
Abstract
Background:
Management approaches and surgical techniques for patellofemoral instability (PFI) continue to lack clear clinical guidelines and indications. Medial patellofemoral ligament reconstruction (MPFLR) is the most frequently used surgical procedure; however, variation in technique remains significant, particularly in skeletally immature patients.
Purpose/Hypothesis:
The purpose of this study was to examine variations in MPFLR technique in skeletally immature patients as represented by 20 orthopaedic surgeons with different experience levels and specialty training backgrounds who perform a high volume of PFI surgery in this age group. The hypothesis was that variation would be high.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Operative records of skeletally immature patients who underwent a primary, single-stage MPFLR between 2016 and 2021 within the JUPITER (JUstifying Patellar Instability Treatment by Results) cohort, a multicenter prospective study involving 13 tertiary care academic centers, were analyzed, including demographic information, injury data, and surgical technique details.
Results:
Of the 305 surgical PFI cases in skeletally immature patients, 245 knees (46% female, 54% male; mean age, 13.6 ± 1.8 years; range, 5.1-19.0 years) met inclusion criteria. High variation was identified in MPFLR tendon graft type (59% allograft, 41% autograft), patellar fixation (62% suture anchor, 32% patellar bone bridge/tunnel), and femoral fixation (76% interference/tenodesis screw, 23% suture anchor). All cases (100%) used fluoroscopic guidance and physeal-sparing principles, with femoral implant placement distal to the distal femoral physis. High variation was seen in adjunctive procedures, including lateral retinacular release or lengthening (22%), osteochondral fracture treatment (13% overall; 53% of which underwent loose body removal, 44% fixation, and 3% osteochondral allograft implantation), concomitant hemi-epiphysiodesis for genu valgum (9%), and patellar tendon medialization (Grammont procedure, 2%).
Conclusion:
Despite the presence of open physes, which generally limits PFI surgical technique options, variation in multiple aspects of MPFLR was high among this cohort of 20 high-volume surgeons.
The treatment approach to patellofemoral instability (PFI) may vary based on a number of variables, such as whether a dislocation episode is a first-time or recurrent event, and patient-based factors, such as age, activity level, and anatomic risk factors of the patient. The management of first-time dislocations, in the absence of severe concomitant knee injuries, remains somewhat controversial. Nonoperative treatment methods, including use of patellar stabilization braces and physical therapy focused on quadriceps strengthening, are common, if not the current standard of care. However, for recurrent PFI, patellar stabilization surgery is considered the consistently recommended approach to optimize activity levels, prevent the short-term dysfunction associated with instability events, and curb the degenerative chondral effects that are associated with repetitive PFI with the goal to enhance long-term joint preservation, given the exceedingly high rates of recurrence described in patients after a second dislocation.8,11
Although the majority of world literature has historically focused on PFI in adult populations, the condition is, in fact, primarily an adolescent and pediatric problem, with the incidence rates in 10- to 14-year-old and 15- to 19-year-old patients far exceeding those of any other 5-year age group in the population, based on epidemiologic evidence. 29 At the same time, young age has been shown to be among the strongest risk factors for recurrence, both with and without surgical treatment, and ranks high among a lengthy list of both demographic and anatomic risk factors for the condition. 31 Thus, the subpopulation most likely to be affected by the condition is also the cohort most likely to experience failure of current treatment methods, both operative and nonoperative. Because more invasive bony realignment approaches, such as tibial tubercle osteotomy and trochleoplasty, are not appropriate for patients with open physes, and techniques historically used in children, such as medial retinacular reefing, medial patellofemoral ligament (MPFL) repair, and semitendinosus tenodesis (Galeazzi procedure), have been shown to have suboptimal stabilization outcomes, MPFL reconstruction (MPFLR) has emerged as the preferred technique for younger patients.3,9,20,23,28 Its utility and favorable safety profile have contributed to a >2-fold increase in the rate of PFI procedures in children over a recent 10-year period. 21
Despite the increase in MPFLR surgery in skeletally immature patients in recent years, evidence indicates that variation in the application of the technique remains significant, a concept that has been shown to contribute to higher costs, decreased value, and poorer overall outcomes in multiple studies of prior conditions in the US health care system.2,4,5,7,11,12,16,30 The described variation may relate, in part, to an evolution in understanding regarding the precise anatomic ligamentous femoral footprint of the MPFL on the medial femur, relative to the distal femoral physis. However, although some initial studies reported attachments in some patients or cadaveric specimens at or proximal to the level of the physis, a recent meta-analysis demonstrated that based on the conclusions of the majority of studies on the subject, and in the vast majority of knees studied, the footprint is distal to the femoral physis. 27 Despite this emerging consensus, there may remain variation in the use of implant types, implant materials, graft selection, fixation constructs on both the patella and femur, and the use of concomitant procedures in association with MPFLR.17,25
The purpose of the current study was to examine the variation in MPFLR techniques applied in a large cohort of skeletally immature patients who underwent surgery performed by 1 of 20 orthopaedic surgeons with different experience levels and specialty training backgrounds, all of whom perform a high volume of PFI surgery in this age group and participate in a research study group on the subject. The study hypothesis was that variation would be high.
