
Abstract
Background:
Running-related overuse injuries are common among recreational runners; however, there is currently little prospective research investigating the role of running characteristics on overuse injury development.
Purpose:
To investigate the relationship between running characteristics and lower extremity musculoskeletal injury (MSKI).
Study Design:
Cohort study; Level of evidence, 2.
Methods:
The study included 827 incoming cadets of the class of 2020 at the United States Military Academy. Before cadet basic training, running spatiotemporal parameters (stride length, ground contact time, and cadence) were recorded for each participant, and foot-strike pattern was analyzed. Demographic data were recorded and analyzed as potential covariates. Lower extremity MSKIs sustained over the 9 weeks of cadet basic training were documented. Kaplan-Meier survival curves were estimated, with time to incident lower extremity MSKI as the primary outcome, by level of the independent predictor variables. Risk factors or potential covariates were carried forward into multivariate Cox proportional hazards regression models.
Results:
Approximately 18.1% of participants incurred a lower extremity MSKI resulting in ≥3 days of activity limitation during cadet basic training. Univariate analysis indicated that participants with the shortest stride length (<133.0 cm) were 39% more likely to incur any lower extremity MSKI and 45% more likely to incur an overuse MSKI than those with the longest stride length (>158.5 cm), and that participants with the longest ground contact time (>0.42 seconds) were twice as likely to incur any MSKI than those with the shortest contact time (<0.28 seconds). After adjusting for sex, weekly distance running 3 months before cadet basic training, and history of injury, multivariate regression analysis indicated that participants with the longest contact times were significantly more likely to incur overuse lower extremity MSKI than those with the shortest contact times (hazard ratio, 2.15; 95% CI, 1.06-4.37). There was no significant difference in risk of MSKI associated with foot-strike pattern or cadence.
Conclusion:
Study participants running with the longest ground contact times were 2.15 times more likely to incur an overuse lower extremity MSKI during cadet basic training than those with the shortest contact times. Also, study participants with the shortest stride length were 45% more likely to incur an overuse MSKI than those with the longest stride length.
Musculoskeletal injury (MSKI) related to running and fitness training is common in young athletic populations, with annual injury rates ranging from 19% to 79%. 41 Such injuries can lead to loss of playing time and productivity within this population. Similarly, lower extremity MSKIs due to fitness training are a primary source of injury and disability in the US military. 35 MSKIs accounted for 80% of all injuries across the US Army in 2016 and 65% of all medically nondeployable soldiers as of March 2019. 28 The majority of MSKIs in soldiers are overuse injuries, with incidence estimates ranging from 65% to 82%14,38; 36% of all overuse MSKIs in the military are related to marching and running.14,38 With running being the primary mode of physical endurance training within the US military and also very popular within the civilian population, it is important to understand the factors that may increase the risk of MSKI in order to develop and implement evidence-based injury prevention strategies.
Evidence suggests that nonmodifiable factors such as previous history of injury, sex, race, and foot posture may be associated with increased risk of training injury.19,26,27,33 Although these variables are important, modifiable risk factors should be the focus when the goal is implementing injury prevention strategies. Modifiable risk factors that may mitigate the risk of MSKI and running-related injuries include body mass index (BMI), running shoe characteristics, foot-strike pattern, cadence, ground contact time, and stride length.1,10,15,17,22,25,32,34,39
There have been a number of laboratory studies conducted indicating that modification of foot-strike pattern and running spatiotemporal variables such as stride length, contact time, and cadence can be associated with kinematic and kinetic changes that may reduce a runner’s risk of injury.1,8,11,15,18,22,25,34,42 In many cases, these results are used as a surrogate to explain injury risk. However, a Brindle’s systematic review and meta-analysis concluded that mean stride time, contact time, cadence, and stride length during running are not different between those with and without a history of overuse injury, highlighting the need for prospective studies to determine the role of these variables during running in overuse injury development.
The purpose of the current study was to prospectively investigate the relationship between lower extremity MSKI and running characteristics to include training volume, stride length, contact time, foot-strike pattern, and cadence.
