
Abstract
Background:
Little information is available on the embryology of the structures that connect the lateral meniscus to its nearby structures (proximal tibia, fibular head, and popliteus tendon), which restrict lateral meniscal extrusion.
Purpose:
To describe the menisco-tibio-popliteus-fibular complex (MTPFC)—conformed by the lateral meniscotibial ligament (LMTL), popliteofibular ligament, meniscofibular ligament, and the 2 popliteomeniscal ligaments (superior and inferior)—and anterolateral ligament (ALL) of the knee in human embryos/fetuses from weeks 9 to 37 of gestation.
Study Design:
Descriptive laboratory study.
Methods:
The authors analyzed 36 formalin-fixed embryos/fetus knees, ranging between weeks 9 and 37 of gestation. All had normal external morphological characteristics. A microdissection was performed by meticulously searching the structures of the MTPFC and the ALL, their anatomic relationships, and their appearance over time. Histological sections were taken of the entire knee, the lateral meniscus, the ALL, and the LMTL to observe its structure from its early stages, junctions, and cellularity. In addition, the composition and orientation of the fibers were evaluated.
Results:
The MTPFC was not found in the youngest knees (9 weeks). The ligaments of this complex could not be seen until week 11 of development. Moreover, the ALL was a consistent finding from the 13th week of development onward. All the ligaments of the MTPFC were seen between developmental weeks 11 and 16 in all the specimens. The histological results showed that the histology of the ALL showed dense connective tissue organized into thick bundles of collagen fibers in its central portion, with a parallel and undulating arrangement and the anterolateral capsule demonstrated 3 easily distinguishable layers corresponding to the fibrous membrane, the subsynovial membrane formed by loose connective tissue, and the synovial membrane.
Conclusion:
All the structures of the MTPFC were visualized from week 11, with the LMTL being the first to form. Moreover, the ALL was a consistent finding from week 13 of development onward.
Clinical Relevance:
Understanding the embryological development of the MTPFC and the ALL of the knee is clinically relevant, as it can provide crucial insights into the pathogenesis of knee conditions and inform treatment strategies. By elucidating the timeline and characteristics of these structures’ formation, clinicians can better diagnose and manage conditions affecting the lateral meniscus and related structures, ultimately improving patient outcomes and surgical interventions.
The anatomy of the lateral compartment of the knee has been studied and documented extensively in adults; however, only a few studies have been conducted on its embryological origin and stages of formation. 20 Masferrer et al 16 performed an anatomic study in adult knees and denominated this anatomic region that connects the lateral meniscus, proximal tibia, popliteus tendon (PT), and fibular head as the menisco-tibio-popliteus-fibular complex (MTPFC). It consists of 5 ligaments: the lateral meniscotibial ligament (LMTL), the popliteofibular ligament (PFL), the meniscofibular ligament (MFL), and the 2 (superior and inferior) popliteomeniscal ligaments (PML).16,19 These structures are important, as they limit the extrusion of the lateral meniscus.16,18 It is essential to study embryology and histological characteristics of these ligaments to help understand the injuries that cause meniscal extrusion and their treatment.25,6
It has been stated in the literature that the lateral collateral ligament (LCL) begins to organize and extends caudally to the fibular head by the eighth week of embryonic development. 21 At 10 weeks, the LCL is visible and parallel to the lateral surface of the joint. The PT is attached to a small pit below the lateral epicondyle of the femur, and its relationship to the LCL is visible. 20 Previous publications have not studied and described the embryonic development of the MTPFC.2,8,15 Therefore, an embryological study focused on the description of this complex is called for.
The menisci are formed from mesenchymal tissue in the knee joint between weeks 8 and 10 of embryonic development.2,15 O’Rahilly and Müller 20 described the development of the knee joint and established a multiphase morphogenetic timeline. During phase 23, which is comparable to the tenth and eleventh weeks of development, the meniscus becomes distinguishable.9,20 Kabakçı et al 14 found that the second and third trimesters are when the lateral meniscus shows more morphological development.
