
Abstract
Background:
A paucity of data exists to guide surgical management of the medial collateral ligament (MCL). High-grade MCL injuries are often treated with surgical repair or reconstruction; however, guidelines for choosing one or the other technique remain unclear.
Purpose:
To systematically review the literature to determine whether repair versus reconstruction of the MCL in multiligament knee injuries results in improved outcomes.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines was performed between January 1980 and January 2024. The initial search yielded 85 studies. Exclusion criteria included <2 years of follow-up, technical/case reports, articular fractures, and undifferentiated multiligament results. Extracted data included patient characteristics, ligaments injured, chronicity of injury, incidence of failure, arthrofibrosis, patient-reported outcome scores, and stress radiographs. Failure was included as reported by studies and included clinical failure (graft laxity), failure of the repair or reconstruction, or the need for a lysis of adhesions or manipulation under anesthesia. Statistical analysis included unpaired t tests and chi-square goodness-of-fit tests.
Results:
In total, 30 studies were included in the final analysis (458 repairs, 590 reconstructions). The mean patient age for the repair group was 33.1 years (SD, 5.11 years) with a mean follow-up time of 4.2 years (SD, 2.59 years) and the mean patient age for the reconstruction group was 33.4 years (SD, 4.40 years) with a mean follow-up time of 3.1 years (SD, 1.41 years). There was no significant difference found between the reconstruction and repair groups of the MCL for the Lysholm, subjective International Knee Documentation Committee, Tegner scores, and stress radiographs (P > .05). Arthrofibrosis rates for MCL reconstruction (5.4%) were determined to be significantly less than those within the repair group (11.6%) (P < .001). Failure rates for MCL reconstruction (2.9%) were determined to be significantly less when compared with the MCL repair group (5.7%) (P = .024). Anterior cruciate ligament (ACL) failure rates for MCL reconstruction (0.2%) were determined to be significantly less than those within the repair group (2.3%) (P = .002).
Conclusion:
This systematic review showed that MCL reconstructions demonstrated decreased postoperative arthrofibrosis compared with MCL repairs across all studies. Studies reporting on failures reported decreased clinical failures and ACL graft failures in the setting of concomitant ACL and MCL reconstructions compared with MCL repairs. Future randomized controlled studies are needed to further determine the best surgical technique for patients with multiligament knee injuries.
Injuries to the medial collateral ligament (MCL) are the most frequent ligament knee injuries.30,38 In the United States, the incidence of injuries to the superficial MCL (sMCL) and other medial knee stabilizers (the deep MCL and posterior oblique ligament) has been reported to be 0.24 per 1000 persons annually. 5 Moreover, in a recent epidemiological study of 6343 patients with 7769 sports-related knee injuries, the incidence of MCL tears was 7.9%. 36 The mechanism of injury typically involves valgus loading of the knee, with or without a tibial external rotation force.30,35,37,46 Nearly 78% of grade 3 MCL tears occur as part of a multiligament knee injury, of which, approximately 95% have a concomitant anterior cruciate ligament (ACL) tear.14,16 In the setting of ACL reconstruction (ACLR), preoperative medial-sided knee instability is a risk factor for ACLR graft failure, highlighting the importance of proper repair or reconstruction of the MCL. 1
It is generally accepted that grade 1 and 2 MCL tears, as well as select cases of isolated grade 3 tears, can be treated nonoperatively with bracing and early functional rehabilitation.7,13,30,37,57 However, the management of grade 3 MCL tears with persistent valgus instability remains controversial. Surgical intervention may be indicated either when patients do not respond to initial nonoperative measures or when they have chronic valgus instability or in the face of a multiligament knee injury.12,30,57
Reconstruction and primary operative repair of the MCL have been described, but there remains a paucity of outcome data comparing these treatments to help guide surgical decision-making.6,57 Notably, a systematic review by Kovachevich et al 26 found that both MCL repair and reconstruction produced satisfactory results in the setting of multiligament injuries. However, there is still some concern of postoperative arthrofibrosis after both MCL reconstruction and repair. 41 The heterogeneity and retrospective quality of the data available prevented any formal comparison or meta-analysis. 26
Our aim was to determine whether sufficient evidence has become available regarding MCL repair versus reconstruction. Therefore, the purpose of this study was to systematically review the literature to determine whether repair or reconstruction of the MCL results in improved outcomes. Our null hypothesis was that there would be no significant difference in failure rate, arthrofibrosis, and patient-reported outcomes between patients who underwent MCL reconstruction versus MCL repair in multiligament knee injuries.
