
Abstract
Background:
The concept of on-track versus off-track bone lesions in glenohumeral instability continues to evolve. Although much has been ascertained from an original biomechanical model, bony pathological changes, especially on 3-dimensional (3D) imaging, have not been fully evaluated.
Purpose:
To compare the differences in on-track versus off-track lesions to characterize glenoid and humeral head bone defects using 3D modeling software.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A consecutive cohort of 75 patients with recurrent anterior instability, with evidence of Hill-Sachs lesions (HSLs) and glenoid bone loss (GBL) and a mean age of 27.1 years (range, 18-48 years), were reviewed. 3D models of unilateral proximal humeri and glenoids were reconstructed. The volume, surface area, width, and depth of identified HSLs were quantified, along with their location (medial, superior) and orientation (Hill-Sachs angle). The percentage, width, and length of GBL as well as the glenoid track status were calculated. The on-track and off-track groups were compared using the Mann-Whitney U test.
Results:
The off-track group had greater HSL surface area (374.23 vs 272.64 mm2, respectively; P = .001), more HSL medialization (14.96 vs 17.62 mm, respectively; P = .028), greater HSL volume (603.08 vs 433.61 mm3, respectively; P = .007), and a greater mean HSL width (16.06 vs 11.53 mm, respectively; P = .001) than the on-track group. The off-track group also had greater GBL (22.55% vs 17.73%, respectively; P = .037), a greater GBL width (6.92 vs 3.58 mm, respectively; P < .001), and a greater GBL length (21.61 vs 16.1mm, respectively; P = .015) than the on-track group. Further analysis of large off-track lesions revealed a greater Hill-Sachs angle (33.16° vs 26.20°, respectively; P = .035) and a more superior extent of HSLs compared with borderline off-track and on-track lesions.
Conclusion:
Off-track lesions were found to have larger GBL, a larger HSL width, a more medialized HSL, and greater HSL surface area. This study outlines the specific characteristics of high-risk bipolar bone loss lesions to simplify the identification of patients in a clinical setting and aid in appropriate treatment planning.
Keywords
The glenohumeral joint is prone to instability because of its lack of bony constraint.3,5 The majority of glenohumeral dislocations occur anteriorly and often result in fractures in either the glenoid, the humeral head, or both. 5 The incidence of glenoid rim fractures after an anterior shoulder dislocation has been reported to be as high as 35%. 19 Further, attritional anterior glenoid bone loss (GBL) can lead to significant narrowing of the glenoid fossa, particularly with recurrent dislocations. 3 More recently, the importance of Hill-Sachs lesions (HSLs) has been brought to light. 16 These have been reported in up to 90% of first-time anterior dislocations. 3
The interplay of bipolar lesions with both GBL and HSLs likely sheds the best light on this complex problem. Yamamoto et al 18 defined the “glenoid track” by characterizing the posterior humeral head articular surface and its articulation with the glenoid at varying degrees of abduction and external rotation. These authors found that the location of the HSL with respect to the glenoid track determines whether the lesion engages the glenoid rim during motion.
The location of an HSL in relation to the glenoid track and the degree of GBL are now understood to be important clinical findings for surgical outcomes and thus influence the treatment algorithm for anterior shoulder instability. 3 Even though the glenoid track concept is the current gold standard for describing on-track versus off-track lesions, the measurement and calculation of the glenoid track can be time consuming. A recent expert consensus concluded that HSLs are poorly quantified and classified by current imaging systems. 15 There remains a paucity of literature describing the morphology and interplay of bipolar lesions, especially involving advanced measures of size and location. To our knowledge, no previous studies have described specific characteristics of lesions with the glenoid track concept for the simpler identification of patients who are at a high risk for recurrent instability.
The purposes of this study were to assess the characteristics of GBL and HSLs by utilizing 3-dimensional (3D) modeling in patients with a history of anterior shoulder instability and correlate these measures with on-track and off-track lesions. It was hypothesized that off-track lesions would have statistically significantly different radiological measurements of GBL and HSLs compared to on-track lesions.
