
Abstract
Background:
Functional recovery and return to sports after fixation of osteochondritis dissecans (OCD) lesions of the knee with osteochondral autologous transplantation (OAT) have not been well investigated.
Purpose:
To retrospectively evaluate the functional recovery and clinical outcomes after internal fixation with OAT for knee OCD.
Study Design:
Case series; Level of evidence, 4.
Methods:
A consecutive series of patients who underwent OAT for OCD lesions between 2010 and 2020 were initially enrolled in the study. Patients with adult-onset OCD and those who underwent fragment removal and/or mosaicplasty were excluded. Lysholm score, Tegner activity scale, return-to-sports rate (at the practice/training and preinjury levels), and time to return were evaluated. Clinical factors influencing postoperative functional recovery were analyzed.
Results:
Included were 24 patients (26 knees); there were 23 male and 1 female patients, with a mean age of 14.7 years. The mean follow-up period was 27.6 months. A total of 17 lesions were located in the medial femoral condyle and 9 in the lateral femoral condyle. The mean Tegner score was 7.0 preoperatively and 6.5 postoperatively, with no significant difference. The return-to-sports rate was 96.2% at the practice/training level and 84.6% at the preinjury level, with an average return time of 5.1 months and 9.6 months, respectively. In a subgroup analysis of knees that returned to preinjury level (n = 22) by lesion location, there was a significant difference between knees with lesions in the lateral femoral condyle (12.9 months) versus the medial femoral condyle (8.1 months) (P = .02). The rate of return to preinjury level after primary surgery was significantly higher than after revision surgery after failed drilling (P = .02).
Conclusion:
Return-to-sports rates and clinical outcomes were favorable after fixation with OAT in patients with knee OCD. A shorter time to return to sports was observed in knees with medial lesions compared with lateral lesions. Furthermore, the rate of return to sports at the preinjury level was significantly higher after primary surgery than after revision surgery after drilling.
Keywords
Osteochondritis dissecans (OCD) is a relatively rare disease in which the subchondral bone is affected, and the overlying articular cartilage is secondarily damaged at a later stage. 12 Although the etiology of OCD remains unknown, factors such as inflammation, ossification, and repetitive trauma have contributed to its development.22,45 Many procedures exist to treat OCD, but which is the most ideal is still unclear. Skeletal maturity and lesion stability, along with patient age, are key to determining appropriate treatment. 7 In general, nonsurgical treatment with activity restriction has been adopted for stable lesions in skeletally immature patients, yielding a healing rate of approximately 50%.3,8,9,41 Meanwhile, the healing rate for skeletally mature patients is reported to drop to around 30%.29,37 Indications for surgery include failure of nonoperative treatment, unstable lesions, presence of mechanical symptoms or loose bodies, and pain in daily life and sports activities. 40 For stable lesions in skeletally immature patients, retrograde or anterograde drilling is the sole indication for treatment.2,30 The most common surgical treatment for unstable OCD fragments is internal fixation,1,7 and recent literature suggests that the healing rate after internal fixation in skeletally immature patients ranges from 75% to 100%,1,26,44 whereas the rate in skeletally mature patients is lower, approximately 70% to 85%.4,23,43 The surgical options for irreparable lesions are on osteochondral autograft/allograft, autologous chondrocyte implantation, 25 or a combination thereof. 36 Treatment algorism in our practice follows the aforementioned treatment guidelines.
For unstable lesions, a number of internal fixation methods have been employed and their surgical outcomes have been reported. In the past, a variety of fixation devices have been used, including metal screws and biodegradable pins/rods. Fairly satisfactory results have been obtained, but some implant-related complications have been reported, such as migration or breakage of the implant, and foreign body reactions. Autogenous bone peg fixation is another option. However, there are concerns about loosening and fracture of the tibial donor site. Therefore, the optimum surgical treatment for unstable lesions remains controversial. 32
In our practice, internal fixation with osteochondral autologous transplantation (OAT) is the primary surgical option for unstable (and potentially salvageable) OCD lesions, with the intent of achieving both mechanical stability and promoting biological healing. The advantage of OAT is that the OCD lesion is covered with hyaline cartilage with a host-specific subchondral bone plug. 31 In 1999, Berlet et al 5 were the first to report the “biological internal fixation” method, which applies the OAT technique to the fixation of unstable OCD lesions. In this method, an autogenous osteochondral plug is harvested from the ipsilateral knee and transplanted into the OCD lesion for fixation. Since then, fixation with OAT for unstable OCD has been reported in several case series papers, with generally favorable results.5,15,26,34 However, few previous studies have examined the rate of return to sports after surgery.