Methods
Article Identification and Selection
This study was conducted using the 2009 Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement guidelines and registered on the PROSPERO international prospective register of systematic reviews. Searches were performed of the MEDLINE, Embase, Cochrane, and PubMed databases between January 1980 and January 2024; article identification was performed in January 2024. 40 The following search terms were used: medial collateral ligament, repair, reconstruction, superficial medial collateral ligament, and tibial collateral ligament. The search strategy utilized was as follows: (((Medial collateral ligament) AND (repair)) OR ((medial collateral ligament) AND (reconstruction)) OR (superficial medial collateral ligament) OR (tibial collateral ligament)).
All studies from each database were uploaded to EndNote Reference Manager for duplicate article deletion. 40 Articles from EndNote were then transferred to Rayyan QCRI (Qatar Computer Research Institute, Hamad Bin Khalifa University, Qatar) for further evaluation. 44 Four authors (E.R.F., L.V.T., K.L.F., and G.D.S.) reviewed all abstracts for inclusion criteria. Inclusion criteria consisted of articles that published results on patients (1) ≥15 years of age, (2) with MCL ligament injuries requiring surgical management (repair or reconstruction) with or without an ACL injury requiring surgical management, (3) having at least 1 subjective outcome score with at least 2 years of follow-up (Knee injury and Osteoarthritis Outcome Score, Lysholm score, International Knee Documentation Committee [IKDC] score, and Tegner score), (4) with ≥1 forms of objective outcome measurement (including IKDC objective scores, valgus stress examination, or valgus stress radiographs), and (5) with level of evidence 1 to 4. Exclusion criteria included patients <15 years of age, <10 patients in the study, technique papers, case reports, patients with fractures associated with the MCL injury, studies that only treated the MCL nonoperatively, studies with revision cases, studies reporting on MCL injuries with posterior cruciate ligament or posterolateral corner injuries (MCL and ACL were included), and studies addressing multiligament injuries to the knee that did not identify the MCL as a separate cohort. It should be noted that articles included both acute (<6 weeks) and chronic (>6 weeks) ligament injuries. Four reviewers (E.R.F., L.V.T., K.L.F., and G.D.S.) examined all full texts of abstracts meeting the inclusion criteria. Any disagreement in full texts to include in the analysis was decided by the senior author (R.F.L.). Furthermore, all systematic reviews found in the database were examined for additional relevant studies that may have been missed.
Primary repairs were defined as suture repairs of the native MCL, while reconstructions were defined as any reconstruction or augmentation with an auto- or allograft. For our purposes, sMCL augmentations with autografts or allografts were considered reconstruction procedures.
Data Collection
Patient characteristics, level of evidence, chronicity of injury, follow-up time, available patient-reported subjective and objective scores, reports of failures and development of arthrofibrosis, reconstruction techniques, and concomitant ACL graft failure were collected from each study. Arthrofibrosis was included as reported by the studies, or if not directly discussed, it was correlated with reports of decreased postoperative range of motion (flexion deficits ≥10° and extension deficits ≥5°), the need for a lysis of adhesions (LOA), the need for manipulation under anesthesia (MUA), or formation of scar tissue leading to pain or limitations in movement within the individual studies. Reports of failure were included as reported by studies and included clinical failure of the MCL repair or reconstruction (significant laxity still present after surgery), failure of the repair or reconstruction (graft or fixation failure), and the need for an LOA or MUA. Failure of the ACL was defined as clinical failure (significant postoperative laxity), graft failure, or graft fixation failure. Numeric values including age, subjective patient-reported outcomes, and stress radiographs (with preoperative and postoperative values of side-to-side differences), as available, are reported as a mean.
Statistical Analysis
After data extraction, RStudio (RStudio, PBC) 48 was utilized to perform a t test and to determine whether there was a statistically significant difference (P < .05) for Lysholm scores, IKDC subjective scores, Tegner scores, and stress radiograph means between the repair and reconstruction groups. Failures were defined by the author of each study. A chi-square goodness-of-fit test was conducted using RStudio to determine if there was a significant difference (P < .05) in arthrofibrosis rates and failure rates between the repair and reconstruction groups.
