
Abstract
Background:
Young athletes who undergo surgery for a rotator cuff tear (RCT) are expected to return to sports (RTS) at the preinjury level.
Purpose:
To determine the rate and level of RTS and associated factors after RCT surgery in young athletes.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A literature search was performed in PubMed, Embase, and Cochrane Library the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The inclusion criteria were studies in English evaluating RTS after surgical treatment of RCTs in athletes <40 years. Study quality was evaluated according to the Methodological Index for Nonrandomized Studies scores. Fixed-effects and random-effects meta-analyses were conducted to investigate the overall RTS rate and the ability to RTS at the preinjury level and explore the heterogeneity of the studies.
Results:
Of 168 studies initially identified, 13 studies (332 athletes; 270 competitive and 62 recreational) were included. The mean age of the athletes was 26.1 years (range, 13.2-39 years). Eleven studies (289 athletes) reported the type of sports; the most common sports were baseball (n = 195), football (n = 47), and tennis (n = 13). A total of 25 athletes were lost to follow-up, leaving 307 athletes with postoperative RTS data for meta-analysis. The combined rate of RTS according to the fixed-effects model was 84% (95% CI, 80%-88%). The level of RTS was evaluated in 11 studies (251 athletes), and according to the random-effects models, the combined rate of RTS at the preinjury level was 63% (95% CI, 49%-77%). In a subgroup analysis, the rate of RTS at the preinjury level was significantly different between competitive athletes (61% [95% CI, 46%-76%]) and recreational athletes (89% [95% CI, 78%-99%]) (P = .004).
Conclusion:
Results of this review indicated that most young athletes were able to RTS after RCT surgery, and more than half were able to RTS at the preinjury level. Compared with competitive athletes, a higher proportion of recreational athletes were able to RTS at the preinjury level after surgery.
After shoulder dislocation/subluxation, rotator cuff tear (RCT) is one of the most common shoulder problems encountered by orthopaedic surgeons, and it is a condition that affects patients’ motor ability and reduces their quality of life. 23 RCTs are uncommon injuries in people <40 years old but cause significant morbidity if unrecognized.1,5,15 Because athletes are at an increased risk for traumatic and overuse injuries,12,16,20,21 many people worldwide undergo surgical treatment annually for RCTs. Overhead athletes are particularly at risk of injury because repetitive physiological demands imposed on the shoulder increase microtrauma, while contact and collision athletes increase the risk of acute traumatic tears. 14
Return to sports (RTS) is an important challenge after RCT surgery and is a measure of success for athletes. In a large study, including 683 athletes aged from 15 to 81 years, the overall rate of RTS was 84.7%, including 65.9% returning to the preinjury level of sports, but only half of the professional athletes returned to the preinjury level of sports. 14 The main expectation of athletes is RTS at the preinjury level after treatment, 25 especially for young professional athletes. However, few studies have evaluated the rate and level of RTS after RCT surgery, especially for younger athletes.
The purpose of this study was to systematically review the literature on the rate and level of RTS and associated factors after RCT surgery in young athletes. We hypothesized that the level of RTS after RCT surgery for young athletes would be associated with the type of athlete (competitive vs recreational), the type of tear (partial- or full-thickness), and the type of surgery (debridement or repair).
Methods
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 19 guidelines were followed to perform the systematic review of the literature and the meta-analysis and to present the results.
Search Strategy
An electronic search of the literature was performed in MEDLINE via PubMed, Embase, and Cochrane Library using the following keywords: (1) rotator cuff repair; (2) return to sports; and (3) athletes. The search terms were as follows: (RCT or rotator cuff repair) AND (return to sports) AND (athletes). The final search was conducted on December 14, 2022. Furthermore, we studied the references and then included appropriate references, which were referenced in the papers we reviewed in this study.