Methods
Study Design and Setting
We conducted a prospective cohort study over a 9-week period at the United States Military Academy (USMA) to address the stated research questions. Data collection occurred in the summer of 2016 the study participants were cadets of the class of 2020 who were entering basic training at the USMA, and the primary outcome of interest was time to lower extremity MSKI while participating in cadet basic training. The protocol for this study was approved by our institutional review board. The methods for the current study have been described in detail elsewhere 17 ; however, key aspects of study design for the current analyses are presented in this section.
Study Participants
All 1308 incoming cadets of the class of 2020 were recruited into the study, and 78% (n = 1025) provided consent before preinjury baseline data collection. Of these 1025 cadets, all data were obtained for 827 cadets, who composed the final cohort. Baseline data collection took place during the cadets’ first week of enrollment at the academy, before the initiation of any physical training. Details related to participant inclusion in the study are illustrated in Figure 1.
The number of cadets who provided consent to participate (n = 1025), the number of participants with missing data (n = 198), and the total number of participants included in the final analysis (n = 827). Participants who dropped out of the study did so strictly due to missing data. USMA, United States Military Academy.
Participants included in the study were between the ages of 17 and 23 years and were deemed healthy and medically fit for military service before admission to the academy through the Department of Defense Medical Evaluation Review Board (DODMRB). The exclusion criterion was lower extremity or back injury within the previous 3 months; no incoming cadet was excluded from the study for this reason. Demographic data (age, sex, and race) were obtained within the USMA application process, while height and weight were recorded as part of the DODMRB process. These variables were recorded and evaluated to determine if it would be necessary to adjust for their influence, as other studies have shown that these variables, as well as history of injury, have been associated with increased risk of future injury.27,40,41
Baseline Data Collection
All participants were assessed before cadet basic training while wearing the Army physical fitness uniform, which consists of shorts, a t-shirt, and self-selected training shoes. A baseline questionnaire that assessed previous and current activity levels and injury history was administered to all study participants. For the purposes of this study, questions identifying those with a history of lower extremity MSKI and self-reported weekly distance running at 3 months before beginning cadet basic training were included in our analysis as potential confounding variables.
Running Spatiotemporal Parameters
Running biomechanics were evaluated using the OptoGait system (Version 1.11; Microgate) and a 2-dimensional high-speed video camera. All participants were asked to run approximately 60 m outside, over ground, on a concrete surface at their self-selected 2-mile (3.2-km) run pace, in their self-selected running shoes. At the 40-m mark, we asked participants to run through the OptoGait system, a movement analysis and functional assessment system equipped with optical sensors collecting at a frequency of 1000 frames per second (Hz). The OptoGait system has demonstrated high test-retest reliability while also being a valid instrument for the measurement of spatiotemporal gait parameters in healthy young adults. 21 The system consists of photoelectric cells sited along transmitting receiving bars of 1 m in length that can be extended to 10 m, with a maximum distance of 6 m between them. The transmitting and receiving bars contain infrared light-emitting diodes that enable communication between the 2 bars. When the participant passes between the transmitting and receiving bars, the system automatically calculates spatiotemporal parameters by sensing interruptions in communication. 21
Parameters collected for the purposes of this study were stride length (from left heel to right heel; in cm), contact phase duration (ie, ground contact time; in seconds), and cadence (ie, step rate; in steps/min). Data were saved within the OptoGait system using the participant’s study identification number. To operationally define stride length and contact time, the output associated with each variable was organized from least to greatest and then sorted into quartiles. For cadence, the participants were sorted into 2 groups: those who maintained a cadence ≥170 steps/min and those running at <170 steps/min. At the same time, foot-strike pattern was recorded by a high-speed video camera (Casio Exilim HS EX-ZR200) mounted to a Vivitar tripod (45-cm camera lens height, 130-cm distance from the OptoGait receiving bar). The camera sampled at 240 Hz with a resolution of 512 × 384 pixels and shutter speed of 1/1000 seconds. The camera was placed perpendicular to the 10-m OptoGait track, capturing sagittal plane video from the shoulder down to preserve the identity of the participants. A 20 × 14-cm white board, with the participant’s identification number written on it, was placed in the camera’s view at the beginning of each video and recorded to identify the runner in the video.