Studies in the analysis considered selection bias, small sample sizes, and lack of comparative controls. In many cases, it was not possible to provide controls because of the heterogeneous nature of the multiligament injuries, reconstruction techniques, and surgical choices made based on concomitant injuries. The authors ensured that the studies examined considered such limitations to minimize bias and recognize the constraints presented by the nature of the data.
Risk of Bias Assessment
The Methodological Index for Non-Randomized Studies (MINORS) was used to assess the included studies for risk of bias. This index uses 8 questions for noncomparative studies and 12 questions for comparative studies. Each category is given a score from 0 to 2. A perfect score is 16 for noncomparative studies and 24 for comparative studies. All studies describing both MCL reconstruction and repair were graded with the comparative study grading, and all other studies were graded with the noncomparative grading.
Results
After completing a literature search and removing duplicate articles, 4403 entries matched the search criteria. The 4403 entries were reduced to 85 articles after abstract review and to 42 after initial full-text review. A total of 30 articles were included in the final analysis (Figure 1). ‖
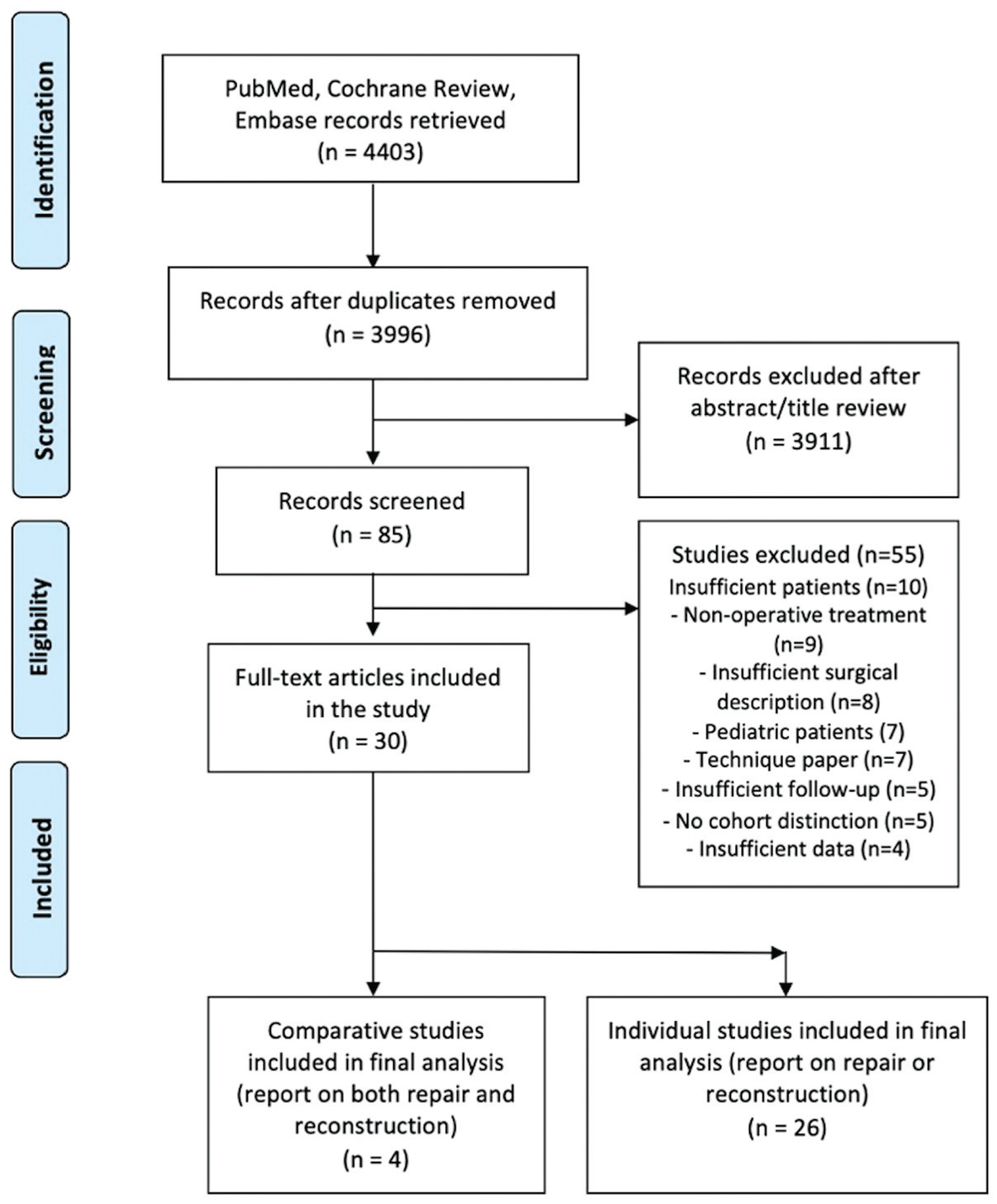
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart outlining the process of screening and selection.