Methods
Study Cohort
After institutional review board approval was granted, the operative records of skeletally immature patients who underwent MPFLR between 2016 and 2021 were identified in the prospective cohort study database of the JUPITER (JUstifying Patellar Instability Treatment by Results) study group.
JUPITER is a multicenter, multiarm, prospective longitudinal cohort study involving 12 tertiary care academic centers (28 surgeons) investigating the treatment of PFI. Its aims are 2-fold: to identify risk factors and predictors of outcome for first-time and recurrent PFI and to compare the safety and efficacy of nonoperative treatment, isolated MPFL reconstruction, and “à la carte” surgical approach to treat PFI.
The data included in this study were obtained during a period of data freeze, thus making this investigation an interval analysis of the overall cohort of skeletally immature patients who underwent operative treatment. Patients who underwent a primary, single-stage MPFLR were evaluated. Due to the differing surgical indications associated with some types of cases, the following cases were excluded from the present cohort: revision or staged procedure; concomitant medial-side retinacular or MPFL imbrication, advancement, or repair; bony distal realignment procedures such as tibial tubercle osteotomies; femoral osteotomies; and trochleoplasty (Figure 1).

Flowchart depicting patient selection and exclusion. MPFLR, medial patellofemoral ligament reconstruction; TTO, tibial tubercle osteotomy.
Preliminary demographic information was collected at the initial clinic visit. Patients completed a screening form, and surgeons collected a baseline history and physical examination, which included age, sex, laterality, and mechanism of injury, among other data. After surgery, surgeons completed an operative questionnaire that collected procedural details of the MPFL surgical technique, which included graft selected, patellar and femoral fixation methods and materials, and information regarding concomitant procedures (if any) that were performed (see Supplemental Material). Completed data forms were entered into PatientIQ, a cloud-based software platform that automates the collection of patient reported outcomes (Datamonkey Inc).
Statistical Analysis
Statistical analyses were performed using the Statistical Package for Social Sciences (SPPS) Version 22.0 (IBM Corp). Continuous variables were reported as means and standard deviations, and discrete variables were reported as frequencies and percentages.