Selection Criteria
The inclusion criteria encompassed cohort studies or case series in the English language, with evidence levels ranging from 1 to 4, evaluating patients with partial- or full-thickness RCTs who underwent surgical treatment (debridement or rotator cuff repair). Only patients <40 years were considered. The exclusion criteria were literature reviews, expert opinions, nonclinical studies, case reports, and studies not assessing RTS. Importantly, patients >40 years in the literature were excluded. Associated lesions—including shoulder instability, superior labral anterior-posterior (SLAP) lesions, et cetera—were not considered exclusion criteria. Two independent authors read the abstract of the article and analyzed the articles related to the abstract. The references of each article are also carefully evaluated for inclusion. Any disagreements or issues were resolved by a review of the articles, and the senior author (G.C.) made the final decision.
Evaluation of the Quality of the Studies
The quality of the included studies was evaluated according to the Methodological Index for Nonrandomized Studies (MINORS) score. 27 It includes 12 items, with 8 items for noncomparative studies, with the last 4 items specific for comparative studies. The score for the items varies from 0 to 2 (0, not reported; 1, reported but poorly done or inadequate; 2, reported but well done and adequate). The highest possible score is 16 for noncomparative studies and 24 for comparative studies.
Data Collection
Data were collected based on a predefined standardized form according to the protocol, as follows: (1) study characteristics (design, year, and number of patients); (2) characteristics of the study participants (age, sex, sport practiced, and level of sport [competitive vs recreational], and dominant shoulder); (3) characteristics of the RCT (injury mechanism, injury severity, tear type, and time between injury and surgery); (4) treatment (surgical treatment, arthroscopic or open surgery, and associated surgeries); (5) clinical and functional results at final follow-up; and (6) complications at final follow-up. The athletes were divided into competitive and recreational according to Araújo and Scharhag criteria. 4 Competitive athletes were those who regularly trained and competed in either the professional or amateur leagues, thus, professional athletes were included within the cohort of competitive athletes.
Data Analysis
The data were analyzed using Review Manager 5.4. The primary outcome was RTS after surgical treatment of RCTs, and the secondary outcome was the change in functional outcome scores from the preoperative to the final follow-up. RTS was analyzed by rate (ability to return at any level) and level (preinjury vs higher/lower level). The I2 index was used to measure the heterogeneity of the included findings, 13 with I2 values interpreted as low (25%-49%), moderate (50%-74%), or high (≥75%). As the expected heterogeneity was high, we performed a meta-analysis of the RTS data according to the random-effects model. The mean RTS rate (with 95% CI) in the different studies and the combined rate were plotted in a forest plot. In addition, subgroup analyses were performed for related factors affecting the level of RTS (competitive vs recreational athlete, partial- vs full-thickness tear, debridement vs repair).
Publication bias was assessed using a funnel plot representing the size of each study on the y-axis, related to the immediate estimated effect of treatment on the x-axis, with the larger study at the top and the smaller study at the bottom. If there is no bias, then the point estimates will be evenly and symmetrically distributed around the real effect of the treatment. 9
For all trials, P < .05 was considered statistically significant.
Results
Included Studies
A total of 13 studies ¶ (N = 332 athletes) met the inclusion and exclusion criteria. The PRISMA flowchart in Figure 1 summarizes the study selection process.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of study selection.
Study Characteristics and Quality
All 13 studies were retrospective and included 12 noncomparative studies (case series) and 1 comparative (case-control) study 22 in which professional pitchers who underwent surgery for RCT were compared with controls (pitchers with no history of RCT surgery). The mean (±SD) MINORS score for the noncomparative studies was 10.1 ± 1.7, and the MINORS score for the case-control study was 20. The mean follow-up duration was 3.1 years (range, 0.3-10 years) (Table 1).
Study Characteristics a

MINORS, Methodological Index for Nonrandomized Studies; NR, not reported; LOE, level of evidence.
Patient Characteristics
A total of 332 athletes were included in the 13 studies, including 284 men and 48 women, with a mean age of 26.1 years (range, 13.2-39 years) (Table 2). There were 270 competitive athletes—including professional athletes and 62 recreational athletes. Also, 8 studies reported dominant or nondominant side injuries,2,5,6,11,17,18,26,31 that found the dominant shoulder was involved in 90.8% of athletes (207/228). Eleven studies (289 athletes) reported the type of sports, # and the most common sports were baseball (n = 195), American football (n = 40), and rugby (n = 17).