The 30 studies included 1048 total patients, 458 MCL repairs, and 590 MCL reconstructions. All but 91 MCL injuries (8.7%) in this cohort were part of multiligament injuries. For the studies in which chronicity was mentioned, interventions were performed in the acute phase (<6 weeks) for 406 patients (50.4%) and in the chronic phase (>6 weeks) for 400 patients (49.6%). The mean patient age was 33.3 years (SD, 5.11 years) in the repair cohort and 33.4 years (SD, 4.40 years) in the reconstruction cohort. The mean follow-up time was 4.2 years (SD, 2.59 years) in the repair cohort and 3.1 years (SD, 1.41 years) in the revision cohort (minimum, 2 years). There was a significant difference in acute and chronic cases per group, with the repair group having significantly more acute cases (306/406; 75.4%) and the reconstruction group having significantly more chronic cases (334/400; 83.5%) (P < .001). The number of procedures performed, mean age, chronicity, type of reconstruction, and mean follow-up time for each specific procedure can be found in Table 1.
Characteristics of Patients With MCL Repair and Reconstruction a

Data are reported mean (SD) or n (%) unless otherwise indicated. MCL, medial collateral ligament.
Outcomes including stress radiographs, patient-reported outcomes, arthrofibrosis, failure, and ACLR from each individual study were documented and are reported in Table 2. The overall outcomes comparing MCL repair with MCL