The anterolateral ligament (ALL) of the knee is a structure described in 2013. 1 It originates near the lateral epicondyle of the femur and is inserted between the Gerdy tubercle and the fibular head, expanding to the lateral meniscus.10,27 It has recently been the focus of a study in which a controversy has arisen around its fetal development.21,22,26 The ALL is an anatomic structure that has an intrinsic relationship with the lateral meniscus.4,11 In addition, it is of increasing interest because of its association with lateral meniscal tears, anterior cruciate ligament injuries, and anterolateral instability. Sabzevari et al 22 studied embryos with a gestational age between 18 and 22 weeks and reported no ALL of the knees. 22 Other studies have not found the ALL in fetuses 5 or heterogeneously in the pediatric population.13,23,24 On the other hand, other authors11,26 studied human fetuses between 25.5 and 37.3 weeks and concluded that the ALL is a structure that is always present during fetal development and has anatomic and histological characteristics similar to those of adult ALL. The older age of the specimens in recent studies and a thorough dissection of the knee along with better fetus preservation protocols are some of the reasons for the contradictory results between these studies. This study is the first to use embryos and fetuses from the final stages of embryonic development to the final stages of fetal development, with specimens representative of most weeks of formation.
Little information is available on the development of the MTPFC in the embryonic/fetal knee; therefore, this research aimed to describe the MTPFC and the ALL of the knee in human embryos/fetuses between weeks 9 and 37. We hypothesized that the structures of the MTPFC and the ALL would be constantly observed between developmental weeks 11 and 16 and through all the late embryonic and early fetal stages and that its origin and relationship with the lateral meniscus could be described.
Methods
A total of 36 formalin-fixed fetus knees, with normal external morphological characteristics, ranging from 9 to 37 weeks of gestation (mean, 25.4 ± 8.4 weeks), were evaluated. All fetuses were donated by the embryology department of our institution and were voluntarily donated by their parents. Twenty knees were from male fetuses (56%) and 16 from female fetuses (44%). The local ethics committee for clinical research of our institution approved the study protocol, with registration No. FI22-00001.
All the fetuses and embryos were fixed in formaldehyde 10%. Embryos with anatomic defects, lesions associated with structural deformities, and those of unknown age and sex were excluded. Four embryos of each developmental age (9, 11, 13, 16, and 19 weeks) were included. Two knees from fetuses in the 21st, 24th, 25th, 28th, 30th, 32nd, 35th, and 37th developmental weeks were included. The length of the fetuses was not determined because of the great difference between the embryos and fetuses with longer weeks of gestation.
Dissection Protocol
Previously published studies were used as a basis, with some variations by our group.3,4,12 A careful microscopic dissection was made with 4x lenses (Axiostar Plus). A lateral curve approach from 0.5 to 2 cm (depending on the age of the specimen) proximal and posterior to the lateral epicondyle to the middle of the lateral aspect of the leg after the posterior border of the head of the fibula was identified. Subsequently, the iliotibial band and the biceps femoris tendon were identified, dissected, and incised proximal to the joint line. Both were then reflected proximally to allow for better visualization of the deep structures. Afterward, a blunt dissection was performed and the LCL, the PT, and the PFL were found and visualized. Next, the LCL and the PT were sectioned on the femoral side to expose the entire lateral compartment. The lateral capsule anterior to the LCL was carefully dissected, and the ALL was identified as a thickening of the lateral capsule between the LCL and the patellar tendon, which originates posterior and proximal to the lateral epicondyle and is inserted lateral to the patellar tendon on the lateral proximal tibia between the Gerdy tubercle and the head of the fibula. The ALL was dissected from its tibial to its femoral insertion. 11 The complete lateral meniscus was extracted, sectioning through both meniscus roots. All the structures from the MTPFC described 16 (LMTL, PFL, MFL, and PML) were identified, evaluated, and collected to be processed for histological examination. Moreover, the topographical relationships between the structures were analyzed. In specimens from >16 weeks of gestation, magnifying glasses were utilized for the examination. All the photos were taken with a Zeiss Stemi 508 Stereo microscope with an Axiocam camera (Zeiss).