Running Foot-Strike Pattern
Windows Movie Maker 7.0 (Microsoft) was used to view each participant’s high-speed running video. The characterization of foot-strike pattern defined by Ogueta-Alday et al 30 was used to categorize the foot strikes into 2 groups: rearfoot strike (RFS) or nonrearfoot strike (NRFS). Location of initial plantar contact observed in the posterior one-third of the foot was considered an RFS. Location of initial plantar contact observed in the anterior two-thirds of the foot was characterized as an NRFS. If both anterior and posterior aspects of the foot made initial contact with the ground simultaneously, the foot strike was considered an NRFS. Each participant’s overall foot-strike pattern was determined by whichever characterization (RFS or NRFS) made up the majority of foot strikes in the video clip. Each video clip contained at least 1 left foot strike and 1 right foot strike.
Two medical professionals, a physical therapist (rater 1; not an author) and an athletic trainer (E.F.), evaluated the first 20 participant video clips independently, and the interrater reliability for grading foot-strike pattern was calculated. Both raters were experienced in the use of high-speed video for the evaluation of running mechanics, including but not limited to foot-strike pattern and cadence. Interrater reliability demonstrated a Cohen kappa value of 1, indicating perfect agreement for evaluating foot-strike pattern. After confirming interrater reliability, rater 1 evaluated the remaining participant videos and recorded data in a deidentified, password-protected Microsoft Excel spreadsheet.
Injury Surveillance
In general, all cadets receive medical care through the closed health care system at the USMA. All injuries are evaluated through its associated sports medicine and orthopaedic clinics. As a result, during cadet basic training, all MSKIs are evaluated by physical therapists at the USMA. All lower extremity MSKIs sustained by study participants during the 9-week period associated with cadet basic training were documented using the Armed Forces Health Longitudinal Technology Application as well as the Cadet Illness and Injury Tracking System.
In addition to this 9-week follow-up period after the baseline data collection, the 2-week period beyond the completion of cadet basic training was included to capture those cadets who might have received medical care shortly after the completion of training. Lower extremity MSKIs were operationally defined as those injuries occurring during basic training resulting in physical limitations for ≥3 days. We examined all incident lower extremity MSKIs during the follow-up period, to include both acute injuries and those due to an overuse mechanism. Injuries with an overuse mechanism were operationally defined as those with gradual onset secondary to repetitive microtrauma due to activities such as running or marching. Because of the closed health care system at our institution, our ability to detect any injuries during the follow-up period was excellent.
Statistical Analysis
Descriptive statistics were calculated to describe the sociodemographic characteristics (age, sex, height, BMI, and race) for each group. Means with standard deviations or medians with interquartile ranges (IQRs) according to normality were computed for continuous data, and frequency distributions were calculated for categorical data. The Shapiro-Wilk test was used to assess the normality of the data. Homogeneity of variance was assessed with the Levene test. Two-tailed independent t tests were used to assess between-group (injured vs noninjured during follow-up) differences for continuous data that met parametric assumptions (BMI, height, and age). The Pearson chi-square test was used to examine the association between injury and patient sex. R Version 3.1.2 (The R Project for Statistical Computing) and Stata Version 10.1 (StataCorp) were used to analyze these data.
Initially, Kaplan-Meier survival curves were estimated with time to incident lower extremity MSKI during the 9-week follow-up period as the primary outcome by level of the independent predictor variables (eg, stride length, contact time, foot-strike pattern, and cadence). Promising risk factors and known or potential covariates (sex, self-reported weekly distance running 3 months before cadet basic training, and history of injury) were carried forward into univariate and multivariable Cox proportional hazards regression models, which were used to estimate hazard ratios (HRs) and 95% confidence intervals for the independent variables of interest. For all analyses, P < .05 was considered the threshold for statistical significance.
Results
Of the 827 participants included within the final analysis, 633 (77%) were male and 194 (23%) were female. The mean age was 18.3 ± 1.0 years, while the mean BMI was 23.9 ± 2.9. Age and BMI were not significantly different between injured and uninjured participants; however, mean height differed significantly between groups (173.8 ± 9.5 [injured] vs 177.0 ± 8.3 cm [uninjured]; P < .001). The cumulative incidence of lower extremity MSKI during cadet basic training was 18.1% (n = 150), with 59% (n = 88) being overuse MSKI. The overall median time to any lower extremity MSKI was approximately 15 days (IQR, 7-23 days), while the median time to lower extremity overuse MSKI was approximately 10 days (IQR, 5-20 days). The number and type of injuries observed during the 9-week follow-up period are presented in Table 1.