reconstruction are reported in Table 3. There was no significant difference in postoperative Lysholm scores between the 13 MCL repair studies, with a mean score of 91.9 (SD, 4.24), and the 10 MCL reconstruction studies, with a mean score of 86.8 (SD, 10.46) (P = .122). There was no significant difference in postoperative IKDC scores between the 7 MCL repair studies, with a mean score of 83.5 (SD, 5.88), and the 10 MCL reconstruction studies, with a mean score of 78.6 (SD, 11.29) (P = .303). There was no significant difference between the postoperative Tegner scores between the 5 MCL repair studies, with a mean score of 5.6 (SD, 0.89), and the 6 MCL reconstruction studies, with a mean score of 5.3 (SD, 1.07) (P = .602).
Summary of Outcome Data for Each Included Study a
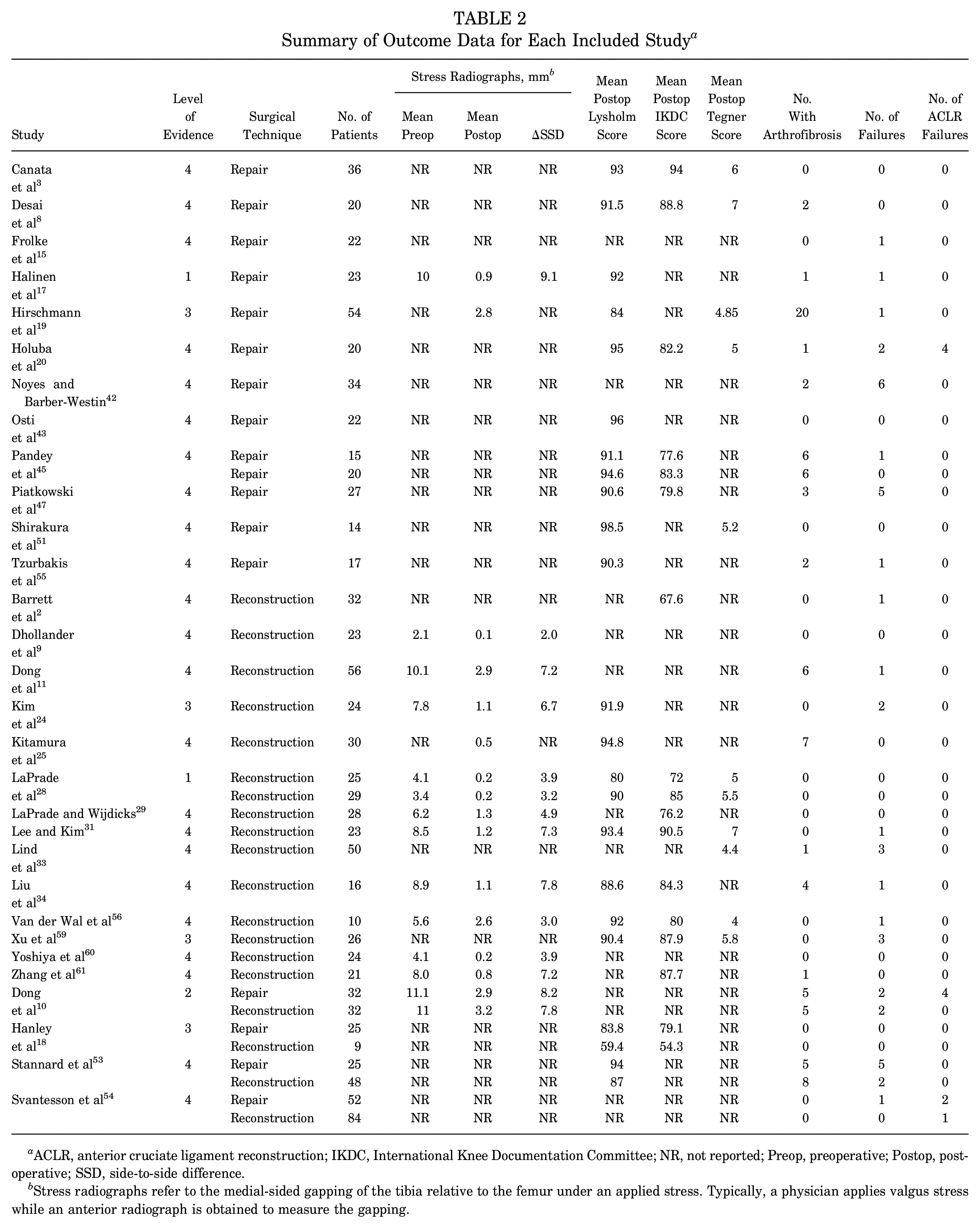
ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee; NR, not reported; Preop, preoperative; Postop, postoperative; SSD, side-to-side difference.
Stress radiographs refer to the medial-sided gapping of the tibia relative to the femur under an applied stress. Typically, a physician applies valgus stress while an anterior radiograph is obtained to measure the gapping.
Summary of Results for MCL Repair Versus Reconstruction a
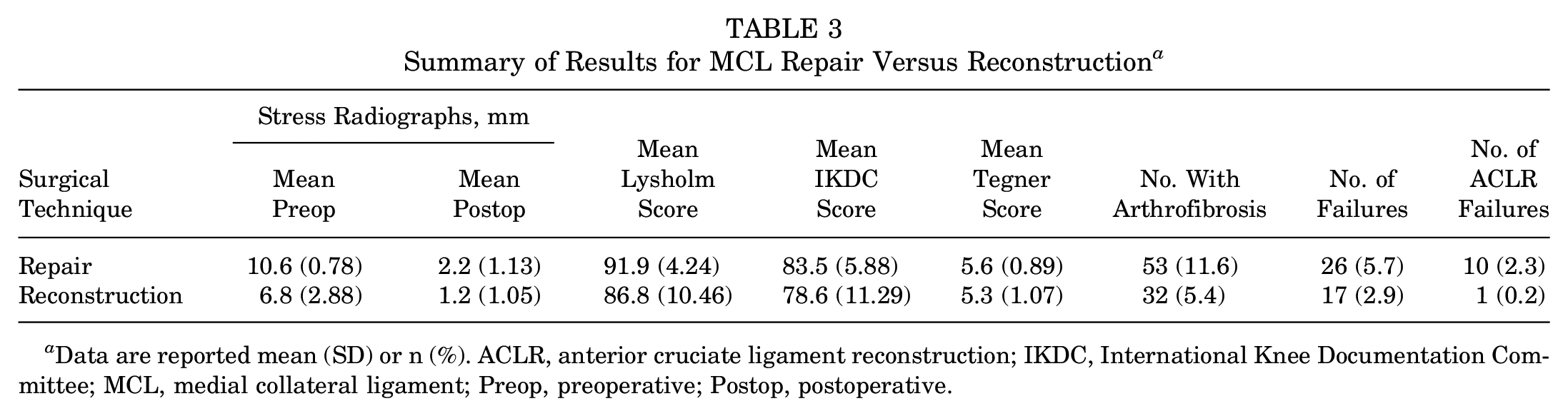
Data are reported mean (SD) or n (%). ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee; MCL, medial collateral ligament; Preop, preoperative; Postop, postoperative.