Histological Study
The fixed samples were dehydrated with ethyl alcohol, rinsed with toluene, and embedded in paraffin. Then, they were cut into a thickness of 10 and 7 μm in the microtome. Then, they were deparaffinized with heat. Finally, the samples were stained with hematoxylin and eosin to assess the cellular components and general tissue, orcein to identify the elastic fibers, and Masson trichrome to identify collagen fibers. Samples were obtained in the sagittal and axial plane of the lateral meniscus, anterolateral capsule, LCL, and ALL, as well as the entire knee in the sagittal plane (only for specimens from 11 to 16 weeks). The qualitative description compared the 3 different samples with respect to thickness, content of dense connective tissue, fiber orientation and arrangement, presence of cellular material, presence of fibroblasts, adipose tissue, muscle fibers, synovial membrane, as well as the type and size of the blood vessels. A standardized magnification of 10-fold, 40-fold, and 100-fold was applied for microscopic evaluation of the samples. The microscopic evaluation and comparison of the samples was performed with a Nikon Eclipse 50i light microscope and an image analysis system that included NIS-elements Advanced Research software, Digital Sight DS-2Mu, and ImageJ program Version 1.49 (National Institutes of Health).
Results
The youngest embryos analyzed were from 9 weeks of gestation. In this dissection, the meniscus and the proximal tibial cartilage were not completely separated as 2 different structures but could be differentiated in a thorough examination. In that examination, the meniscal structure was thicker than the surrounding tissue but attached to the tibia of the embryo. When the meniscus is separated from the tibia, we can see a structure that binds the tibia to the meniscus. Further on, this structure will form the LMTL and the MFL (Figure 1A). At this developmental point, the ligaments of the knee cannot be differentiated from the surrounding tissue.
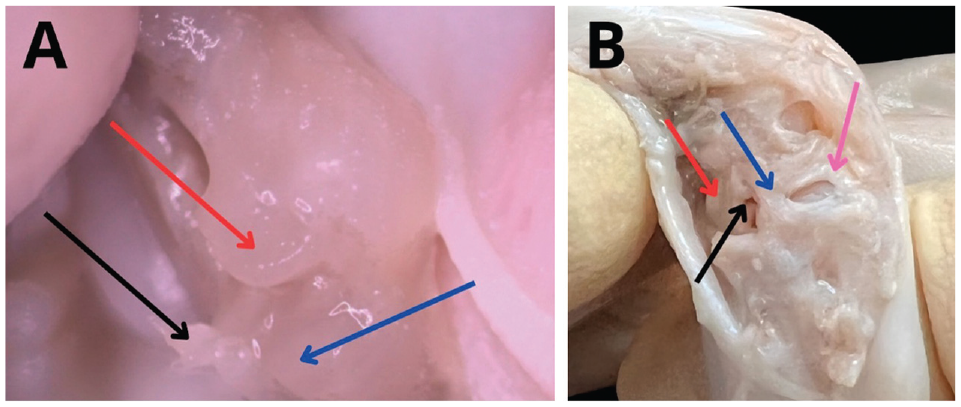
(A) A lateral view of the right knee of a 9-week embryo, where the lateral aspect of the knee is extended, but no ligamentous structures can be seen. The femur (red arrow) and tibia (blue arrow) tissue that connects the meniscus to the tibia; we hypothesized that it would become the lateral meniscotibial ligament (black arrow). (B) A lateral view of a 22-week embryo knee where the lateral meniscotibial ligament (pink arrow), the meniscal fibular ligament (blue arrow), the popliteus muscle (red arrow), and the popliteus meniscal ligaments are present (black arrow).
In fetuses from >11 weeks of gestation, the insertion of a conical structure that can be characterized as the popliteus muscle was seen (Figure 1B). The cavitation of the lateral structures of the knee, along with the extensions that will later form the LMTL and the MFL, was also observed. They can be seen as extensions of the lateral meniscus (Figure 1B). This is the week when the LMTL, the MFL, and the cavitation of the lateral structures of the knee with a conical structure, which can be characterized as the PT in 11 weeks, can be identified for the first time (Figure 2).