Lower Extremity MSKI During the 9-Week Follow-up According to Anatomical Region a
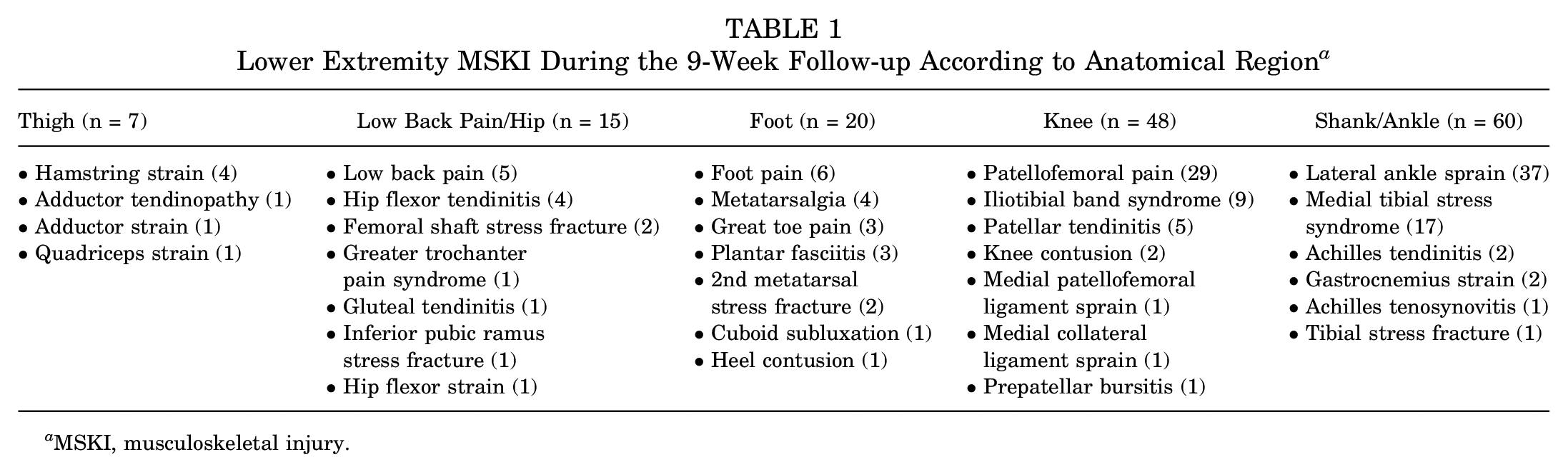
MSKI, musculoskeletal injury.
Univariate and Multivariate Analyses of Any Lower Extremity MSKI
The results of the univariate analysis are shown in Table 2. Our findings indicated that there was no significant association between foot-strike pattern and any MSKI during the 9-week follow-up period. Similarly, cadence was not found to be significantly associated with any MSKI.
Results of Univariate Analysis for Risk of Any Lower Extremity MSKI and Overuse MSKI a

MSKI, musculoskeletal injury; NRFS, nonrearfoot strike; RFS, rearfoot strike; HR, hazard ratio.
Statistically significant (P < .05).
As it related to stride length, univariate analysis indicated that participants with the shortest stride length (<133.0 cm) were at significantly greater risk of any MSKI during the follow-up period when compared with those with longer stride lengths (Figure 2). Specifically, those with the longest stride length (>158.5 cm) were 61% less likely to incur any MSKI (HR, 0.39; 95% CI, 0.25-0.62; P < .05) (Table 2). In the multivariable models, which adjusted for the influence of sex, weekly distance running 3 months before basic training, and history of injury, participants with the longest stride length were 39% less likely to incur any MSKI than those with the shortest stride length (HR, 0.61; 95% CI, 0.37-1.01; P≥ .05) (Table 3).

Kaplan-Meier survival curve of the risk of any lower extremity musculoskeletal injury (MSKI) during cadet basic training according to stride length.