Results
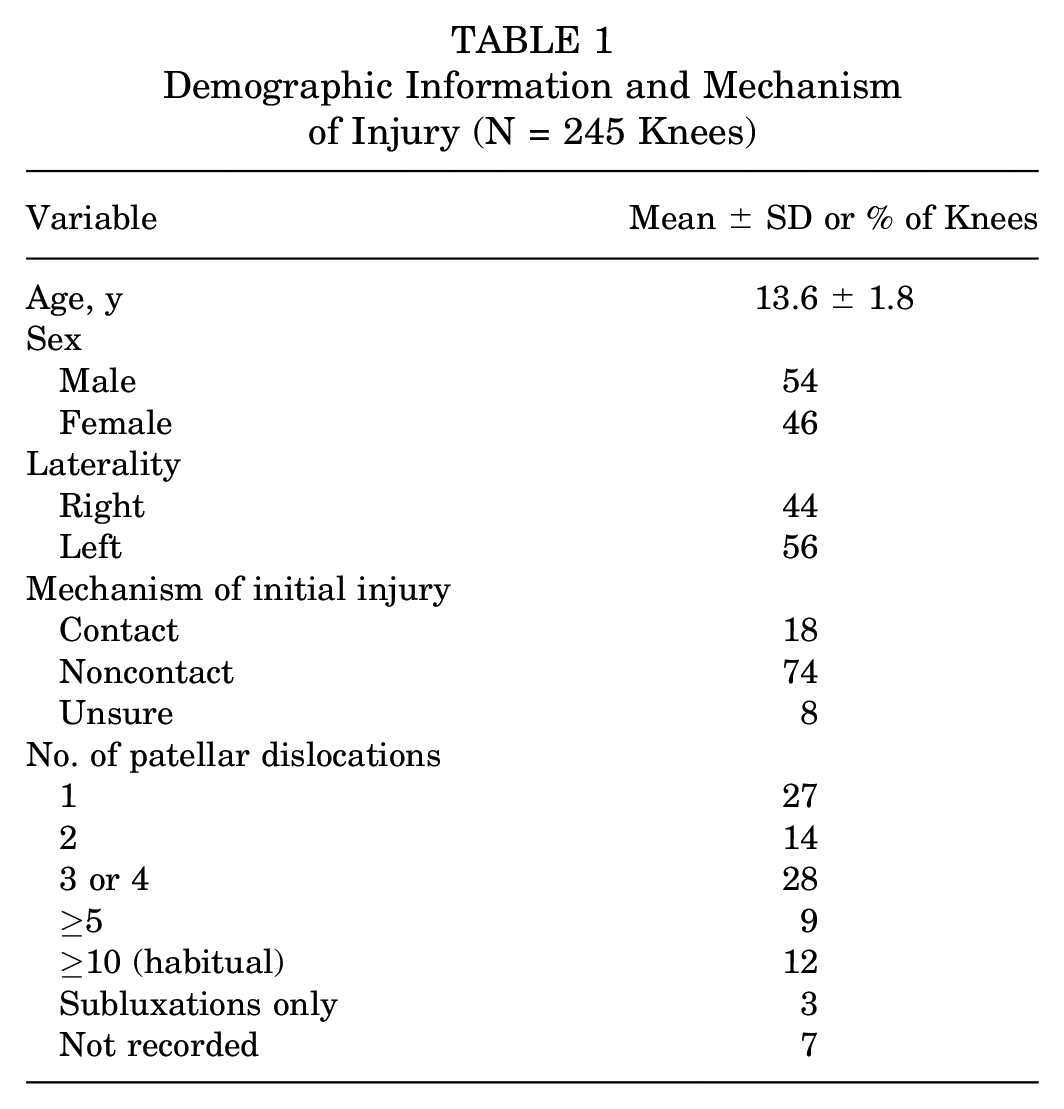
At the time of data mining for the current study, the overall database of patellar instability patients enrolled for participation in the JUPITER study included 1713 knees in 1517 patients. Of these, there were 305 knees (18%) in skeletally immature patients who underwent PFI surgery of any kind, all of whom were deemed to have open physes by the surgeon-investigator upon review of the magnetic resonance imaging closest to the date of the surgery. 6 Among these knees, 245 (46% female, 54% male) met all inclusion/exclusion criteria and comprised the final cohort (Table 1). Eleven tertiary care academic centers (20 surgeons with different experience levels and specialty training backgrounds) were represented by this cohort (Table 2). The mean age of the study cohort was 13.6 ± 1.8 years (range, 5.1-19.0 years) (Figure 2). The initial injury mechanism was of a noncontact nature in 74% and a result of contact in 18%, with 8% patients being unsure. This was a first-time patellar dislocation for 65 knees (27%) and a recurrent dislocation for 180 knees (73%).