Methods
After institutional review board approval (NMCSD.2005.0038), data were collected from a consecutive pool of patients presenting to the senior author (M.T.P.) with recurrent anterior shoulder instability. All patients aged between 18 and 65 years presenting with HSLs with available computed tomography (CT) scans were identified and subsequently enrolled. Only patients with a minimum of 5% GBL were included in analysis. The reason for this criterion was 2-fold; first, we sought to avoid potential GBL measurement errors in analysis, and second, <5% GBL was considered to be clinically insignificant in the setting of bipolar bone loss and therefore did not require preoperative CT.10,11 Patients were excluded from analysis if they presented with posterior shoulder instability, presented with multidirectional shoulder instability, or had a history of shoulder-stabilizing surgery. Imaging computations and analyses were performed in accordance with the methodology described by previous studies.6,14 A total of 75 patients with recurrent anterior shoulder instability with available CT scans showing visible HSLs and GBL were included in our analysis.
CT Imaging
All patients underwent standard glenohumeral CT using Sensation 64 (Siemens), a 64-slice scanner. Patients were placed supine with their arms in an adducted and neutral position. Imaging data were acquired with 0.6 mm of collimation, 140 kV, 300 mAs, and a slice thickness of 2 mm.
3D Surface Models
Mimics software (Materialise) was used to convert all 2-dimensional (2D) CT scans into 3D images. DICOM (Digital Imaging and Communications in Medicine) data from the 75 patients’ 2D CT scans were analyzed using Mimics software by selecting the 2D region of interest and then extracting to the contour of the cortical bone of the humerus and scapula. The segmented 2D CT scans were then used to create 3D models of the humerus and scapula for each patient in stereolithography (.stl) files. This method has been used in prior studies as well.9,10
Characterization of HSLs
The .stl files allowed for full 360° manipulation of the models. The 3D reconstructed models were exported to 3-matic (Materialise). Articular and HSL surface areas were marked and measured using a touch screen and stylus pen to locate respective areas on the humeral head. A 3D representation of a “fixed” humerus, defined as a humeral head without an HSL, was obtained by matching the contour of the HSL rim and the humeral head. The HSL humerus model was then digitally subtracted from the fixed humerus model, producing a 3D model of only the HSL. This model was used to obtain dimensional measurements, including the volume, width, and depth of the HSL in all patients.
The width and depth were obtained in the 3D models using the polyline function to show a 3D representation of each 2D axial cut while still allowing the manipulation of the figure in 3 dimensions to ensure that the widest and deepest points were measured accurately. The medialization, vertical position, and angle of HSLs were measured from 3D images of the humeral head in the true posterior view. These images were obtained and exported to ImageJ (National Institutes of Health) to record 2D measurements of the reconstructed 3D model.
Hill-Sachs Angle
The Hill-Sachs angle (HSA) was defined as the best-fit line through the deepest aspect of the lesion and the humeral shaft of the diaphysis axis6,14 (Figure 1).

Measurement of the Hill-Sachs lesion's center angle, defined as the best-fit line through the deepest aspect of the lesion and the humeral shaft of the diaphysis axis. The angle in image (A) is smaller than the angle in image (B) which represents higher risk lesion.
Medialization and Vertical Position
The most superior point and the most inferior point constituted the most superior and inferior extents of the HSL, respectively. The superior-to-inferior distance was divided into 4 equal segments, and the medial extent of the HSL was measured at each of the 4 points. After that, the average was computed and reported. The vertical position of the HSL was defined as the distance from a horizontal line that intersected the most superior point of the humeral head (Figure 2).
Measurement of medialization of the Hill-Sachs lesion (HSL), defined as the normalized distance from a line parallel to the humeral shaft that is tangential to the humeral head to the most medial extent of the HSL at the given level. There were 4 points measured at equidistant intervals along the HSL. The most medialized HSL would be the smallest amount of medialization. The HSL in (B) is more medialized (higher risk) than the HSL in (A). Similarly, the superior extent of the HSL is demonstrated via the blue line, and off-track lesions were found to have a greater superior extent (B; high risk lesion). The red line represents the most superior aspect of humeral head.
Characterization of GBL
All reconstructed 3D glenoids were orientated to the oblique sagittal plane in the en face view and exported to ImageJ to record 2D measurements of the 3D model. The 2D measurements of the glenoid included total surface area of bone loss (%), bone loss width (mm), bone loss length (mm), and glenoid track status. Measurements were obtained as follows.
GBL (Surface Area)
Total GBL was calculated using the perfect-circle method as described by Hamamoto et al. 9 The best-fit circle method was utilized with the en face view of a 3D glenoid, effectively quantifying GBL. The percentage of bone loss was calculated by dividing the surface area of the bone defect by the area of the true circle (Figure 3).