Univariate analysis also indicated that participants with longer contact times were at greater risk of any lower extremity MSKI when compared with participants with shorter contact times (Figure 3). Participants with the longest contact time (>0.42 seconds) were twice as likely to incur any MSKI than those with the shortest contact time (<0.28 seconds) during cadet basic training (HR, 2.17; 95% CI 1.33-3.54; P < .05) (Table 2). The association between contact time and any lower extremity MSKI during the follow-up period was dose dependent (Figure 3). After adjusting for covariates in the multivariable models, those with the longest ground contact time were 1.42 times more likely to incur any MSKI during cadet basic training (95% CI, 0.86-2.36; P≥ .05).
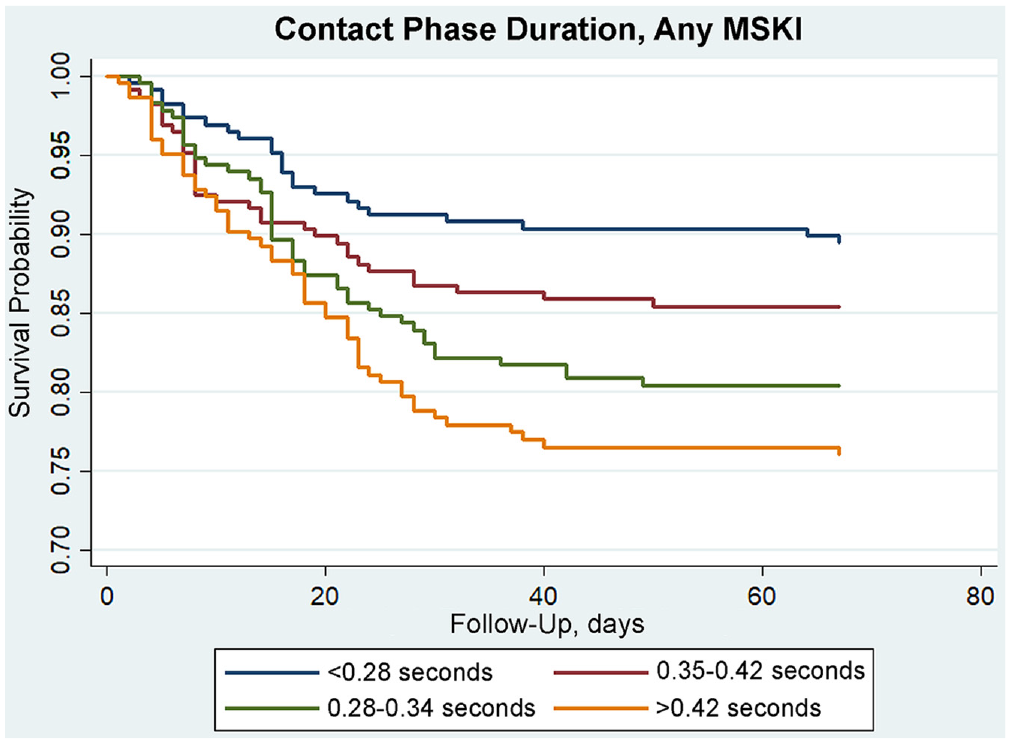
Kaplan-Meier survival curve of the risk of any lower extremity musculoskeletal injury (MSKI) during cadet basic training according to duration of contact phase.
Univariate and Multivariate Analysis of Overuse Lower Extremity MSKI
Consistent with the analysis of all MSKIs, there was no significant association between foot-strike pattern or cadence and lower extremity overuse MSKI during the follow-up period in the univariate models (Table 2). Participants with the longest stride length (>158.5 cm) were 59% less likely to incur an overuse MSKI over the follow-up period compared with those with the shortest stride length (<133 cm) (HR, 0.41; 95% CI, 0.23-0.74; P < .05). After adjusting for covariates, multivariate analysis indicated that participants with the greatest stride length were 45% less likely to incur an overuse MSKI versus those with the shortest stride length (HR, 0.55; 95% CI, 0.29-1.03; P≥ .05) (Table 3).
