,17 Female athletes are also found to report more severe concussion symptoms than their male counterparts; thus, the observed sex difference may also be due to a greater proportion of female athletes presenting to the emergency department because of the severity of their symptoms.2,5,33,49 Furthermore, male athletes are more likely to underreport concussion symptoms than female athletes.36,45 According to survey data of high-school athletes, female athletes have greater knowledge of concussion symptoms, and male athletes are more likely to cite a variety of reasons for not reporting a potential concussion. 45
Limitations
This study has several limitations. The NEISS database only included data from emergency department visits, which likely underrepresented the total incidence of concussions among soccer players. Concussion symptoms are underreported by athletes, and many athletes who may have been concussed did not visit the emergency department, which could have resulted in a response bias.16,35 On the other hand, recent increased awareness regarding concussions may have led to higher rates of reporting in more recent years compared with previous years. This database only included information from 100 hospitals, and although these hospitals were selected to be a representative sample of the United States, they may have over- or underrepresented soccer-related injuries. Data that quantify the total number of athletes who play soccer are not available, and the database does not allow for the assessment of repeat injuries sustained by the same athlete. The NEISS database does not include data from urgent care centers, which are being utilized more frequently for low-acuity conditions. 40 This shift in the setting of care to urgent care centers, primary care providers, and specialists could artificially lower the proportion of soccer-related concussions seen in the emergency department. The NEISS database coding system is not consistent with the International Classification of Diseases, Tenth Revision codes, which could result in missed or inaccurate diagnoses. The coronavirus disease 2019 pandemic may have also influenced the results, even though soccer concussions were measured as a percentage of total soccer-related injuries. However, the proportion of athletes participating in organized soccer likely decreased compared with those participating in unorganized soccer, which may involve a different style of play. Unlike organized sports databases, the NEISS database includes players who may not be aware of or follow the USSF header policy.
Conclusion
The USSF youth soccer header policy implemented in 2016 was associated with a 25.6% relative risk reduction of presenting to the emergency department with a soccer-related concussion in 2020-2023 compared with 2012-2015. A header ban in players aged ≤10 years and a limitation to 30 minutes of header practice a week in players aged 11 to 13 years may improve player safety by reducing head impacts.
Footnotes
Final revision submitted October 3, 2024; accepted November 8, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.A.L. has received education payments from ImpactOrtho. A.H. has received hospitality payments from Arthrex. M.R. has received education payments from Arthrex and hospitality payments from Stryker. A.C. has received consulting fees from Smith+Nephew and Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.