Patient Characteristics a

NR, not reported.
Mean ± SD.
Some patients participated in >1 sport.
Characteristics of Injuries and Treatment
Overall, 7 studies5,6,8,11,15,26,28 (184 athletes) reported the cause of injury (traumatic or nontraumatic), with 175 (95.1%) reported accidents such as a fall on the shoulder or a direct hit. The mean time between the injury or the onset of symptoms and the surgery was 15.6 months (range, 3 weeks to 10 years). RCT type was described in 9 studies2,5,6,11,15,17,26,28,29 (233 athletes): 153 (65.7%) were partial tears, 78 (33.5%) had full-thickness tears, and 2 had contusion injuries (0.8%). The treatment type was reported in 11 studies ** (261 shoulder surgeries)—123 (47.1%) arthroscopic debridements, 114 (43.7%) arthroscopic repairs, and 24 (9.2%) open surgeries. The most frequently associated surgical procedure was acromioplasty (Table 3).
Characteristics of Injuries and Treatment a
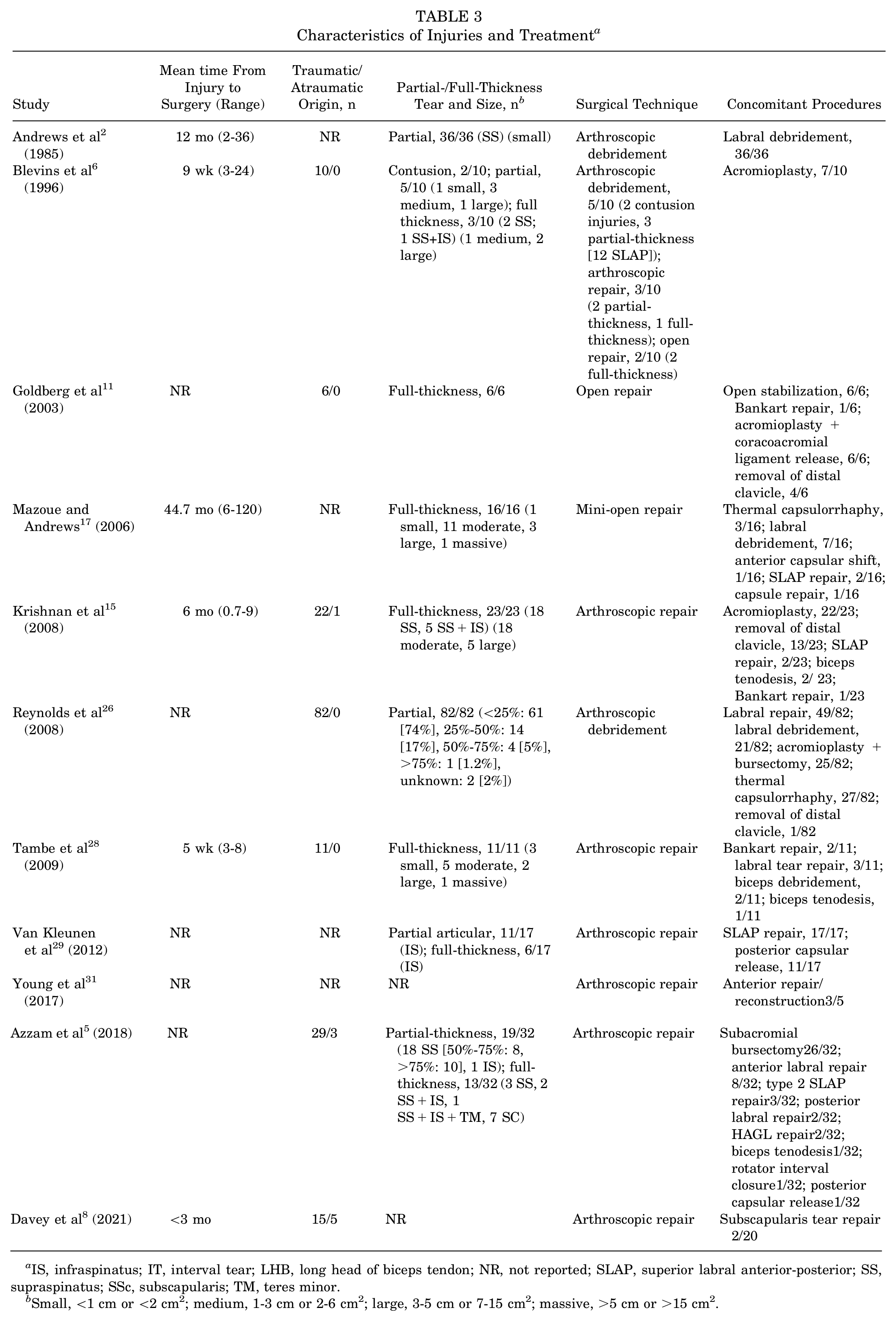
IS, infraspinatus; IT, interval tear; LHB, long head of biceps tendon; NR, not reported; SLAP, superior labral anterior-posterior; SS, supraspinatus; SSc, subscapularis; TM, teres minor.