Results of Multivariate Analysis for Risk of Any Lower Extremity MSKI and Overuse MSKI a
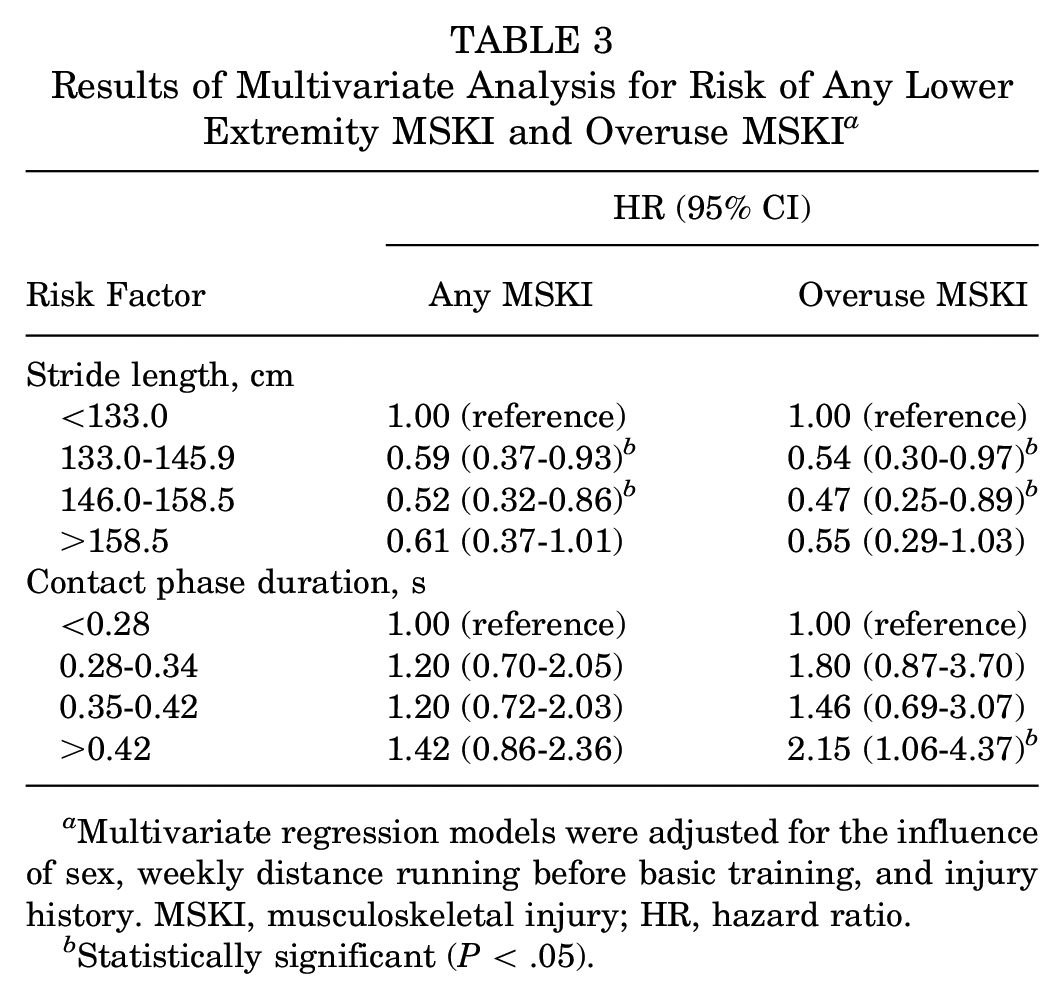
Multivariate regression models were adjusted for the influence of sex, weekly distance running before basic training, and injury history. MSKI, musculoskeletal injury; HR, hazard ratio.
Statistically significant (P < .05).
Based on univariate analysis, participants with the longest ground contact times (>0.42 seconds) were 3.07 times (95% CI, 1.54-6.11; P < .05) more likely to incur an overuse MSKI during cadet basic training than those with the shortest ground contact times (<0.28 seconds). The significant findings were carried over into the multivariate models even after adjusting for the influence of sex, weekly distance running before basic training, and injury history, with participants with the longest ground contact times being 2.15 times (95% CI, 1.06-4.37; P < .05) more likely to incur an overuse MSKI injury during the follow-up period when compared with those with the shortest contact times.