The purpose of the current study was to retrospectively evaluate functional recovery (return to sports) and clinical outcomes after internal fixation with OAT for OCD of the knee. We hypothesized that OAT for OCD would have a high return to sports rate and good clinical outcomes.
Methods
Study Design and Participants
The protocol for this study received ethics committee approval. In this retrospective study, we identified patients who underwent OAT for OCD lesions during the study period between April 2010 and March 2020, and reviewed our experiences with this procedure. Regarding the inclusion criteria, we selected OCD lesions that underwent in situ fixation using OAT. Excluded criteria were patients with adult-onset OCD, those with unsalvageable fragments for which fragment resection and mosaicplasty were performed, those who were lost to follow-up for more than 1 year postoperatively, and those with incomplete clinical or radiographic data for analysis.
Initial Evaluation and Treatment Indications
All patients had been forced to restrict their daily and sports activities due to persistent pain and catching in the knee. A comprehensive clinical evaluation, including physical examination and clinical score acquisition, was performed for each patient upon their initial visit. Radiographs were taken in the anteroposterior, lateral, and standing weightbearing views, and magnetic resonance imaging (MRI) was performed. Radiographic evaluation was performed using the Brückl classification, 6 and MRI scan evaluation was performed using the Hefti classification. 16 According to Hefti classification, lesions were classified into 1 of the following 5 stages: stage 1, small change of signal without clear margins of fragment; stage 2, osteochondral fragment with clear margins, but without fluid between fragment and underlying bone; stage 3, fluid is visible partially between fragment and underlying bone; stage 4, fluid is completely surrounding the fragment, but the fragment is still in situ; or stage 5, fragment is completely detached and displaced (loose body). In arthroscopic and gross examinations, OCD lesion type was determined according to the International Cartilage Repair Society (ICRS) classification system, as follows: grade 1, stable with continuity; grade 2, partial discontinuity; grade 3, complete discontinuity; or grade 4, dislocated fragment, loose within the bed or empty defect.
Nonoperative treatment was initially employed for stable lesions, and surgical treatment was indicated for patients who failed nonoperative treatment or for unstable lesions. Surgical treatment was based on grading of the lesion. Drilling was performed on stable ICRS grade 1 lesions with a smooth and congruent surface. For unstable lesions, our primary option was internal fixation using OAT. We surmised that even a seemingly immobile lesion could exhibit mechanical instability due to subchondral avulsion. 45 Therefore, we employed fixation with OAT for both ICRS grade 2 and 3 lesions exhibiting partial or complete articular cartilage discontinuity. If the lesion was considered to be unsalvageable, we opted for a combination of fragment removal and mosaicplasty with OAT.
Surgical Technique and Postoperative Rehabilitation
All surgeries were performed by either of the 2 senior authors (S.Y., and H.N.) under general anesthesia. Initially, all patients underwent arthroscopy with an anterolateral and anteromedial portal to confirm the location and size of the OCD lesion and the ICRS OCD grade. An arthrotomy was then made, and the size and surface integrity of the lesion was evaluated on gross examination. For the OAT procedure, the recipient site of the OCD lesion was prepared to a depth of 15 mm using an appropriately sized recipient cutting tube (6, 8, or 10 mm; Arthrex, OATS; osteochondral autograft transfer system). Osteochondral grafts were harvested from the ipsilateral lateral femoral condyle. The harvest site was located at the anterodistal aspect of the articular facet in the nonweightbearing area. During extraction, extreme care was taken to avoid injury to the epiphyseal plate in patients with open physis. Subsequently, in situ fixation was performed by biological fixation using the autologous osteochondral plugs. The graft was inserted using a donor harvest device and gently pressed into the recipient site until it was flush with the surrounding cartilage. One or more plugs were used to cover at least 50% of the lesion surface. As a general rule, 1 plug in the center or 2 plugs to the periphery of the lesion were inserted until rigid stability could be achieved (Figure 1).