The percentage of glenoid bone loss (GBL) was calculated using the best-fit circle method. (A) The amount of GBL was <20% and did not represent a higher risk for dislocations in the setting of a smaller Hill-Sachs lesion. (B) In contrast, there was a higher amount of GBL and thus a higher risk for recurrent instability.
Glenoid Defect Length
The glenoid defect length was measured as the inferior-to-superior distance of the glenoid defect in the en face view (Figure 4).

Measurement of the glenoid defect length, defined as the inferior-to-superior distance of the glenoid defect in the en face view.
Glenoid Defect Width and Glenoid Track Status
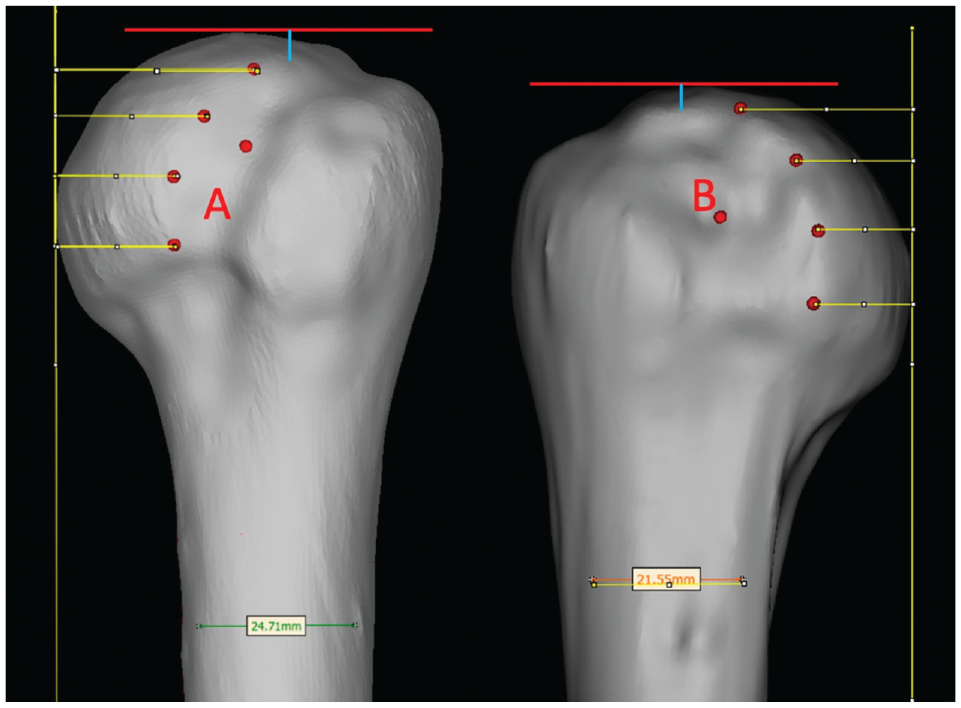
The glenoid track, defined as the contact area between the glenoid and the humeral head, was calculated according to Omori et al. 13 The best-fit circle method was used to predict the width of the glenoid. This value was multiplied by 83%, and the maximum width of the glenoid defect was subtracted. Using 3D reconstructed models, the Hill-Sachs interval was measured from the most medial point of the HSL to the insertion of the rotator cuff tendon. The lesion was “on-track” if the glenoid track was greater than the Hill-Sachs interval, whereas a lesion that extended medially to the medial margin of the glenoid track was “off-track,” resulting in a risk for dissociation (Figures 5 and 6).

Measurement of the glenoid track and the width of the Hill-Sachs lesion. The mean width of the Hill-Sachs lesion is smaller (14mm) than the glenoid track (21.1mm), indicating that this lesion is on-track.

Measurement of the glenoid track and the width of the Hill-Sachs lesion. Blue circle represents best-fit circle technique. The mean width of the Hill-Sachs lesion is greater (19.5mm) than the glenoid track (18.5mm), indicating that this lesion is off-track.
Subgroup Analysis
Subgroup analysis was performed to analyze large off-track lesions (defined as a maximum width of the HSL >1 mm larger than the glenoid track) versus borderline off-track lesions (defined as a maximum width of the HSL <1 mm larger than the glenoid track) and on-track lesions.