Discussion
The primary purpose of this study was to examine whether running characteristics, including foot-strike pattern, cadence, contact time, and stride length, were associated with lower extremity MSKI among cadets during basic combat training. Our results suggested that participants with the shortest ground contact times were at a significantly reduced risk of overuse lower extremity MSKI over the course of cadet basic training when compared with those with the longest contact times, regardless of sex, prior distance running, or history of injury (HR, 2.15; 95% CI, 1.06-4.37). Also, those cadets with shorter stride lengths were at greater risk of any lower extremity MSKI as well as overuse lower extremity MSKI. Though all findings were not statistically significant, the magnitude of the increased risk should be considered. There was no significant association between lower extremity MSKI and foot-strike pattern or cadence on univariate or multivariate analysis.
Numerous laboratory studies have observed changes in kinetic, kinematic, and spatiotemporal variables indicating that adoption of a shorter stride length would minimize vulnerability to MSKI.16,23,42 However, the meta-analysis by Brindle et al 4 concluded that stride length was not consistently different between runners with or without a history of overuse injury. The systematic review included a prospective cohort study of >200 novice runners, finding no difference in stride length between injured and noninjured male and female runners at 2 fixed speeds (2.5 and 2.8 m/s). 3 Interestingly, within the current study, cadets with the shortest stride lengths had the greatest risk of lower extremity MSKI. A 5-fold larger sample size in the current study, population divergence (military basic trainees vs novice runners), differences among variable quantification methods (OptoGait vs instrumented treadmill), and differing running instruction methods (fixed speed vs self-selected speed) may explain the varied results among studies. Additionally, Bredeweg et al 3 relied on self-reported injuries, which were fewer in number compared with the current study, within which injuries were diagnosed by a physical therapist in a closed health care system.
Our results may also be explained to some extent by the relationship of stride length with contact time and running velocity. The laboratory study by García-Pinillos et al, 12 which investigated the effect of running velocity on spatiotemporal variables in male endurance runners, observed increased stride length and decreased contact time as running velocity increased. This observation is not novel, as Cavanagh and Kram 5 noted this as an established curvilinear relationship over the entire velocity range, with stride length reaching a plateau at greater velocities, much greater than those typically attained by endurance runners. An example of the contribution of stride length and cadence to increased velocity is highlighted in the increase in velocity from 3 to 4 m/s, which includes an approximate 28% increase in stride length while only requiring a 4% increase in cadence. Moreover, when fatigue occurs in elite runners, speed decreases primarily as a function of stride length, indicating that runners who maintain longer stride lengths over the duration of a run are likely the ones with greater aerobic endurance. 5 Low aerobic fitness has been established in the literature as a significant risk factor for overuse injury. 27 Also, in the laboratory study by Lieberman et al, 23 investigating the effect of variable cadences on running economy, kinematics, and kinetics, the authors highlighted the importance of looking specifically at the distance of the foot from the hip and the knee. They reported that participants who extended their stride length through hip flexion rather than knee extension at the end of the swing phase had a nearly vertical tibia, minimizing rates and magnitudes of impact peak. 23 This observation indicates that we should consider more than stride length alone as it relates to injury risk and rather break down distance of foot from the knee and the hip as well. Also, we acknowledge that anthropometry, particularly participant height, is a component that limits one’s ability to modify stride length despite its influence on risk of MSKI.
In the current study, we observed that participants with an NRFS pattern during running at preinjury baseline were 36% less likely to sustain a lower extremity overuse MSKI during the follow-up period; however, this finding was not statistically significant. Studies investigating the risk of injury associated with foot-strike pattern to date have yielded conflicting results, although laboratory studies have indicated that an RFS pattern results in significantly greater shock attenuation by the lower extremity, greater mean vertical loading rates, greater peak hip adduction, increased patellofemoral loading, and increased knee abductor moment.13,20 There has been some indication of the types of injuries that are more often observed in individuals who maintain an RFS running pattern compared with an NRFS pattern. Those individuals with an RFS pattern might be more susceptible to hip and lower back pain, patellofemoral pain, increased anterior compartment pressures, and tibial stress injury, while those who maintain an NRFS pattern might be more susceptible to foot and ankle injury.7,13,36,42 As with many previous studies investigating this relationship, we were limited by the number of individuals who exhibited an NRFS pattern at preinjury baseline (11%), which may have limited our ability to observe a difference in injury risk between groups if it did exist.
