
Abstract
Background:
Young female patients undergoing hip arthroscopy have an increased prevalence of baseline capsular laxity of the hip joint. This laxity, along with superimposed postoperative iatrogenic capsular deficiency secondary to an unrepaired capsule, could potentially lead to worse outcomes after arthroscopic treatment of femoroacetabular impingement (FAI) in this population.
Purpose:
To compare outcomes and revision rates for young female patients undergoing hip arthroscopy for FAI and labral tear with capsular closure (CC group) versus capsular nonclosure (CNC group).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review of prospectively collected data of patients who underwent index hip arthroscopy using interportal capsulotomies by a single surgeon between January 2014 and February 2020 was performed. Female patients aged 12 to 21 years who underwent hip arthroscopy with cam or pincer osteoplasty and labral repair with a 2-year minimum follow-up were included. The Beighton score was assessed. The Hip Outcome Score–Activities of Daily Living (HOS-ADL) and Hip Outcome Score–Sport-Specific Subscale (HOS-SSS) were obtained preoperatively and at 3 months, 1 year, and 2 years postoperatively. Data were analyzed using the Mann-Whitney U test and Fisher exact test.
Results:
A total of 23 hips (20 patients) were included in the CC group and 17 hips (16 patients) were included in the CNC group. The groups were not different regarding characteristics and preoperative patient-reported outcome scores. At all follow-up intervals postoperatively, the CC group scored significantly higher HOS-ADL and HOS-SSS. Fifteen of 17 (88.2%) patients in the CC group returned to sports versus 8 of 14 (57.1%) in the CNC group (P = .03). Four (17.4%) hips in the CC group had revision surgery compared with 9 (52.9%) hips in the CNC group (odds ratio, 5.1; 95% CI, 1.2-22.5; P = .02).
Conclusion:
Young female patients treated with CC while undergoing arthroscopic FAI had improved outcomes, fewer revisions, and a higher return-to-sports rate than those treated without CC.
Keywords
Femoroacetabular impingement (FAI) has become an increasingly well-recognized source of hip pain. Although patients from all demographics can be affected, FAI is most commonly seen in physically active individuals, particularly younger female patients. 39 The use of hip arthroscopy in treating FAI has become widely prevalent with acceptable complication rates and improvement in baseline function in adults as well as adolescents.3,31 Although complication rates and patient-reported outcomes in hip arthroscopy for FAI have been favorable, proper surgical technique is essential to optimize surgical outcomes.
As with many procedures, proper patient selection has been associated with outcomes of FAI.11,18,40 Several studies have evaluated the role of sex and consistently demonstrated worse outcomes among female patients.7,34,40 Specifically, in a cohort of adolescent patients undergoing hip arthroscopy for FAI, Menge et al 30 demonstrated significantly worse modified Harris Hip Scores as well as higher rates of reoperation in female patients when compared with an age-matched male cohort. Although female patients did experience significant improvement postoperatively, reasons for the discrepancy in overall improvement when compared with the male cohort are not fully understood. The effect of age on arthroscopic management of FAI has also been investigated. Although hip arthroscopy is successful in various age groups, middle-aged and older adults have been shown to improve to a lesser degree when compared with their younger counterparts and have a higher conversion rate to total hip arthroplasty (THA). 24 Anatomic factors have also been shown to affect FAI outcomes, as patients with acetabular overcoverage, excess acetabular retroversion, or increased femoral anteversion are at risk for less favorable outcomes.13,20
The success of hip arthroscopy in managing FAI is also affected significantly by surgical technique. Specific to the labrum, repair has demonstrated superior outcomes when compared with debridement.2,11,21 As the labrum helps to restore suction seal of the hip, debridement is thought to interfere with the hip's ability to protect against postoperative microinstability.2,6 A recent topic of debate has revolved around hip capsule management. It has been established that hip stability is largely dependent on the capsule's role in ensuring rotational, translational, and axial stability. 43 Accordingly, without capsular closure (CC), the hip joint may be subject to recurrent microinstability or even frank dislocation.10,27,29,33 Despite considerable investigation, it remains unclear whether full, partial, or no capsular repair is clinically superior.1,12,15,25 While some studies have demonstrated better outcomes with CC, others have been inconclusive or demonstrated the contrary.1,12,14,15,25,40
Research continues to advance toward improving the outcomes of arthroscopic management of FAI. The contribution of capsular deficiency to hip microinstability and its associations with patient outcomes is an area of ongoing interest with a lack of consensus. It is particularly important to analyze female patients in this area given their increased predisposition to FAI in addition to more prevalent baseline capsular laxity. 22 It is possible that this laxity could be worsened by postoperative iatrogenic capsular deficiency secondary to an unrepaired capsule. The purpose of this study was to compare outcomes and revision rates in young females with arthroscopically treated FAI and labral tear with CC versus capsular nonclosure (CNC). The authors hypothesized that female patients undergoing CC would have improved postoperative outcomes when compared with those who did not.