Fetal right knee at 11 weeks of gestation in an oblique view in which the lateral collateral ligament is dissected, and the popliteus tendon (black arrow), the lateral meniscus (blue arrow), and the femur (red arrow) are shown. The lateral meniscotibial ligament is held in the clamp.
In week 13, a translucent and wide fibrous band spanning the lateral femoral epicondyle to the anterolateral proximal tibia, posterior to the Gerdy tubercle was identified; it became the ALL

(A) In this lateral view, the ALL can be seen in the right knee at 13 weeks of gestation, indicated with a black arrow. The red arrow indicates the LCL. (B) A lateral view of a 32-week embryo knee where the ALL is referred (black arrow) and the LCL is pointed with a red arrow. ALL, anterolateral ligament; LCL, lateral collateral ligament.

(A) The meniscofibular ligament (green asterisk) is a linear thin structure that binds the meniscus (red asterisk) to the fibular head (black asterisk) in an embryo at 11 weeks. (B) Meniscal dissection of a 22-week embryo: the meniscofibular ligament (green asterisk), the meniscus (red asterisk), and the lateral meniscotibial ligament (orange asterisk).

(A) The popliteus-meniscal ligaments (red arrow), 2 thin linear structures that connect the posterior region of the lateral meniscus (blue arrow) and join the upper and lower zones of the meniscus to the popliteal tendon (black arrow). (B) A lateral view of a 20-week embryo knee where the meniscus (blue arrow), meniscotibial ligament, meniscofibular ligament (red arrow), popliteus muscle (black arrow), and popliteofibular ligament (green arrow) are present.
Histological Analysis
The histology of the anterolateral capsule demonstrated dense connective tissue organized into a thin layer in the peripheral portion, consisting of densely organized collagen fibers and fibroblasts (fibrous membrane). Beneath this layer was a layer of loose connective tissue (subsynovial membrane), highly vascularized, and the synovial membrane with an abundant number of round-nucleus synoviocytes was in the innermost portion (Figure 6). No elastic fibers were present.
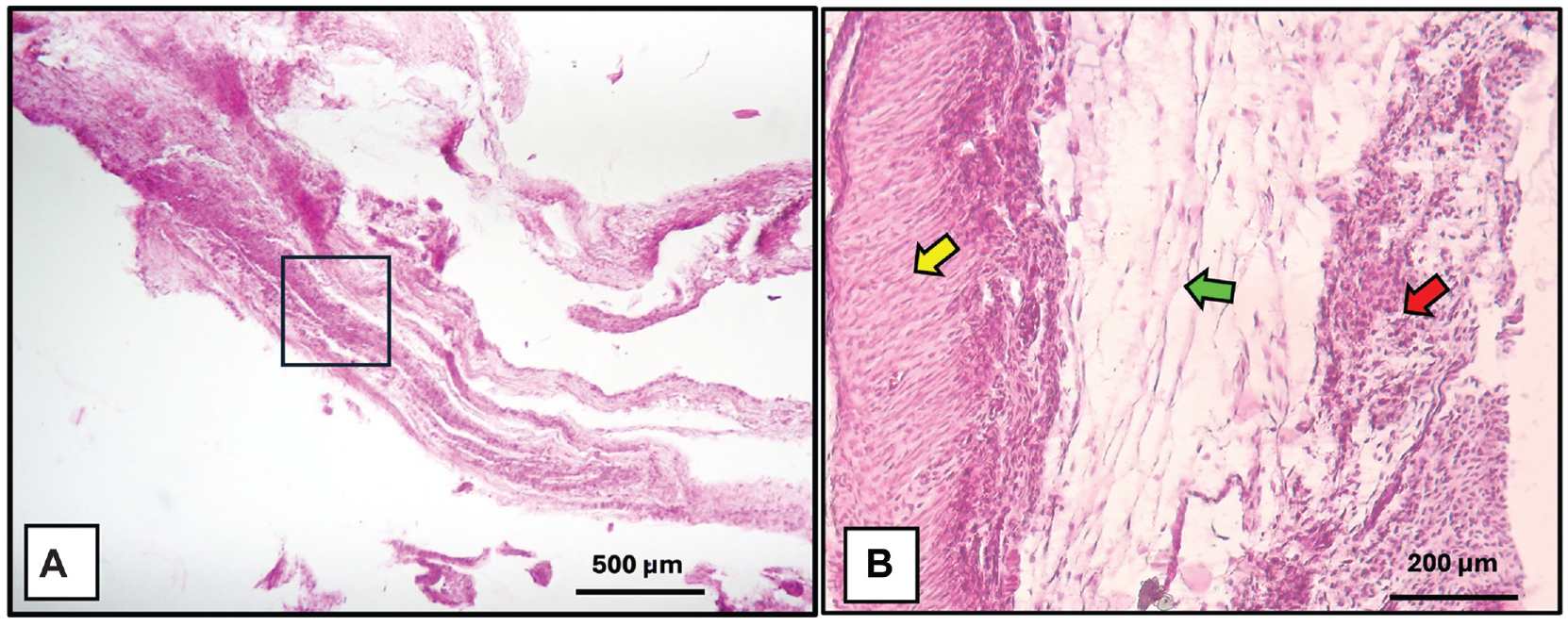
(A) Histological sections of the anterolateral joint capsule. (B) Fibrous capsule (yellow arrow), subsynovial membrane (green arrow), and synovial tissue (red arrow). Specimen of 26 weeks of gestation. The black boxes represent the approach zones on the right.