Serial images of a 16-year-old boy with OCD in the medial femoral condyle who underwent internal fixation using OAT. (A) Anteroposterior radiograph reveals a demarcated lesion in the MFC. (B) Sagittal T2-weighted MRI scan of the knee before surgery showing a bone fragment in situ completely surrounded by high-signal intensity line (Hefti classification stage 4). (C) Postoperative radiograph at 4 months, demonstrating progression of bony healing with apparently smooth joint congruity. (D) Intraoperative image showing partial cartilage fissuring at periphery of the OCD lesion in the MFC. (E) In situ fixation performed by biological fixation using 2 8-mm-diameter autogenous osteochondral plugs under arthrotomy. MFC, medial femoral condyle; MRI, magnetic resonance imaging; OAT, osteochondral autologous transplantation; OCD, osteochondritis dissecans.
Postoperative physical therapy began the next day with a series of exercises and isometric movements to strengthen the quadriceps. The knee was immobilized with a brace for 1 week, and full range of motion exercises were started at the second postoperative week as tolerated. Weightbearing was prohibited for the first 4 weeks postoperatively and progressed gradually to full weightbearing at 6 to 8 weeks after surgery. The patient was allowed to gradually return to sports at 4 months, taking into account bone union and muscle strength recovery.
Follow-up Evaluations
All patients were followed up regularly after surgery. Radiological examination was repeated every month until bony union was confirmed. The achievement of bone union was based on follow-up radiographic findings of integration at the interface between the OAT graft and the surrounding recipient bone. If there was uncertainty as to whether bony union had been achieved, computed tomography (CT) imaging was used to further evaluate healing. We opted not to utilize MRI for routine serial imaging examination because we felt the status of the bony union could be better confirmed by radiographs and CT images. In addition to the monthly evaluations for bony healing, clinical and radiological examinations were conducted regularly at 6, 9, and 12 months, and every 3 to 6 months for up to 2 years, followed by yearly assessment thereafter. Clinical results were also assessed during the follow-up period using the Lysholm score. 24
As for the evaluation of postoperative functional recovery, the type of sports activity, time to return to sport, and return rate were examined. Activity levels were determined using the Tegner activity scale, 38 and sports participation levels were assessed before and after surgery. Before surgery, most patients had to reduce their activity level due to knee pain. Therefore, the preoperative level was determined as the preinjury level, and the postoperative sports activity level was assessed every month after surgery. Currently, there is no standardized or widely accepted definition for when an athlete has officially returned to sport. Functional recovery in postoperative return to sports was classified into 2 levels: preinjury and participation. The preinjury level was defined as returning to the same level of sports activity as before the injury, and participation level was defined as returning to the level of practice or training. Clinical factors affecting the timing and rate of return to sports were also examined by comparing medial versus lateral femoral condylar lesions and primary versus secondary surgery after previous procedures such as drilling or meniscal surgery.
Clinical and radiological data collected during the preoperative and consecutive follow-up periods were obtained from the patient records. Patient data on demographics, functional recovery status, and postoperative complications were extracted from the chart review.
Statistical Analysis
Continuous data were reported as means and standard deviations, and categorical data were reported as frequencies and percentages. The paired t test was used to compare the pre- and postoperative Lysholm scores. The nonparametric Wilcoxon test was used to compare the Tegner scores before and after surgery. Return-to-sports evaluations were conducted with the unpaired t test or chi-square test. Statistical significance was set at P < .05.
Results
During the study period, OAT for OCD was performed in 34 patients (37 knees). Of these, 5 knees (including 2 adult-onset OCD knees) that underwent loose body removal or mosaicplasty and 6 knees in 5 patients who did not have more than 1 year follow-up data or for whom clinical/radiological data were not complete were excluded from the study. As a result, 24 patients (26 knees) who met the inclusion/exclusion criteria were included in the study.