Methods
Institutional review board approval was obtained, and a retrospective review of prospectively collected data of patients who underwent hip arthroscopy for FAI was conducted. Index hip arthroscopy occurred between January 2014 and February 2020 by a single fellowship-trained surgeon (K.J.E.). Patients were included if they were female, were 12 to 21 years of age, and underwent hip arthroscopy with femoral and/or acetabular osteoplasty with associated labral repair in the setting of FAI. Exclusion criteria included patients <12 and >21 years of age, male sex, lateral center-edge angle <19°, existing rheumatological condition, and prior hip surgery. Both groups were treated as intention to treat to limit attrition bias in the revision setting.
Demographics from each patient were collected along with patient Beighton scores. Hip Outcome Score–Activities of Daily Living (HOS-ADL) and HOS–Sport-Specific Subscale (HOS-SSS) were collected preoperatively and at 3 months, 1 year, and 2 years postoperatively. Outcome scores were also collected at 1 year and 2 years postrevision if applicable. These outcomes scores have been previously validated to assess hip function after hip arthroscopy. 28 The minimal clinically important difference (MCID) and Patient Acceptable Symptom State (PASS) were evaluated 2 years after the index surgery.19,23
Return to sports was defined as the ability to compete in the same sport for at least a season without reinjury to the operated hip.
Surgical Technique
Each patient underwent standard hip arthroscopy in the lateral position under general anesthesia. The patient was placed in the lateral decubitus position and stabilized using a bean bag with the operative leg up. A lateral hip distractor (Smith+Nephew) was used for distraction, with a well-padded traction boot on the operative leg. The nonoperative leg was left free. All bony prominences were well padded. Anterior and anterolateral portals were created with fluoroscopic assistance. Viewing from the anterolateral portal, the surgeon performed an interportal capsulotomy to allow for improved visualization and working space within the hip. All patients in the study underwent labral repair using Arthrex Knotless SutureTaks. Between 2 and 5 anchors were used for all labral repairs, depending on the size of the lesion. The number of anchors used was determined by the senior surgeon performing the procedure and typically included 3 to 5 anchors. Once the labral repair was completed, a No. 2 FiberWire (Arthrex) was placed in the anterior and posterior aspects of the distal leaflet of the capsulotomy and used to retract the capsule to allow visualization of the femoral head-neck junction once the hip was taken off traction. A distal anterolateral accessory portal was created under direct visualization to perform the femoral osteoplasty. The femoral osteoplasty was then performed without traction using a 4-mm or 5.5-mm burr depending on the size of the cam morphology, consistent with the technique previously described in the literature. 26 Appropriate bone removal was confirmed under fluoroscopy. In the CC group, the interportal capsulotomy was closed using 2 No. 2 FiberWire sutures placed in an interrupted fashion with assistance from a suture-passing device. The patients in the CNC group did not have any part of their capsule closed.