Small, <1 cm or <2 cm2; medium, 1-3 cm or 2-6 cm2; large, 3-5 cm or 7-15 cm2; massive, >5 cm or >15 cm2.
Rate and Level of RTS
Of the 332 athletes, 25 athletes were missing information on RTS; thus, the remaining 307 athletes were included in the meta-analysis. The combined rate of RTS according to the fixed-effects model was 84% (95% CI, 80%-88%), with low heterogeneity (I2 = 22%) (Figure 2). Also, 6 studies reported the mean time to RTS, which ranged from 4.1 to 17 months. The level of RTS was evaluated in 11 studies †† (251 athletes). In the meta-analysis according to the random-effects models, the combined rate of RTS at the preinjury level was 63% (95% CI, 49%-77%), with high heterogeneity (I2 = 85%) (Figure 3). However, the funnel plot was symmetric, suggesting that no publication bias was more marked in small studies (Figure 4).
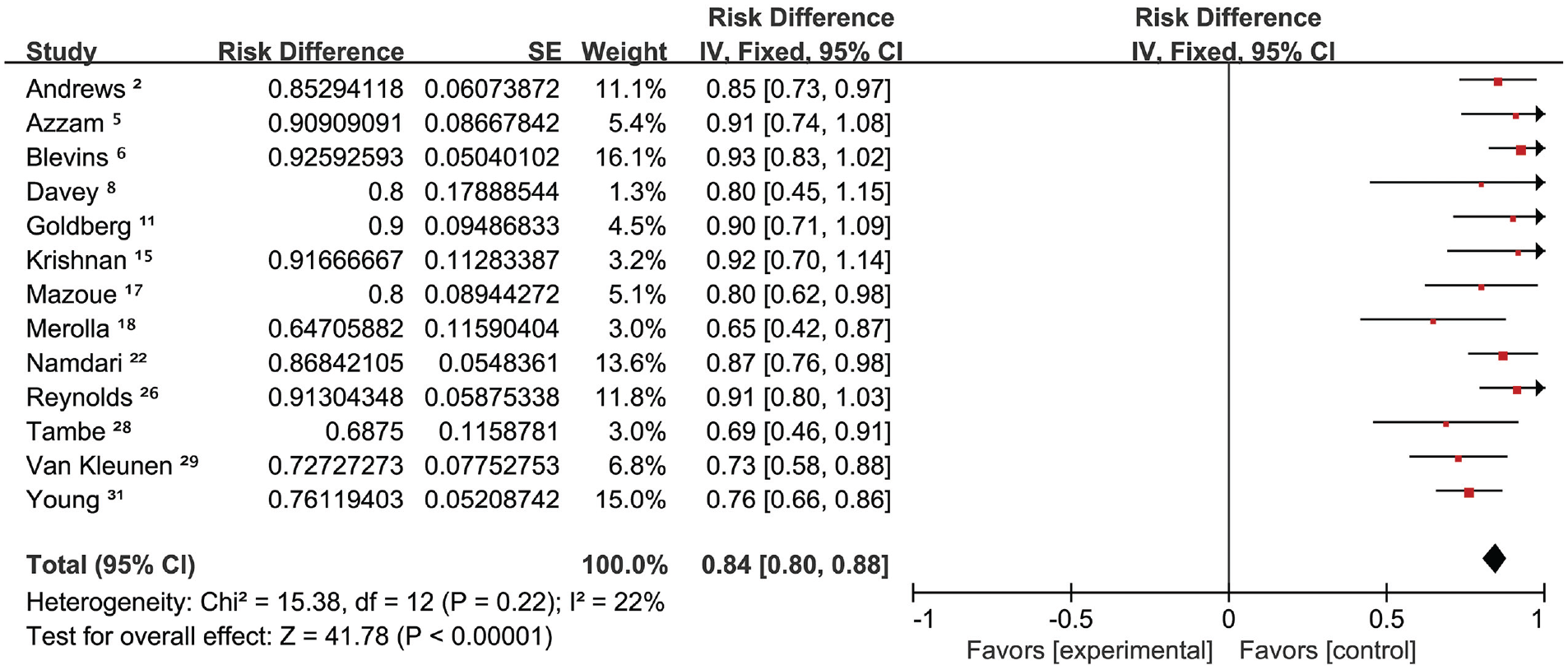
Forest plot of the combined rate of return to sports. SE, standard error.
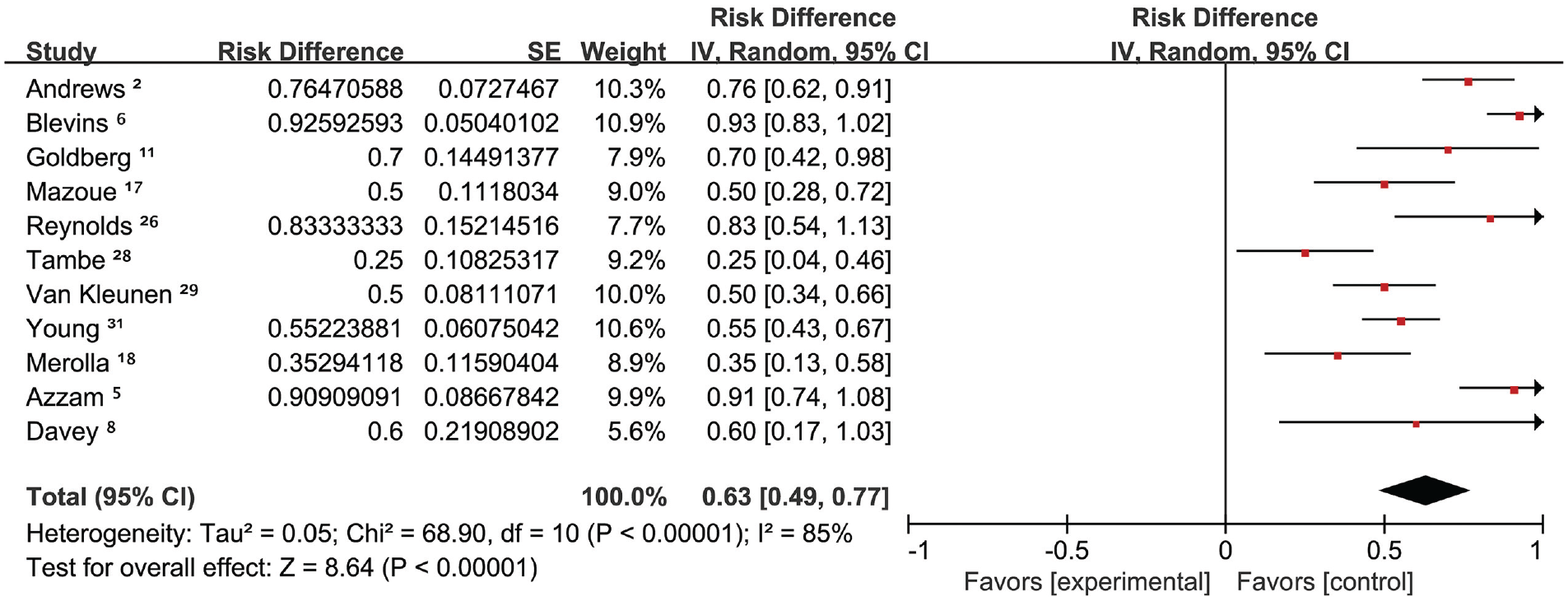
Forest plot of the combined rate of return to sports at the preinjury level. SE, standard error.