Table 1 presents the demographic and clinical profiles of the study population. The mean follow-up period was 27.6 months (range, 12-120 months); 17 of the OCD lesions were located in the medial femoral condyle (MFC) and 9 on the lateral femoral condyle (LFC). There were 11 knees classified as Hefti stage 3 and 15 knees classified as Hefti stage 4; 12 knees were classified as having ICRS grade 2 OCD whereas 14 knees had ICRS grade 3 OCD. Regarding previous surgeries, 7 knees (1 medial and 6 lateral condyle lesions) underwent drilling as a primary procedure for stable OCD, while saucerization with or without repair of the lateral discoid meniscus was performed in 6 knees.
Demographic and Clinical Profile of the Study Population (N = 24 Patients; 26 Knees) a

Data are presented as mean ± SD (range) or No. of knees unless otherwise indicated. ICRS, International Cartilage Repair Society; LFC, lateral femoral condyle; MFC, medial femoral condyle; MRI, magnetic resonance imaging; OAT, osteochondral autologous transplantation; OCD, osteochondritis dissecans.
Table 2 shows the outcomes at 1 year postoperatively. The Lysholm score showed significant improvement from 70.0 preoperatively to 96.0 postoperatively (P < .01). Regarding return to participation and preinjury level, 96.2% of patients were able to return to participation, which took an average of 5.1 months, and 84.6% returned to preinjury level, which took an average of 9.6 months. The Tegner score decreased from 7.0 before injury to 6.5 after surgery, with no significant difference. Bony union was achieved within 1 year in all knees.
Return-to-Sports Data and Outcome Scores at 1 Year Postoperatively (n = 26 Knees) a

Data are presented as mean ± SD (range) or No. of knees (%). Preop, preoperative; Postop, postoperative.
Defined as returning to practice or training.
Statistically significant difference between preoperative and postoperative scores (P < .01).
Table 3 shows the rates and times to return to sports according to lesion site. When comparing MFC and LFC lesions, there was no significant difference in the Lysholm score, return to participation, or return to preinjury level rates. However, the time to return to preinjury level was significantly longer for those with LFC lesions versus MFC lesions (12.9 vs 8.1 months, respectively; P = .02).
Return-to-Sports Data and Outcome Scores According to Lesion Site a

Data are presented as mean (range) or percentage. Boldface P value indicates statistically significant difference between groups (P < .05). ICRS; International Cartilage Repair Society; LFC; lateral femoral condyle; MFC; medial femoral condyle; ns, not significant.
Defined as returning to practice or training.
Table 4 describes the return to sports rates after the primary and secondary surgeries. There were no significant differences in return to participation rates or Lysholm score between the 2 groups, but the rate of return to preinjury sports was significantly lower after drilling from the secondary surgery (57% vs 95% after primary surgery; P = .02).
Return-to-Sports Data and Outcome Scores After Secondary and Primary Surgeries a
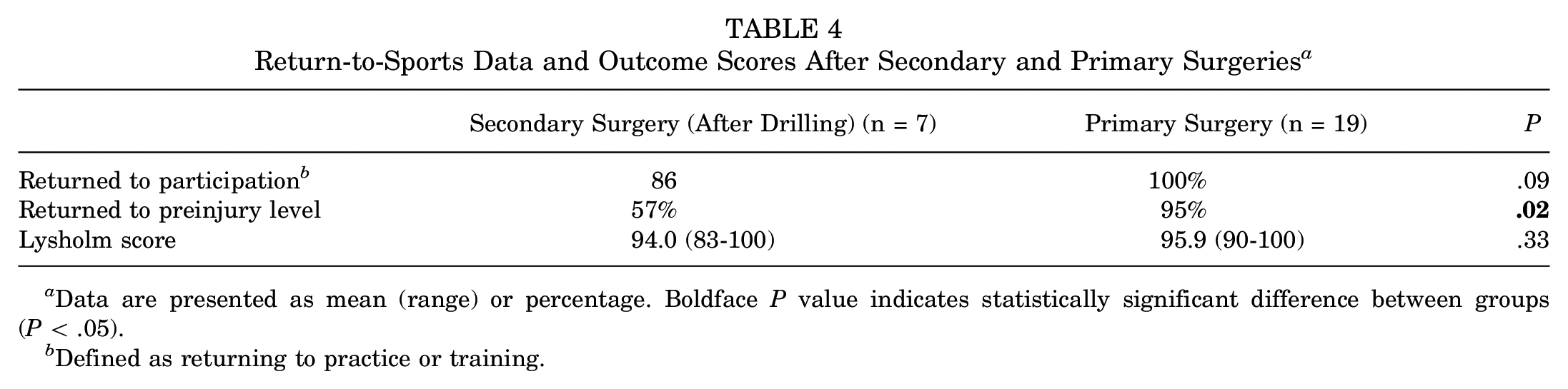
Data are presented as mean (range) or percentage. Boldface P value indicates statistically significant difference between groups (P < .05).