Demographic Information and Mechanism of Injury (N = 245 Knees)
Surgeon Fellowship Training Background

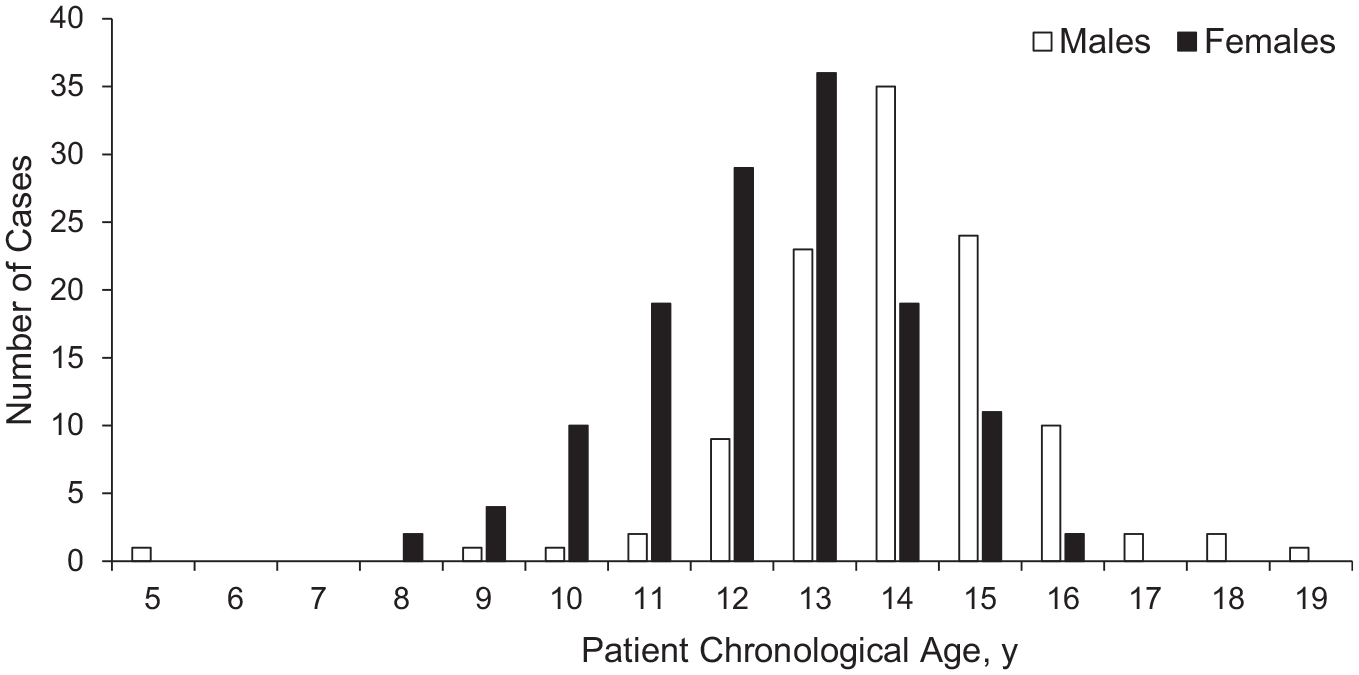
Age distribution of the study cohort.