For postoperative arthrofibrosis (decreased range of motion or stiffness requiring LOA or MUA, flexion deficits ≥10°, and extension deficits ≥5°), 53 of 458 repairs (11.6%) resulted in arthrofibrosis and 32 of 590 reconstructions (5.4%) resulted in arthrofibrosis. Arthrofibrosis rates for MCL reconstruction were determined to be significantly less than the repair group (χ2 = 13.078; P < .001). For failures, 26 of 458 repairs (5.7%) resulted in failures and 21 of 590 reconstructions (2.9%) resulted in failures. Failure rates for MCL reconstruction were determined to be significantly less than the repair group (χ2 = 5.121; P = .024). For ACLR failures, 10 of 435 repairs (2.3%) resulted in ACL failure and 1 of 522 (0.2%) reconstructions resulted in ACL failure. ACL failure rates for MCL reconstruction were determined to be significantly less than the repair group (χ2 = 9.273; P = .002).
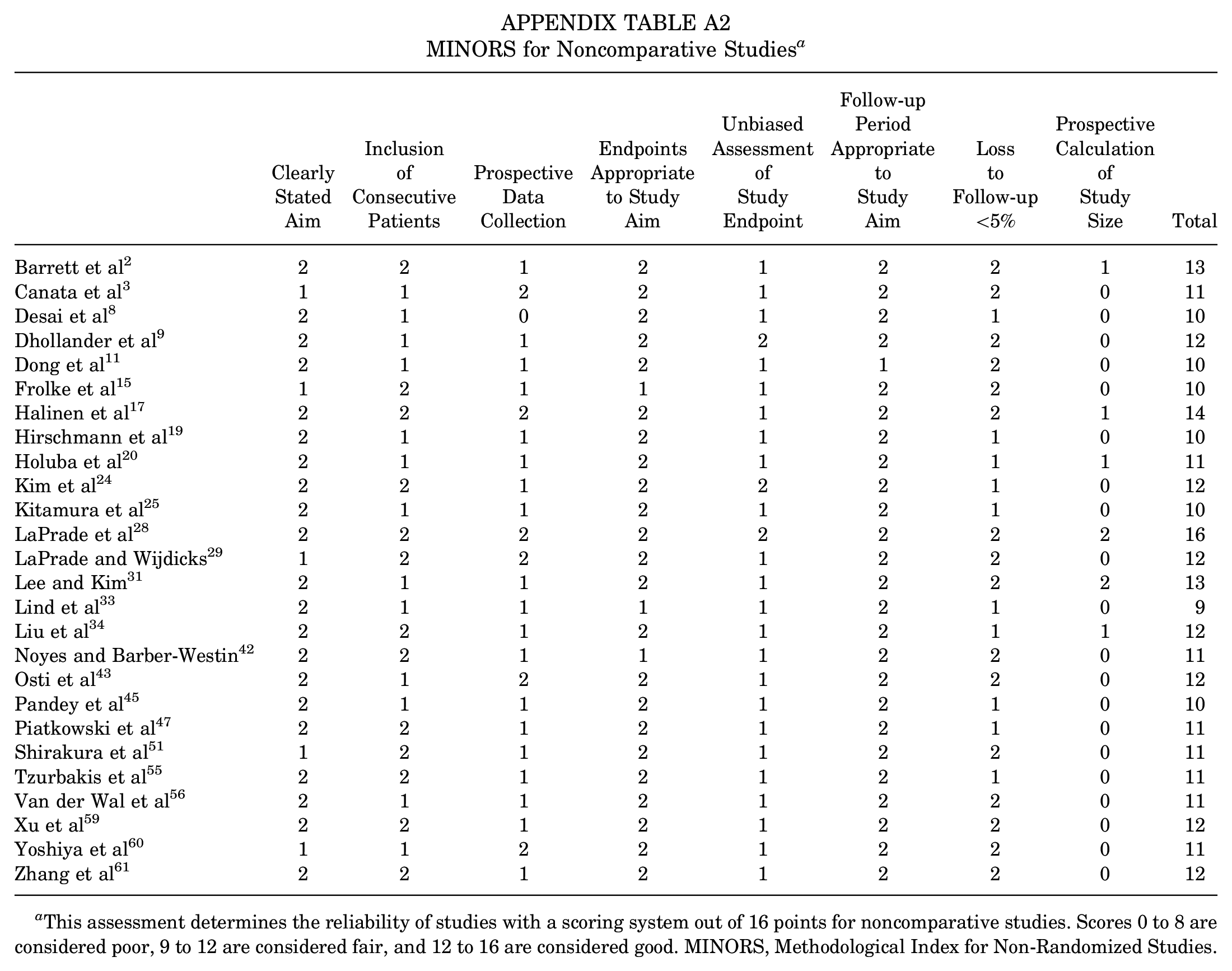
Risk of bias assessment using the MINORS criteria is listed in Appendix Tables A1 and A2. A mean score of 18.5 of 24 (range, 15-21) was reported for the comparative studies and 11.4 of 16 (range, 9-16) for the noncomparative studies.