Rehabilitation
Postoperative rehabilitation protocols were identical between the 2 treatment arms. Patients were 50% weightbearing for 2 weeks, after which they were progressed through low-resistance exercises. After demonstrating proper muscle firing patterns, patients began to increase muscle strength and advance toward full range of motion beginning at postoperative week 4. Throughout weeks 4 to 7, patients were encouraged to bear weight as tolerated and were graduated through increasingly demanding single- and double-leg exercises. Beginning at postoperative week 8, patients were cleared to start jogging and agility exercises with gradual progression. Sport-specific training was initiated at postoperative week 12. Return-to-play criteria included pain-free range of motion, hip strength >90% of the contralateral side, and ability to perform sport-specific drills without pain. Athletes were released to play by the senior surgeon. Braces were not required by the operating surgeon.
Statistical Analysis
Statistical analysis was performed using BlueSky Statistics Version 6.30 (Bluesky Statistics). Numeric variables determined to be normally distributed by the Shapiro-Wilk test were evaluated using a t test for 2 independent samples. Otherwise, nonparametric data were evaluated using the Mann-Whitney U test. Categorical variables were analyzed with a Fisher exact test. Odds ratios were calculated to quantify the strength of association between treatments and outcomes. A p-value of <.05 was considered significant.
Results
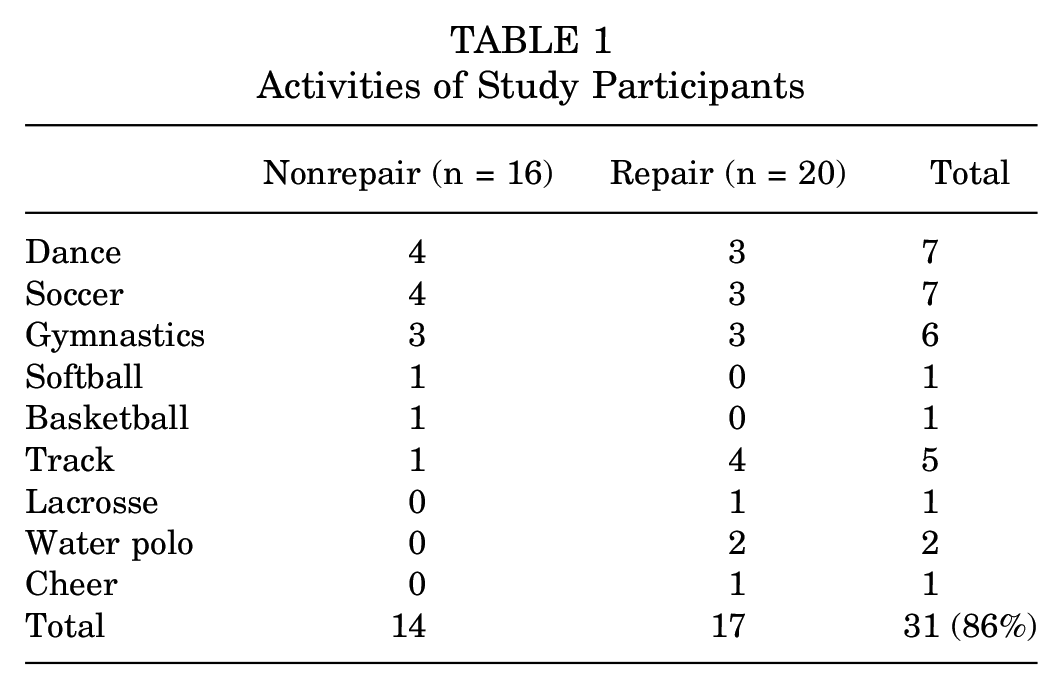
A total of 867 total hip arthroscopies were performed during the study period by the senior surgeon. A total of 408 patients were excluded from the study because they were male; furthermore, 119 patients were excluded due to being a revision case, 62 for severe dysplasia (lateral center-edge angle <19°), 23 for rheumatological conditions, 13 for previous slipped capital femoral epiphysis, and 198 for being out of the age range of 12 to 21 years. This left 44 patients; however, 8 more patients were excluded for not having preoperative and/or 2-year follow-up data, leaving a total of 36 patients and 40 hips in the study. Seventeen hips (16 patients) were included in the CNC group and 23 hips (20 patients) were included in the CC group. A total of 36 patients were treated. No patients were lost to follow-up. The minimum time to follow-up was 24 months and the mean time to follow-up was 35.8 ± 11.4 months (range, 24-60 months). The mean final follow-up in the CC group was 32.3 months, while the mean final follow-up in the CNC group was 38.7 months. All index procedures performed on the CNC group occurred between January 2014 and September 2015. All index procedures performed on the CC group occurred between October 2015 and December 2016. Of the 36 patients in the study, 31 (86%) participated in sports (Table 1). Dance and soccer were the most represented, with 7 athletes each, followed by gymnastics with 6 athletes. No significant difference in age (P = .387), body mass index (P = .11), or joint laxity based on Beighton scores (P = .794) was found between the 2 study arms (Table 2).