The histology of the ALL showed dense connective tissue organized into thick bundles of collagen fibers in its central portion, with a parallel and undulating arrangement, alternating with collagen fibers oriented in a radial arrangement at its ends corresponding to the bony insertion sites, as well as elastic fibers in its peripheral portions and a looser arrangement of collagen fibers in the same area. Similarly, there was a scant amount of blood vessels and diminished cellularity compared with the anterolateral capsule, mainly consisting of fibroblasts with elongated nuclei (Figure 7).

Sagittal sections of the anterolateral ligament of a human fetus at 25 weeks of gestation. Note the arrangement of collagen fibers in longitudinal (black arrow) and transverse (red arrows) directions, elastic fibers (blue arrow), and blood vessels (yellow arrows). Light microscopy. A and B: H&E staining. C and D: Orcein staining. H&E, hematoxylin and eosin. The black boxes represent the approach zones on the right.
Figures 8 and 9 depict sagittal sections of complete knees at 9 and 11 weeks of gestation, respectively. At 9 weeks of gestation, the osseous component of the knee, the posterior cruciate ligament, and the menisci are already formed (Figure 8, A-C). However, there is no complete formation of the articular capsule and no distinction between the meniscal parenchyma and the articular capsule appearing as a single structure (Figure 8, D and E). At 11 weeks, there is already differentiation of the articular capsule and the lateral meniscus, and the articular capsule is fully formed (Figure 9).

Sagittal sections of the knee of a human fetus at 9 weeks of gestation—including the femur (light blue arrow), patella (pink arrow), tibia (green arrow), muscle (yellow arrow), quadriceps tendon (gray arrow), posterior cruciate ligament (black arrow), posterior horn of the meniscus (orange arrow), anterior horn of the meniscus (red arrow), patellar tendon (white arrow), meniscotibial ligament (brown arrows), and meniscocapsular ligament (dark blue arrow). Light microscopy. A, B, and C: Masson trichrome stain. D and E: H&E staining. H&E, hematoxylin and eosin. The black boxes represent the approach zones on the right.

Sagittal sections of the knee of a human fetus at 11 weeks of gestation—including the femur (light blue arrow), tibia (green arrow), muscle (yellow arrow), joint capsule (gray arrow), posterior horn of the meniscus (orange arrow), anterior horn of the meniscus (red arrow), meniscocapsular ligament (white arrow), and meniscotibial ligament (brown arrow). Light microscopy. A, B, and C: Masson trichrome stain. D and E: H&E staining. H&E, hematoxylin and eosin. The black boxes represent the approach zones on the right.
Discussion
The main finding of this study was that the complete formation of the MTPFC could be observed and described between weeks 11 and 16 of development, and the ALL from week 13 of gestation.