Statistical Analysis
Continuous data were presented as means with standard deviations. Patients were divided into the on-track and off-track groups based on the difference between the glenoid track and the maximum width of the HSL in millimeters. On-track was defined as a glenoid track greater than the maximum width of the HSL, while off-track was defined as a maximum width of the HSL greater than the glenoid track. The Mann-Whitney U test was used to evaluate the measured parameters between the 2 groups. Statistical analysis was performed using SPSS (Version 27.0; IBM). All the new measurement methods were created with the collaboration of fellowship-trained surgeons and research engineers (M.T.P, J.W.A, P.Go, P.Ga.).
Results
There were 48 right shoulders and 27 left shoulders represented. The mean age was 27.1 years (range, 18-48 years). Overall, 55 patients had a lesion defined as on-track, and 20 patients had a lesion defined as off-track. Additionally, 71 patients were male, and 4 were female. The imaging assessments were conducted by 2 fellowship-trained orthopaedic surgeons (M.T.P., J.W.A.). The variability in measurements between the reviewers was assessed via the intraclass correlation coefficient, which was 0.93 for HSL medialization, 0.86 for HSA, 0.90 for HSL width, and 0.81 for HSL volume. For calculation of the GBL, the intraclass correlation coefficient was 0.92.
There was no significant difference in age between the on-track and off-track groups (27.06 vs 27.40 years, respectively; P = .461). Off-track lesions had significantly more HSL volume (603.08 vs 433.61 mm3, respectively; P = .007), a greater mean HSL width (16.06 vs 11.53 mm, respectively; P = .001), and maximum HSL width (20.75 vs 14.68 mm, respectively; P < .001) than on-track lesions. Off-track lesions also had more HSL surface area (374.23 vs 272.64 mm2, respectively; P = .001) and more HSL medialization (14.96 vs 17.62 mm, respectively; P = .028) than on-track lesions. The mean HSL depth (1.89 vs 2.25 mm, respectively; P = .194) and maximum HSL depth (2.96 vs 3.33 mm, respectively; P = .495) were not significantly different between the on-track and off-track groups.
Lesions in the off-track group had greater GBL (22.55% vs 17.73%, respectively; P = .037), a greater GBL width (6.92 vs 3.58 mm, respectively; P < .001), and a greater GBL length (21.61 vs 16.1 mm, respectively; P = .015) than lesions in the on-track group (Table 1).
Humeral head lesions and glenoid bone loss comparasion amongst On-Track and Off-Track lesions a

GBL, glenoid bone loss; HSL, Hill-Sachs lesion. Data are presented as mean values.
Subgroup analysis was performed to evaluate large off-track lesions, defined as a maximum width of the HSL >1 mm larger than the glenoid track (n = 18), compared to borderline off-track lesions and on-track lesions (n = 57). Large off-track lesions had a greater HSA (33.16° vs 26.20°, respectively; P = .035) and a more superior extent of the HSL (4.50 vs 5.99 mm, respectively; P = .033) than borderline off-track and on-track lesions (Table 2).
Subgroup Analysis a

HSL, Hill-Sachs lesion. Data are presented as mean values.
Discussion
The principal findings of this study demonstrate that lesions classified as off-track were associated with larger GBL, had a more medialized HSL, and had a larger HSL width and surface area; additionally, the HSA was greater compared to on-track lesions. It has previously been established that the glenoid track concept is a strong predictor for recurrent instability. 19 However, there remains a paucity of literature on the importance of HSL morphology and its contribution to recurrent instability.5,8 Prior studies have shown that HSLs that extend more medially on the humeral head may increase the risk of recurrent instability and lead to worse clinical outcomes.17,20 The present study further characterized lesions that were more likely to be off-track and thus at risk for recurrent instability.
Both glenoid and humeral head bone loss have been shown to contribute to failure after glenohumeral instability treatment. As a result, the glenoid track concept has been described and adopted as the gold standard in identifying cases that are at risk for recurrent instability. 3 Arciero and colleagues 1 analyzed various sizes of both GBL and HSLs and concluded that combined defects have an additive negative effect on joint stability. A medium-sized HSL (1.47 cm3) and a 2-mm glenoid defect width represented significant risk factors for recurrent instability when only soft tissue Bankart repair was performed. 1 Similarly, a small HSL and a GBL width >4 mm posed the same risk for recurrent instability after soft tissue Bankart repair.