Discussion
The most important finding of this study was that patients with direct repair of the MCL demonstrated significantly higher rates of arthrofibrosis (11.6% vs 5.4%; P < .001) and concomitant ACL graft failure in multiligament cases (2.3% vs 0.2%; P = .003) postoperatively than patients with a reconstruction of the MCL. These findings were found to be significant across 30 studies, which reported outcomes for MCL repairs, MCL reconstructions, or both. Arthrofibrosis has been reported to be a significant source of morbidity after MCL surgical treatment, and our results may provide support for the notion that MCL reconstruction leads to a significantly lower rate of stiffness and range of motion loss.22,30
This study found that the combined results between all studies evaluated reported an increased rate of arthrofibrosis in patients undergoing MCL repair compared with MCL reconstruction, and almost all patients were treated for multiligament knee injuries. Conventional wisdom has long held that the MCL has sufficient healing capacity to mend well in most circumstances with nonoperative treatment without the need for reconstruction or repair.37,38,57 When surgical intervention of the MCL is required, complications including arthrofibrosis and surgical site morbidity have been suggested for both repairs and reconstructions.12,38 However, 78% of grade 3 MCL tears occur as part of a multiligament knee injury, and delaying surgery to allow the MCL to heal on its own is not always the pragmatic choice. 14 Various studies have reported improved clinical and functional outcomes for acute surgery of multiligament knee injuries compared with delayed surgery.32,39,49 A systematic review by Sheth et al 50 reported that patients with acute surgery for multiligament knee injuries reported significantly increased Lysholm scores and Meyers ratings, with no difference in patients undergoing an MUA compared with delayed cases when an early range of motion protocol was used. Additionally, a recent study by Shultz et al 52 reported no significant difference between nonoperative and operative treatment of MCL injuries for patient-reported outcomes, range of motion, or quadriceps strength. Together, these findings suggest that performing an acute MCL reconstruction in place of an MCL repair, including in the case of a multiligament knee injury, paired with a rehabilitation protocol emphasizing early motion, may help prevent arthrofibrosis and improve patient-reported outcomes.
Another finding from this study was that when the ACL is reconstructed along with an MCL repair or reconstruction, the ACL graft is significantly more likely to fail when performed concomitantly with an MCL repair versus an MCL reconstruction. Studies by Dong et al 10 and Svantesson et al 54 had similar findings with the MCL repair group, reporting more ACL graft failures than the MCL reconstruction group. This finding is especially important because approximately 78% of all MCL tears include other ligament tears, and 95% of these cases are reported to have a concomitant ACL tear. 16 Clinically, this highlights the importance of analyzing ACL and MCL tears concomitantly as MCL injuries are typically not isolated. Residual valgus laxity has been reported as a potential risk factor for ACL failure, which could suggest that MCL repair does not restore valgus stability as well as an MCL reconstruction. 21 A biomechanical study by Wijdicks et al 58 compared anatomic augmented repairs (functionally a reconstruction, using a semitendinosus autograft left attached distally) and anatomic reconstruction (semitendinosus graft with distal and proximal tunnels) for MCL tears and reported no significant differences between the 2 states; additionally, the study reported that both techniques improve knee stability and prevent >2 mm of medial opening compared with the native state. These findings suggest that in the case of a grade 3 MCL tear, an MCL reconstruction may be better to properly restore the knee biomechanics, prevent residual valgus laxity, and protect the knee from concomitant ACL graft failure.