At 9 weeks, the lateral condyle, lateral meniscus, and some extensions that will further form the lateral meniscotibial-ligament can be seen. At 11 weeks of development, we could observe the extension from the lateral epicondyle to the fibular head, which will form the LCL and the LMTL, is completely formed. Moreover, a prolongation from the anterior part of the lateral femoral epicondyle that inserts between the Gerdy tubercle and the fibular head was seen. However, the complete formation of the ALL occurs at 13 weeks of development. From 16 weeks of development, we found a consistent pattern, and we could see the complete MTPFC as a formed structure. From 19 weeks onward, there was continuing thickening of these structures up to the forming of a mature knee.
Mérida-Velasco et al 17 reported the formation of both menisci starting at 9 weeks of embryonic development, similar to the descriptions provided by O’Rahilly and Müller. 20 They also described7,17,20 the formation of a ligament that attaches the meniscus to the proximal tibia during weeks 12 to 13; both assertions align with our findings. Like their studies, we found that the capsule and the menisci are condensed in the same structure without clear differentiation in the ligaments between the structures in weeks 9 to 11.
Gardner and Gray 8 found that the entire periphery of the lateral meniscus is not fused to the capsule. The posterior margin of the meniscus is adjacent to the articular recess that separates the lateral meniscus from the popliteal tendon. They also stated that the lateral meniscus is attached to the popliteal tendon along its superior or inferior margin, depending on the section considered. 21 The popliteal tendon maintains its position while the fibula descends to a more distal location. 21 This process brings about the elongation of the PFL and the MFL, which can also be found on the posterior aspect of the adult knee. 21 Their results coincide with ours.
The first structure found in this region was the LMTL, observed from developmental week 11. Fetuses of 13 weeks show clear differentiation between the menisci and tibial cartilage. The MFL and the LMTL keep similar histological structures since their formation. These 2 structures are also in a close relationship since they appear in the younger embryos (Figure 10). This may explain having a similar embryologic origin. The MFL and the PFL elongate with the distalization of the fibular apex. These structures demonstrate the complicated connection between the lateral meniscus and the fibular head to prevent the meniscal extrusion of the knee.16,19 Moreover, the MTPFC was found in all the specimens after developmental week 16.

A lateral view of a 19-week embryo knee, where the lateral meniscotibial ligament can be seen (black arrow). The red arrow is pointing to the meniscofibular ligament.
The ALL was observed as a constant extracapsular structure in the lateral side of the knee in all of the fetuses examined from developmental week 13 onward, similar to Helito et al 11 and Toro-Ibarguen et al. 26 We can conclude that this is a constant ligament in the embryonic knee from week 13. In the same way, this ligament finding and its correlation with the capsule and the lateral meniscus demonstrate the intricate relationship between the ALL, the LCL, and the lateral meniscus. An older age of the specimens in a recent study and a thorough dissection of the knee along with better fetus preservation protocols are some of the reasons for the contradictory results between previous studies. 22 This study is the first to use embryos and fetuses from the final stages of embryonic development to the final stages of fetal development, with specimens representative of most weeks of formation.
Regarding clinical relevance, a previous study has shown that injury to the LMTL and the MFL significantly increases meniscal extrusion, and its repair restores meniscal extrusion to its native values. 18 Thus, understanding the embryological origin and stages of formation will help better understand the anatomy and function in adulthood and help implement surgical techniques for their reconstruction.
Limitations and Strengths
We had a small sample, but the findings were consistent in all weeks. More studies with a larger sample are needed to study the embryonic to fetal development of the MTPFC. Another significant limitation is the difficulty in performing microdissections in the early stages of development, which could lead to observation bias. One of the strengths of this study is that we had embryos in the very early developmental stages in our sample, and we could observe the first developmental weeks of the MTPFC and the ALL.
Conclusion
All the structures of the MTPFC begin to be visualized from week 11. The first structure to develop is the LMTL in week 11, ending with the PML in week 16 of development. The ALL was a consistent finding from week 13 of development.
Footnotes
Final revision submitted May 18, 2024; accepted May 23, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Universidad Autonoma de Nuevo Leon (FI22-00001).