There is a debate in the literature on whether there is a direct correlation between HSL size and GBL. 1 A recent study showed that deeper HSLs are associated with smaller GBL and vice versa. 14 Yang and colleagues 21 compared patients with recurrent instability and off-track HSLs who underwent arthroscopic Bankart repair with remplissage versus the modified Latarjet procedure. That study concluded that both techniques can achieve similar patient-reported outcomes and similar rates of recurrent instability in patients with subcritical GBL, with the Latarjet group having higher complication rates. However, the Latarjet procedure was found to be more effective in revision surgery for instability and a better choice in contact athletes with >10% of GBL. 21
HSLs are further characterized by their location, angle, and overall presence within the glenoid track itself. Di Giacomo et al2,4 demonstrated that the location of the HSL depends on the arm position at the time of the initial dislocation. Patients whose arm was in an abducted position had a higher HSA, which predisposed them to a higher risk for recurrent instability. 2 Additionally, HSLs that are peripheral were associated with worse functional outcomes compared to central lesions. 20 The present study found that off-track lesions demonstrated more HSL medialization compared to on-track lesions. More specifically, our study identified borderline lesions and found that a greater superior extent of the HSL was more associated with large off-track lesions.
Although the glenoid track concept remains the gold standard for assessing the severity of bipolar lesions, our study identified simple parameters of an HSL that may be more practical to measure. Both HSL medialization and HSA were increased in off-track lesions. These characteristics may be easier to assess in clinical practice than the Hill-Sachs interval itself, all with the goal of appropriate clinical decision-making. For example, in cases in which there is intact cartilage between the HSL and rotator cuff footprint, less experienced providers may not account for that distance and only measure HSL width. This could underrepresent the size of the Hill-Sachs interval and, with that, the status of the glenoid track. Our findings are consistent with previous literature in that HSL medialization may be an important factor in understanding the risk of engagement and instability recurrence. 20 Gyftopoulos et al 7 measured HSL medialization with respect to the bicipital groove and found it to be significantly greater in patients with engagement. Similarly, Yamamoto et al 20 defined “peripheral track” lesions as those with more medial extension from the rotator cuff insertion and found these patients to have worse clinical outcomes. The present study corroborates these findings and further suggests that HSL medialization may be one of the most important parameters when considering the prognosis and treatment options for patients with bipolar bone loss.
While there has been a tremendous improvement in the diagnosis and treatment of bipolar bone loss, a recent expert consensus concluded that HSLs are still poorly quantified and classified by current imaging systems. 15 3D CT is widely recognized among experts as the most accurate way to assess both glenoid and humeral head bone defects and is most utilized to calculate the glenoid track.12,15 However, there remains a limited consensus on how to best characterize HSLs and evaluate their contribution to the recurrent instability risk. 15 The present study aimed to describe various radiological characteristics of HSLs that are associated with off-track bipolar lesions in the hope of better delineating their contribution to recurrent instability.
Limitations
The current study relied on data obtained from 3D CT. Although this is an extraordinarily detailed imaging modality with which to describe bone loss in shoulder instability, many surgeons use magnetic resonance imaging (MRI) alone when evaluating patients clinically. Certain parameters, such as HSL surface area and volume, would be more difficult to quantify from 2D imaging such as MRI. However, 3D reconstructions obtained from MRI have been shown to have equivalent accuracy to those obtained from CT, 21 thus making 3D renderings from MRI in normal clinical practice a feasible method to evaluate bipolar bone loss. The lack of MRI data in the present study also limits our ability to account for soft tissue defects that may contribute to recurrent instability. Further studies could incorporate bony morphology, soft tissue injuries, and patient factors to better establish a risk profile for patients with instability and help guide treatment accordingly.
Conclusion
Off-track lesions were found to have larger GBL, a larger HSL width, a more medialized HSL, greater HSL surface area, and a larger HSA. This study outlines the specific characteristics of high-risk bipolar bone loss lesions to simplify the identification of patients in a clinical setting and aid in appropriate treatment planning.
Footnotes
Final revision submitted September 27, 2024; accepted October 14, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.W.A. has received hospitality payments from Arthrex, Mid-Atlantic Surgical Systems, and Smith+Nephew; education payments from Mid-Atlantic Surgical Systems; and grants from Arthrex and DJO. C.B.R. has received grants from Arthrex and DJO and education payments from Smith+Nephew and MedInc of Texas. M.T.P. has received royalties from Anika Therapeutics, Arthrex, and Arthrosurface; consulting fees from Arthrex, Zimmer Biomet, and JRF Ortho; nonconsulting fees from Arthrex and Arthrosurface; education payments from Arthrex; and honoraria from Flexion Therapeutics and JRF Ortho. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Naval Medical Center San Diego (NMCSD.2005.0038).