Limitations
This study is not without potential limitations, which include the heterogeneity of multiligament injury comparisons, diagnostic tests used in diagnosis and postoperative evaluation, surgical methods, and rehabilitation techniques used. For example, Dong et al 10 used a triangular medial reconstruction rather than anatomic reconstructions; thus, results may or may not be directly comparable to anatomic reconstructions. Some authors used different methods of repair for distal MCL avulsions, including the “MCL Stener-like lesion,” versus midsubstance tears in the acute setting.8,55 Additionally, there was no differentiation across studies regarding whether a patient had a full posteromedial corner injury (MCL plus posterior oblique ligament) or just an MCL tear. Also, for valgus stress examinations, different types of measurements were utilized across the studies, which can be inaccurate and make comparisons between stress varues across studies difficult. Another limitation was that the majority of MCL tears occurred as combined, multiligament injuries rather than as isolated MCL tears. Furthermore, we were not able to perform an analysis on the effect of acute versus chronic injuries because most MCL repairs were in the acute phase and most MCL reconstructions were in the chronic phase.
Conclusion
This systematic review showed that MCL reconstructions demonstrated decreased postoperative arthrofibrosis compared with MCL repairs across all studies. Studies reporting on failures indicated decreased clinical failures and ACL graft failures in the setting of concomitant ACL and MCL reconstructions compared with MCL repairs. Future randomized controlled studies are needed to further determine the best surgical technique for patients with multiligament knee injuries.
Footnotes
Appendix
MINORS for Noncomparative Studies a
| Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Data Collection | Endpoints Appropriate to Study Aim | Unbiased Assessment of Study Endpoint | Follow-up Period Appropriate to Study Aim | Loss to Follow-up <5% | Prospective Calculation of Study Size | Total | |
|---|---|---|---|---|---|---|---|---|---|
| Barrett et al 2 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 1 | 13 |
| Canata et al 3 | 1 | 1 | 2 | 2 | 1 | 2 | 2 | 0 | 11 |
| Desai et al 8 | 2 | 1 | 0 | 2 | 1 | 2 | 1 | 0 | 10 |
| Dhollander et al 9 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 0 | 12 |
| Dong et al 11 | 2 | 1 | 1 | 2 | 1 | 1 | 2 | 0 | 10 |
| Frolke et al 15 | 1 | 2 | 1 | 1 | 1 | 2 | 2 | 0 | 10 |
| Halinen et al 17 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 14 |
| Hirschmann et al 19 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 0 | 10 |
| Holuba et al 20 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 1 | 11 |
| Kim et al 24 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 0 | 12 |
| Kitamura et al 25 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 0 | 10 |
| LaPrade et al 28 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 16 |
| LaPrade and Wijdicks 29 | 1 | 2 | 2 | 2 | 1 | 2 | 2 | 0 | 12 |
| Lee and Kim 31 | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 13 |
| Lind et al 33 | 2 | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 9 |
| Liu et al 34 | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 1 | 12 |
| Noyes and Barber-Westin 42 | 2 | 2 | 1 | 1 | 1 | 2 | 2 | 0 | 11 |
| Osti et al 43 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 0 | 12 |
| Pandey et al 45 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 0 | 10 |
| Piatkowski et al 47 | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 0 | 11 |
| Shirakura et al 51 | 1 | 2 | 1 | 2 | 1 | 2 | 2 | 0 | 11 |
| Tzurbakis et al 55 | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 0 | 11 |
| Van der Wal et al 56 | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 0 | 11 |
| Xu et al 59 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 0 | 12 |
| Yoshiya et al 60 | 1 | 1 | 2 | 2 | 1 | 2 | 2 | 0 | 11 |
| Zhang et al 61 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 0 | 12 |
This assessment determines the reliability of studies with a scoring system out of 16 points for noncomparative studies. Scores 0 to 8 are considered poor, 9 to 12 are considered fair, and 12 to 16 are considered good. MINORS, Methodological Index for Non-Randomized Studies.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.B.C. has received education payments from Gemini Mountain Medical and Arthrex and hospitality payments from Smith+Nephew. R.F.L. has received royalties from Arthrex and Smith+Nephew, education payments from Foundation Medical, nonconsulting fees from Smith+Nephew, and consulting fees from Smith+Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Final revision submitted June 9, 2024; accepted June 18, 2024.