Defined as returning to practice or training.
Of the 24 patients, 16 had follow-up results of longer than 2 years. At the final follow-up, which ranged from 24 to 120 months, the Lysholm and Tegner scores averaged 96.8 ± 4.4 (range, 83-100) and 6.1 ± 1.3 (range, 3-7), respectively, indicating that the improvement in clinical outcomes was maintained at mid- to long-term follow-up. No donor site morbidity, complications, or infections related to the index surgery were observed in any of the knees during the entirety of the study. Only 1 patient underwent reoperation (drilling) 4 years after surgery.
Discussion
The principal findings of this study showed that fixation with OAT for knee OCD lesions resulted in largely acceptable outcomes and satisfactory functional recovery. As for clinical factors affecting return to sports, a shorter time to return was observed in knees with MFC lesions compared with LFC lesions. In addition, the rate of return to preinjury level was significantly higher after primary surgery than after revision surgery after drilling.
Drilling is a generally accepted surgical option for stable juvenile OCD lesions, whereas internal fixation (with or without bone grafting) is suitable for unstable lesions. For unstable lesions requiring fixation, various fixation methods have been reported, including variable pitch screws, partially threaded cannulated screws, bioabsorbable screws, pins, and bone sticks or bone pegs.17,21,28,39 Although good clinical outcomes have been reported for the use of the implants for fixation, various complications have also been reported, including cartilage lesions, osteonecrosis, synovitis, and implant failure due to loose body formation.14,19,26,35,42 In addition, these procedures have inherent shortcomings because they do not promote biological healing enhancement. Bone peg/stick fixation may eradicate the implant-related issues, but potential complications such as loosening and fracture at the tibial donor site remain a concern.10,14
The OAT technique called “in situ fixation,” in which the osteochondral fragment is fixed with autogenous osteochondral plugs, has been practiced as an alternative surgical option for unstable OCD lesions.5,13,18,20,33 Studies have reported good-to-excellent clinical results in 95% and 91% of patients with a mean follow-up of 3.4 and 4.5 years, respectively.26,27 Fixation with an osteochondral plug allows for firm stability associated with bone-to-bone contact and subsequent rapid healing at the interface. Therefore, both mechanical and biological enhancement for tissue healing can be attained. Another advantage of this method is that the reconstructed articular surface is smooth and congruent. This is because the original articular surface of the OCD fragment is restored in situ with the original thickness of the articular cartilage. Our results showed that, although the follow-up period was short, bone union was achieved in all cases, and the Lysholm score had also significantly improved.
Yonetani et al 45 conducted a histological evaluation of cylindrical samples obtained from stable juvenile OCD lesions and showed that a separation was present at the subchondral layer even in seemingly stable ICRS grade 2 lesions. Therefore, even for ICRS grade 2 lesions in this study, fixation with OAT was indicated, considering the possibility of underlying instability. Furthermore, in fixation using OAT, pathological tissue consisting of fibrous tissue and sclerotic bone are removed, and a substantial amount of healthy cancellous bone is implanted as autogenous bone grafting.