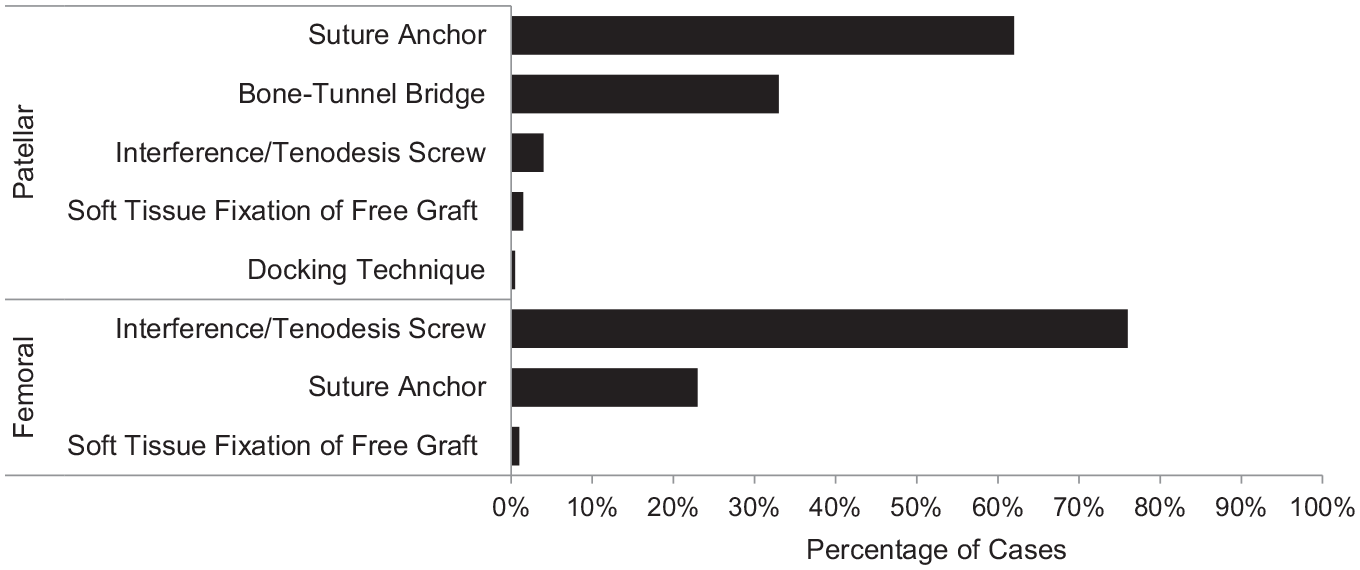
In terms of the MPFLR tendon graft, 41% of knees involved autograft, whereas 59% involved allograft. The most common autograft used was semitendinosus (65%), followed by gracilis (34%) and soft tissue quadriceps (1%). The most popular allograft used was semitendinosus (51%), followed by tibialis anterior (28%), gracilis (20%), and peroneus longus (1%). A suture anchor construct was the most popular patellar fixation technique (62%), followed by the use of tunnel under a bone bridge (33%), interference/tenodesis screws (4%), soft tissue fixation of graft (1.5%), and a docking technique (0.5%) (Figure 3). The majority of surgeons used 2 suture anchors (63%) (Table 3), and the most often used suture anchor material was biocomposite (56%) (Figure 4).
Number of points of fixation.
Number of Fixation Screws Used


Patellar fixation implant material. PEEK; polyetheretherketone.
Interference screws were the most popular femoral fixation construct (76%), followed by suture anchors (23%) and soft tissue fixation of free graft (1%) (Figure 3). The majority of surgeons used either 1 interference screw (97%) or 1 suture anchor at the femur (95%) (Table 3). Biocomposite was the most commonly used interference screw (79%) and suture anchor (69%) implant material (Figure 5).

Femoral fixation implant material. PEEK; polyetheretherketone
Most of the surgeons (51%) identified MPFL femoral location using fluoroscopy only. A combination of fluoroscopy, palpitation of landmarks, and isometric location was the second most popular technique (13%), followed by fluoroscopy and isometric location (10%) (Table 4). Techniques used to further verify the MPFL femoral location included checking isometricity (49%), checking isometricity and fluoroscopy (30%), and fluoroscopy and open identification of landmarks (7%) (Table 5).
Techniques Used to Identify Femoral Location of Medial Patellofemoral Ligament

Techniques Used to Further Verify Femoral Location of Medial Patellofemoral Ligament

In addition to MPFLR, a lateral retinacular procedure was performed in 55 knees (22%), of which 48 (89% of lateral retinacular procedures) underwent a lateral retinacular release and 6 (11% of lateral retinacular procedures) underwent a lateral retinacular lengthening. Overall, 32 knees (13%) underwent osteochondral fracture treatment. Of this subcohort, 18 knees (53% of osteochondral fractures) underwent loose body removal, 13 knees (44% of osteochondral fractures) underwent fixation, and 1 knee (3% of osteochondral fractures) underwent osteochondral allograft implantation. A total of 9% of knees underwent concomitant hemi-epiphysiodesis for genu valgum, and 2% underwent a Grammont realignment (patellar tendon medialization) procedure (Table 6).