Funnel plot chart evaluating publication bias. OR, odds ratio.
Subgroup Analyses
Competitive vs Recreational Athletes
Eleven studies †† (n = 251 athletes) assessed athlete level. According to the meta-analysis of the random effects model, there was a significant difference in the rate of RTS at the preinjury level between the competitive athletes and recreational athletes—60% (95% CI, 46%-75%) and 89% (95% CI, 78%-99%; P = .002), with an I2 index of 82% and 0%, respectively.
Partial- vs Full-Thickness Tears
Information on partial- and full-thickness tears was extracted from 8 studies2,5,6,11,17,26,28,29 and was evaluated by tear type. Based on the random-effects model, the rate of RTS at the preinjury level in partial-thickness tears was 72% (95% CI, 53%-92%) and full-thickness tears were 69% (95% CI, 41%-96%; P = .83), with an I2 index of 88% and 89%, respectively.
Debridement vs Repair
Arthroscopic debridement was used as the only repair method in 2 studies,2,26 while surgical repair was used in 8 studies.5,8,11,15,17,28,29,31 Based on the random-effects model, the rate of RTS at the preinjury level in arthroscopic debridement was 63% (95% CI, 47%-80%), and the rate of surgical repair was 69% (95% CI, 51%-88%; P = .64), with an I2 index of 68% and 88%, respectively.
Functional Outcomes
Functional outcomes were evaluated in 10 studies. ‡‡ Outcome scores varied across the study findings6,15,18,28; nonetheless, results showed significant improvements between the preoperative assessment and the final follow-up (Table 4).
Functional Outcomes a

Dashes indicate areas not applicable. ADL, activities of daily living; AOSRS, Athletic Outcome Shoulder Rating Scale (range, 0-90); ASES, American Shoulder and Elbow Surgeons Shoulder Score (range, 0-100); KJOC, Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow score (range, 0-100); MSF-12, 12-item Mental Short Form; NR, not reported; PSF-12, 12-item Physical Short Form; SF-12, 12-Item Short-Form Health Survey; WORC, Western Ontario Rotator Cuff Index (range, 0%-100%).
Scores are presented as mean (range) or mean ± SD unless otherwise indicated.
Postoperative Complications
Six studies2,5,8,15,28,31 (130 athletes) reported postoperative complications at the final follow-up, of which 4 studies2,8,28,31 did not find any complications. Infection was found in 1 athlete, 15 retear was found in 2 athletes, 5 and axillary nerve palsy was suspected in 3 athletes.5,15 The overall rate of postoperative complications was 4.6%.
Discussion
Our systematic review analyzed 13 studies (322 athletes) on RTS after RCT surgery in younger athletes (age <40 years; mean age, 26.1 years) and tried to find factors that may influence the level of RTS. The results showed the overall RTS rate was 84%, with 63% of the participants able to RTS at the preinjury level after rotator cuff surgery. Compared with competitive athletes, a higher proportion of recreational athletes were able to RTS at the preinjury level after surgery.
Two studies,1,14 whose participants had a wide age variation, systematically evaluated and analyzed the results of RTS after rotator cuff surgery. The most important feature of this article was to reduce the age range and bias for athletes, and the inclusion criteria are more in line with the characteristics of the susceptible population. However, other studies focused only on the athletes with RCT.3,10 In our study, we established the rate of RTS after RCT surgery in young athletes at 84%, with 63% returning to the preinjury level of sport after surgery.