Activities of Study Participants
Patient Characteristics and Pertinent Surgical Measures a

ALAD, acetabular labrum articular disruption; BMI, body mass index; CC, capsular closure; CNC, capsular nonclosure; LCEA, lateral center-edge angle; LT, ligamentum teres; Preop, preoperative; Postop, postoperative; Q, quartile.
There were no other notable differences between the 2 treatment groups regarding patient characteristics and pertinent surgical measures (Table 2). Preoperative HOS-ADL and HOS-SSS were not significantly different between the 2 groups (P = .70 and P = .55, respectively). At 1 year and 2 years postsurgery, the CC group scored significantly higher on HOS-ADL. The 1-year mean score of the CC group was 85.9 ± 2.8, while that of the CNC group was 78.0 ± 5.5 (P < .001). At 2 years, the mean score was 87 ± 3.5 for the CC group and 79.9 ± 5.0 for the CNC group (P = .001). The final HOS-ADL remained significantly higher in the CC group as well (P = .007). For HOS-SSS, the repair group performed better at all time points. At 3 months, the CC group scored 64.7 ± 6.5 while the CNC group scored 55.7 ± 8.3 (P = .004). At 1 year, the CC group scored a mean of 83.7 ± 2.4 while the CNC group scored 77.6 ± 6.0 (P = .007). This difference persisted to 2 years (P = .004) and the final follow-up (P = .03) (Figures 1 and 2).

Hip Outcome Score–Activities of Daily Living between capsular closure (CC) and capsular nonclosure (CNC) groups. FU, follow-up.

Hip Outcome Score–Sport-Specific Subscale between capsular closure (CC) and capsular nonclosure (CNC) groups. FU, follow-up.
Clinically relevant and patient-relevant measures were evaluated as well (Table 3). Fifteen of 17 (88.2%) patients in the CC group returned to sports for at least 1 season without recurrent injury to the ipsilateral hip versus 8 of 14 (57.1%) cases in the CNC group (P = .03).
MCID and PASS for HOS-ADL and HOS-SSS at 2 Years a

Data exclude revisions. Data are presented as n(%). CC, capsular closure; CND, capsular nonclosure; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sport-Specific Score; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State. Blank cell indicates unable to perform comparison as both groups were 100%.
The MCID for HOS-ADL was met by all patients at the final follow-up. Ten (52.6%) patients achieved PASS in the CC group, whereas only 1 (12.5%) in the CNC group achieved the PASS for HOS-ADL. The MCID for HOS-SSS was met by 19 (100%) patients in the CC group compared with 6 (75%) in the CNC group. Eighteen (94.7%) patients in the CC group reached the PASS for HOS-SSS, while only 5 (62.5%) patients in the CNC group reached the PASS for HOS-SSS.
Adverse outcomes were also analyzed. Although these patients were too young to be converted to THA, some did undergo revisions. In the CC group, 4 (17.4%) patients went on to revision surgery compared with 9 (52.9%) in the CNC group (Table 4).