Surgical Information Regarding Concomitant Procedures

Discussion
The current study demonstrated relatively high variation in multiple aspects of MPFLR surgery in skeletally immature patients, when collectively performed by 20 surgeon-investigator members of a geographically diverse PFI study group who perform a high volume of pediatric PFI surgery. This relatively high rate of variation was detected despite the presence of open physes in all patients investigated in this large cohort, which should otherwise limit the array of PFI surgical technique options. This relative variation may be accounted for by the diversity of subspecialty training of the surgeons involved in the investigation or by their differences in experience or practice settings, all of which were substantial, as shown by the wide geographic distribution of study institutions. Although such diversity may reflect the general population of surgeons performing these procedures in the United States, the relative variation in the current study is likely to be an underestimate of the true variation across the country, given that study group members are more likely to have common training backgrounds and practice habits similar to each other and because their previous and current collaborations are likely to contribute to shared techniques.
Although variation in surgical techniques for MPFLR has been extensively studied in the adult population, very few previous studies have systematically assessed MPFLR techniques in skeletally immature patients in a comprehensive or rigorous fashion.13,14 A systematic review and meta-analysis by Shamrock et al 24 explored MPFLR performed specifically in skeletally immature patients, describing features of the techniques used on 132 knees across 7 different pooled studies. However, although that review included articles published between 2003 and 2018, during which time studies of allograft technique were shown to be safe and effective, 100% of cases studied in their collective cohort involved use of autograft. In the current series, less than half of patients (41%) had autograft procedures, most likely due to multiple studies suggesting equivalent or superior results with allograft, compared with autograft, as highlighted in a systematic review by Aliberti et al. 1 Given the additional surgical and tourniquet time, risk of complications, and donor site morbidity of autograft tendon harvest, a pendulum shift toward allograft use in MPFLR may be theorized, particularly given that these findings were in a pediatric population, the families of whom may be less apt to accept cadaveric tissue implant. 24 However, these findings may also reflect a bias of surgeons in the United States, who may have more access to allografts than those in other health care systems. Importantly, longer term MPFLR studies in adolescents are rare, so the durability of allograft over time remains somewhat questionable. Other surgeons may be applying concerns about allograft rupture rates from studies regarding anterior cruciate ligament reconstruction, in which autograft has been clearly shown to be superior to allograft for avoidance of graft tears.
Regarding femoral fixation techniques, cases in the series by Shamrock et al 24 showed a relatively even distribution of interference screw and suture anchor femoral fixation constructs, each at 39% of cases. The current series, in contrast, showed 76% screw fixation constructs on the femur, 23% suture anchor constructs, and 1% free soft tissue suture fixation. Interestingly, Aliberti et al 1 reported that >1 in 5 patients underwent femoral fixation in the form of a soft tissue pulley around medial collateral ligament or adductor tendon insertion, a fixation construct absent in the current series. These differences between studies may be explained by the period of time between the current study and the prior studies, during which reaming or drilling of interference screw sockets was shown to be safe in multiple studies, or by a small number of surgeons in the study by Shamrock et al using the less common soft tissue pulley technique.
The current study also investigated the role of concomitant lateral retinacular interventions in the skeletally immature population. Interestingly, in the current study, lateral releases were performed >8 times more frequently than lateral retinacular lengthening, despite some evidence that lateral release may have complications or side effects warranting further interventions. 10
A number of other concomitant procedures and adjunctive techniques were used in this patient population, although not to a consistent degree. Therefore, it is hard to differentiate whether these additional measures were warranted based on specific features of a subset of patients or whether their use is reflective only of variation in the surgeons’ perceptions of the indications for the techniques. For example, although the majority of patients demonstrated enough growth remaining to allow for use of guided growth or hemi-epiphysiodesis techniques to be added to the patellar stabilization provided by the MPFLR, as reflected by a mean age <14 years, only 9% of patients underwent such measures, despite some evidence of the effectiveness of the technique to enhance patellar stability, when alignment can be brought from valgus or neutral coronal plane realignment to neutral or slight varus alignment.15,19,22 This low percentage of cases involving this technique may be indicative of the large percentage of adult sports medicine surgeons, who are less familiar with the pediatric orthopaedic principles of this technique, managing adolescent patients in the cohort, or the relatively recent introduction of this technique into pediatric sports training. Future research is needed to better understand the role of this technique as an element of patellar stabilization in skeletally immature patients. The use of these concomitant procedures, to inconsistent degrees, represents an additional illustration of the high variation that exists with treatment of PFI in children.