In the subgroup analysis, 61% of competitive athletes and 89% of recreational athletes returned to sports at the preinjury level after RCT surgery (P = .004). This meta-analysis has the same results as the systematic review by Klouche et al, 14 who reported higher RTS rates of 81.4% in recreational athletes and significantly lower RTS rates of 49.9% in competitive athletes. According to the literature, the impact factor of the RTS level is professional athletic status. 17 However, the review by Altintas et al 1 obtained different results than those of the present review, where the overall incidence of RTS at the preinjury level was 70.2%—with 61.5% of competitive athletes and 73.3% of recreational athletes—and the difference was not statistically significant. Returning to sports but not to the preinjury level may signify the end of a competitive athlete's career, whereas recreational athletes may view it as an acceptable outcome. Competitive athletes may also have some other factors affecting their RTS at the preinjury level, such as contract, age, injuries of other parts of the body, and psychological states. It is important to note that RTS at the preinjury level may not be completely related to injury and subsequent shoulder surgery. Withdrawal from competitive sports may be a result of fear of reinjury or some other factors.3,7,30
In a study by Altintas et al 1 on 34 baseball and softball athletes, only 13 players (38%) were able to RTS at the preinjury level after RCT surgery. Competitive sports (61.5%) and overhead sports (38%) were associated with lower rates of return. 24 Unfortunately, no study has compared the rotator cuff repair outcomes between athletes participating in overhead and contact sports and those participating in nonoverhead or noncontact sports. Furthermore, most studies did not distinguish between competitive athletes and recreational athletes in these subgroups.
In the subgroup analysis of partial- and full-thickness tears, we reported the same results as the systematic review by Klouche et al 14 and did not find any significant difference in the rate of RTS at a preinjury level between partial and full-thickness tears. Both debridement and arthroscopic repair for rotator cuff injuries may have different indications. The choice of surgical method depends on the patient's specific situation and the physician's advice. 6 We also conducted a subgroup analysis between arthroscopic debridement and surgical repair, which showed that the 2 treatments had no significant difference in the level of RTS.
Concomitant lesions, such as labrum injury, cannot be ignored when treating RCT, especially for young athletes. Azzam et al 5 found that only 43% of patients treated with concurrent labral repair felt that their athletic performance was the same or better as their presurgery level, as opposed to 78% of patients who did not undergo labral repair (P = .049). Similarly, Van Kleunen et al 29 concluded that for throwing athletes, the combination of infraspinatus tear, SLAP tear, and deficit in glenohumeral internal rotation resulted in a guarded prognosis in RTS at the preinjury level. Labral tears can also be treated with debridement and repair. Therefore, the presence of a tear may not be an indicator of poor return, but rather of the treatment itself. Overall, the concomitant pathology should not be overlooked and should be carefully addressed.
Limitations
Our study is not without limitations. First, the level of evidence was very low in most of the included studies. Assessment of the study quality showed a mean MINORS score of 10.1 for the noncomparative studies, mainly because of the large number of retrospective case series. Because of the diversity of reports (eg, there is a big difference between a young professional baseball player and a young recreational golfer) and the lack of specific outcome data for each athlete, we were unable to perform a more detailed analysis. Different studies had different descriptions of athletic level, which affected the grouping of data, which may in turn have affected the results of the subgroup analysis. More prospective studies should focus on evaluating the association of RTS and tendon healing, the type and level of sports practiced, and psychological factors 30 to understand the improvement of rotator cuff repair in athletes.
Conclusion
The results of this review indicated that most young athletes were able to RTS after RCT surgery, and more than half were able to RTS at the preinjury level. Compared with competitive athletes, a higher proportion of recreational athletes were able to RTS at the preinjury level after surgery. These data may help in the discussion and education of young athletes on the rate and level of RTS after RCT surgery.
Footnotes
Final revision submitted May 15, 2024; accepted May 20, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the National Natural Science Foundation of China (No. 82172423 and 81871770), the Beijing Municipal Natural Science Foundation (No. 7222209), and the Beijing Natural Science Foundation (No. L222094).