Revision Surgery Performed a

CC, capsular closure; CNC, capsular nonclosure.
Patients in the CNC group experienced increased odds of revision (odds ratio, 5.1; 95% CI, 1.2-22.5). Revision occurred at a mean of 9.2 months after the index procedure (Table 5). The reason for revision was recurrent or continued pain with associated labral tear, capsulolabral adhesions, and/or instability.
Characteristics of Patients Requiring Revision and Outcome Scores After Revision a

CC, capsular closure; CNC, capsular nonclosure; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sport-Specific Subscale; Preop, preoperative.
Revision labral repair and CC were performed in all cases of revision arthroscopy. Revision femoral osteoplasty was performed in 2 (22% of revision cases) of the CNC group revision cases and 1 (25% of revision cases) of the CC group revision cases. All patients reached the MCID for HOS-ADL 2 years after revision. However, only 1 of 13 patients achieved the PASS for HOS-ADL. Twelve of 13 patients obtained the MCID for HOS-SSS 2 years after revision, but only 5 of 13 met the PASS for HOS-SSS (Table 5). When including postoperative revision scores at the final follow-up, the CNC group scored 80.5 ± 4.9 and the CC group scored 85.7 ± 3.9 on HOS-ADL (P = .007) (Figure 1). For HOS-SSS, the CNC group scored 79.5 ± 7.3 and the CC group scored 83.8 ± 3.8 (P = .17) at the final follow-up (Figure 2). Thus, when revisions were included in analysis of all patients, 100% reached the MCID for HOS-ADL and 92.5% reached the MCID for HOS-SSS at the final follow-up.
Six patients in each group were considered hypermobile (Beighton score ≥5). In the CNC group, 4 (66.67%) of the hypermobile patients required revision. In the CC group, only 1 (16.67%) of the hypermobile patients required revision. This produced an odds ratio of 10 (95% CI, 0.6-154.4; P = .79) when subgroup analysis was performed on hypermobile patients.
Discussion
This study found that young female patients treated with CC while undergoing hip arthroscopy for FAI had improved outcomes, fewer revisions, and greater return-to-sports rates compared with those treated without CC. Clinically significant improvements were seen in both the CC and CNC groups from preoperatively to postoperatively; however, HOS-ADL and HOS-SSS were significantly greater in the CC group compared with the CNC group at 1 and 2 years postoperatively.
The overall percentages of patients achieving the MCID for HOS-ADL and HOS-SSS were 100% and 92.5%, respectively. These included patients without CC and those undergoing revision. These percentages are greater than the reported outcomes in other publications reporting outcomes in male and female adolescents. In the male and female adolescent population, Menge et al 30 reported that 97% and 91% of patients reached the MCID for HOS-ADL and HOS-SSS, respectively. Additionally, Cvetanovich et al 8 reported that 81% and 97% reached the MCID for HOS-ADL and HOS-SSS, respectively. Nwachukwu et al 37 reported that 79% and 85% reached the MCID for HOS-ADL and HOS-SSS, respectively, in a mixed adolescent population. Furthermore, specifically in the adult population, Nho et al 36 found that only 73% of adult patients reached the MCID for HOS-ADL. These outcomes were specific to primary procedures and did not include revision hip arthroscopies.
Bolia et al 1 found that all-comers >18 years of age undergoing hip arthroscopy for FAI had improved HOS-ADL and HOS-SSS postoperatively if they underwent CC versus nonclosure. They also found that the CNC group was 6.8 times more likely to require conversion to THA during the study period. 1 Similarly, while both the CC and CNC groups in the present study had improved HOS-ADL and HOS-SSS postoperatively that met the MCID, the CC group had significantly better improvement than the CNC group. While the present study did not use THA as a revision outcome, the CNC group was 5.1 times (95% CI, 1.2-22.5 times) more likely to undergo revision hip arthroscopy. This smaller number of revisions may be because of the shorter follow-up interval in the present study. It may also represent a trend that adolescents have better outcomes overall after hip arthroscopy compared with adults.