Limitations
Limitations of the current study include the lack of granularity in a number of variables that may be relevant to the patient cohort that underwent MPFLR surgery. Although demographic and injury data, such as sex, laterality, and mechanism of injury, were reflected in the current data, other factors, such as anatomic risk factors, activity level, and preoperative patient-reported outcomes, may have explained some of the variation demonstrated in surgical technique. 18
Conclusion
The current study demonstrated high variation in the application of different technical principles, implants, and techniques in MPFLR surgery for skeletally immature patients with PFI. Given the well-established importance of decreasing variation for health care cost containment and optimization of outcomes, comparative studies and substratified analyses are needed to better elucidate the most favorable techniques and their components. 26
Authors
Jacqueline Brady, MD (Oregon Health and Science University Hospital, Portland, Oregon); Peter Fabricant, MD, MPH (Hospital for Special Surgery, New York, New York); Jack Farr, MD (OrthoIndy Hospital, Indianapolis, Indiana); Jason Koh, MD (NorthShore Skokie Hospital, Skokie, Illinois); Dennis Kramer, MD (Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts); Robert Magnussen, MD (Ohio State University Wexner Medical Center, Columbus, Ohio); Matthew Milewski, MD (Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts); Lauren Redler, MD (Columbia University Irving Medical Center, New York, New York); Sabrina Strickland, MD (Hospital for Special Surgery, New York, New York); Marc Tompkins (TRIA Orthopedic Center, Bloomington, Minnesota); Adam Yanke, MD, PhD (Midwest Orthopaedics at Rush, Rush University Medical Center, Chicago, Illinois); Yi-Meng Yen, MD, PhD (Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts).
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241300516 – Supplemental material for Variation in Surgical Technique for Medial Patellofemoral Ligament Reconstruction in Skeletally Immature Patients: Data From the JUPITER Prospective Multicenter Study Group
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241300516 for Variation in Surgical Technique for Medial Patellofemoral Ligament Reconstruction in Skeletally Immature Patients: Data From the JUPITER Prospective Multicenter Study Group by Benton E. Heyworth, Sofia Hidalgo Perea, Daniel W. Green, Matthew W. Veerkamp, Eric J. Wall, Philip L. Wilson, Henry B. Ellis, Danielle E. Chipman, Beth E. Shubin Stein, Shital N. Parikh, Jacqueline Brady, Peter Fabricant, Jack Farr, Jason Koh, Dennis Kramer, Robert Magnussen, Matthew Milewski, Lauren Redler, Sabrina Strickland, Marc Tompkins, Adam Yanke and Yi-Meng Yen in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted April 19, 2024; accepted June 4, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.E.H. has received education payments from Arthrex, consulting fees from Imagen Technologies, and royalties from Springer Science and has stock/stock options in Imagen Technologies. D.W.G. has received consulting fees from Arthrex and OrthoPediatrics Canada; nonconsulting fees from Synthes GmbH; speaking fees from AO Trauma International and Arthrex; and royalties from OrthoPediatrics Canada, Pega Medical, and Wolters Kluwer Health. P.L.W. has received research support from Allosource, education payments from Pylant Medical, and royalties from Elsevier. H.B.E. has received education payments from Pylant Medical, speaking fees from OrthoPediatrics, and hospitality payments from Stryker. B.E.S.S. has received research support from CONMED and Arthrex, and her spouse has received consulting fees and royalties from Arthrex. S.N.P. has received consulting fees from Pfizer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Cincinnati Children’s Hospital Medical Center (ref No. 2015-7943).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.