Return to Sports
Examination of the evidence for athlete outcomes reveals just how little is known about this disease. Athletes have different needs for treatment compared with the general public. Although many studies have focused on sports-related outcomes after surgical treatment of knee OCD, few have specifically examined return to sports rates. Sasaki et al 34 reported that all 12 patients who underwent OAT for juvenile OCD returned to their previous level of sports activity at an average of 5.7 months after surgery. However, previous reports have had mixed results and the definition of return to sports remains ambiguous, making it difficult to determine a clinical standard. The finding of this study was that this surgical treatment option allowed for adequate return to sports rates although return to sports rates decreased slightly when a return to sports was defined as a return to preinjury level. According to the results of our study, only 1 case was unable to return to participation, and the recovery rate to preinjury level was 84.6%.
The rate and period of return to sports were influenced significantly by lesion location. A shorter return to sports time was observed in lesions of the MFC compared with LFC lesions. This was also supported by Webb et al, 42 who analyzed healing rates for internal fixation of unstable OCD lesions in skeletally immature patients, finding that all 5 failures occurred in the 11 knees with LFC lesions. This result may be related to the discoid lateral meniscus. It has been reported that 11.3% to 14.5% of lateral discoid menisci are associated with lateral condylar OCD, while lateral discoid menisci are present in 89% of the lateral OCD knees. 11
Another factor affecting functional recovery identified in this study was a history of surgery on the same knee. Of the 26 knees, included in this study, 7 previously underwent surgical drilling and 6 had a history of discoid meniscal repair. When the fixation with OAT was conducted after failed drilling, the return to preinjury level rate was significantly lower than that after the primary OAT procedure. Failure to heal after drilling was more common in lateral lesions, with 6 cases in lateral compared with 1 case in medial lesions. The higher rate of drilling of lateral lesions may have confounded a fair comparative analysis between MFC and LFC lesions. The small sample size in this study precluded further analysis regarding how each of these 2 factors (lesion location and revision surgery) influenced postoperative functional recovery. Repeat surgeries may have caused prolonged pain and muscle weakness, which may have delayed the patient’s return to sports. In the future, comparative analysis of functional outcomes between drilling and other surgical procedures should be considered.
Return to sports was evaluated as being able to return to the same sport as before the injury, so actual athletic performance was not evaluated. The most common cause for not returning to sports was residual pain, but, in some cases, the patient had changed sports. The involvement of social factors must also be considered, since this includes cases in which the patient changes sports due to advancement in higher education or employment, regardless of competitive level.
Limitations
There were some limitations included in this study. First, the study was descriptive and the results were not compared with other methods. Second, the follow-up period (minimum of 1 year) was too short, and the progression of osteoarthritis would be higher if the follow-up period were longer. Moreover, long-term observation is necessary to monitor for unexpected long-term complications, especially lesions at the harvest site. Third, the study involved a small number of patients. In the analysis of the present study results, 2 factors (lateral lesions and revision surgery) were identified as potential factors affecting postoperative functional recovery; however, the sample size was too small to run a multiple regression for each confounder. Consequently, it was not possible to determine whether one, or both, might be the independent factor related to poorer outcomes. In addition, the preponderance of male subjects was a drawback that precluded fair statistical analysis of prognostic factors. Fourth, the level of sports activity is varied among the study subjects, making it difficult to make a fair assessment of the surgical effect on postoperative functional recovery.
Conclusion
Return-to-sports rates and clinical outcomes were favorable after fixation with OAT in patients with OCD of the knee who wished to continue their sports activities, achieving 96.2% and 84.6% return to sports rates at participation and preinjury levels. As for clinical factors influencing functional recovery, a shorter return to sports time was noted in patients with medial lesions compared with those with lateral lesions. Furthermore, the rate of return to the preinjury sports level was significantly higher after primary surgery than after revision surgery after drilling.
Footnotes
Acknowledgements
The authors acknowledge Nick Pollifrone for his assistance in editing the English of this article.
Final revision submitted May 20, 2024; accepted June 13, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hyogo Medical University (reference No. 3760).