Running cadence has recently garnered a great deal of attention in clinical and performance improvement settings. Previous research conducted in a laboratory setting indicates that an increase in cadence during running is associated with reduced ground-reaction forces, vertical oscillation, and joint loads.22,42 In the current study, we did not observe a significant difference in cadence between the injured and noninjured groups (mean, 168.77 vs 169.72 steps/min, respectively). Our results align with other studies directly investigating the relationship between injury risk and cadence.6,11,37 However, the current body of literature is conflicting, as high school cross-country runners with the lowest step rates during running at both fixed and self-selected speeds had a greater likelihood of shin injury. 24
Participants with the longest-duration ground contact times (>0.42 seconds) were at greatest risk of lower extremity overuse MSKI in the current study. Presently, there is no consensus in the literature regarding the influence of contact time on injury risk. Bredeweg et al 3 observed no association between contact time and running-related injury in a mixed group of male and female novice runners at fixed speeds. When male and female runners were analyzed separately, male runners who incurred a lower extremity injury had approximately 10% shorter contact times (mean, 0.21 seconds) than their uninjured counterparts (mean, 0.24 seconds) running at a velocity of 2.5 m/s. 3 Interestingly there was no difference in contact times between the same injured and uninjured male runners when running at faster speeds (2.7 m/s). Runners in the current study ran at a mean self-selected pace of 4.4 m/s, which may account for the contrasting study results. The relationship between shorter contact time and increased injury risk may be a result of increased maximal lower extremity stiffness. Leg stiffness strongly influences contact time and has been identified as being a prospective risk factor in those runners later diagnosed with an overuse injury compared with uninjured runners.4,9,29 To our knowledge, there has been no research examining the direct effect of leg stiffness on the incidence of running-related MSKI.
Limitations and Strengths
As with similar studies, there were limitations with the current study that should be considered when interpreting the results. We only observed spatiotemporal variables over a 10-m distance within the latter part of a 60-m run. Future studies might consider monitoring cadence over an entire run or, in this case, over the entirety of cadet basic training and analyzing the mean step rate while also appreciating variability in step rate throughout. Also, the data presented may not be an accurate representation of true running characteristics while running longer distances. For example, participants within the current study ran at a rate of approximately 4.4 m/s whereas previous studies often include rates of ≤4.0 m/s.2,4 Previous research indicates that changes in running speed influence kinetics and kinematics at the hip, knee, and ankle, which could produce contrasting observations within other similar studies.26,31 Although we attempted to recruit all 1308 cadets within the incoming class, we successfully recorded all data on 827 cadets. With that said, there were only 150 total injuries, with 88 (59%) of those being overuse injury in the 827 participants with complete data. The limited number of observed overuse injuries likely limited our statistical power, making it more difficult to observe differences related to overuse injury. Also, only approximately 11% of cadets included within our study exhibited an NRFS pattern, making it difficult to observe a difference in the risk of injury if it did exist within our analysis of foot-strike pattern.
Even though we were only able to observe a limited number of lower extremity overuse MSKIs, we conducted a large-scale prospective cohort study within a closed health care system. This distinguishes the current study from the few prospective studies that have directly examined injury outcomes and allowed us to gather accurate information on the population of interest from baseline to injury in order to calculate accurate survival estimates.
Conclusion
In the current study, participants running with the longest ground contact time (>0.42 seconds) were 2.15 times more likely to incur an overuse lower extremity MSKI during cadet basic training than those with the shortest contact time (<0.28 seconds). Also, study participants with the shortest stride length (< 133.0 cm) were 45% more likely to incur a overuse lower extremity MSKI than those with the longest stride length (> 158.5 cm). Our observations have important clinical implications related to guidance for patients looking to minimize their risk of lower extremity MSKI through modification of running spatiotemporal variables.
Footnotes
Acknowledgements
The authors acknowledge LTC(Ret) Michael Johnson, LTC(Ret) Mike Crowell, Amy Weart, CDR Mark Riebel, LTC Daniel Watson, LTC Rob Halle, LTC Eliza Szymanek, Dr. Brian Stoltenberg, and the physical therapy staff at Keller Army Community Hospital. This research was also supported by the Uniformed Services University of the Health Sciences, Department of Physical Medicine & Rehabilitation, Musculoskeletal Injury Rehabilitation Research for Operational Readiness (MIRROR) (HU00011920011).
Final revision submitted March 22, 2024; accepted May 2, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Keller Army Community Hospital (ref No. 13-011).