The capsule is an important static stabilizer of the femoroacetabular joint. 35 Thus, it would be expected that anatomic closure results in improved stability after capsulotomy. Jimenez et al 16 found that CC improved hip stability over CNC, in a systematic review of 24 biomechanical studies performed on hip capsule integrity in various states of repair. In patients with hypermobility, CC after hip arthroscopy may be especially important for maintaining hip stability postoperatively. These patients tend to have thinner hip capsules 9 and impaired connective tissue repair mechanisms even in the absence of genetic findings.5,45 This is concerning for at-risk populations such as young female athletes. Studies have shown magnetic resonance imaging evidence of restored capsular tissue and thickness after capsulotomy without CC after hip arthroscopy.17,44 The quality and the restored resting length of the repaired capsule were unclear. In this regard, hypermobile patients may have an impaired healing response. Because of connective tissue dysfunction in these patients, the capsular defect created by the capsulotomy may not heal with adequate quality or tension after hip arthroscopy. Thus, this population may benefit more from CC after hip arthroscopy. In the present study, a subgroup analysis was performed on patients with hypermobility that found the hypermobile group was 10 times more likely to undergo revision hip arthroscopy if their capsule was not closed at the time of surgery. However, this finding was not statistically significant, likely because of the small number of patients included in the subanalysis. However, this is a substantial trend that should not be dismissed. The authors strongly recommend closing the capsule for all young female patients with hypermobility undergoing hip arthroscopy.
In a systematic review, O’Connor et al 38 showed a return-to-sports rate after hip arthroscopy of 84.6%. In a cohort of male and female patients aged 13 to 23 years, Mohan et al 32 reported a return-to-play rate of 92% in amateur athletes. Chen et al 4 found a return-to-sports rate of 84.9% in athletic adolescents aged 10 to 19 years. The present study found similar rates in the CC group, at 88.2%. However, this rate was much lower in the CNC group at just 57.1%. Overall, this study had a return-to-sport rate of 74%. The difference in overall rate of return to sports is likely confounded by the poorer outcomes in the CNC group. This may also be because females tend to have inferior outcomes after hip arthroscopy. The cited studies did not report the return-to-sports rate for females specifically; thus, a fair comparison cannot be made.4,32,38
Limitations
Limitations of this study include the retrospective nature, relatively short follow-up, small sample size, and narrow inclusion criteria. These limitations may result in selection bias. Additionally, the patients undergoing CNC had their surgeries performed earlier in the study than the CC group. It is possible that advances in technique or surgeon skill between the 2 time periods could be a potential confounder; however, the senior surgeon had already completed >400 hip arthroscopies in his practice at the onset of the study. The surgeon changed his approach to this population in response to his experience, and CC was thought to be a better option for these patients. Comparative studies that include a historical control group have been shown in other studies to overestimate the treatment outcomes when compared with randomized controlled trials.41,42 This is 1 factor in the small sample size of the present study. However, the fact that all patients after a particular time point underwent CC eliminates selection bias regarding which patients received the intervention. The narrow inclusion criteria lend themselves to limiting confounding factors in patient characteristics and surgical procedures that can affect clinical outcomes. While the narrow inclusion criteria limit this study's generalizability, it gives improved insight into a population that has historically been found to have worse outcomes with a higher risk of revision surgery after hip arthroscopy.
Conclusion
This study found that young female patients treated with CC while undergoing hip arthroscopy for FAI had improved outcomes, fewer revisions, and a higher return-to-sports rate compared with those treated without CC.
Footnotes
Final revision submitted April 26, 2024; accepted May 16, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.S.M. has received education payments from ImpactOrtho, a grant from Stryker, and education payments from Goode Surgical. K.J.E. has received speaking fees and education fees from Arthrex Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from an WIRB Copernicus Group Company (20183142).