
Abstract
Background:
Anterior cruciate ligament (ACL) reinjury risk is high in young athletes, with graft failure rates as high as 23%. The optimal autograft choice to minimize reinjury risk in this population is unclear.
Purpose:
To compare graft failure rates between bone–patellar tendon–bone (BPTB), hamstring tendon (HT), and quadriceps tendon (QT) autografts in patients aged ≤18 years with a minimum follow-up (FU) of 24 months.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review of the literature between database inception and March 2022 encompassed PubMed/MEDLINE, Cochrane CENTRAL, Embase, and Web of Science Core Collection databases. Studies on autograft ACL reconstruction (ACLR) using HT, QT, or BPTB autograft in patients ≤18 years old with a minimum FU of 2 years were included. Graft failure rates were pooled and estimated using random-effects models via the inverse variance method and logit transformations. Meta-analyses were used to estimate failure rates and pairwise comparisons were conducted by autograft type when appropriate.
Results:
A total of 24 studies comprising 2299 patients (HT: n = 1237, 44.8% female, 59.1-month mean FU; BPTB: n = 913, 67.3% female, 79.9-month mean FU; QT: n = 149, 36.4% female, 35.3-month mean FU) were included. HT exhibited the highest failure rate at 11.8% (95% CI, 9.0%-15.4%); failure rates for BPTB and QT were 7.9% (95% CI, 6.2%-10.0%) and 2.7% (95% CI, 1.0%-7.5%), respectively. HT had a significantly higher failure rate than both BPTB (Q = 5.01; P = .025) and QT (Q = 7.70; P = .006); BPTB had a significantly higher failure rate than QT (Q = 4.01; P = .045). Male patients were less likely than their female counterparts to experience graft failure after HT ACLR (odds ratio, 0.48; 95% CI, 0.25-0.95).
Conclusion:
While the HT remains a common choice for ACLR, the current aggregate data indicate that BPTB and QT demonstrated significantly lower failure rates than HT ACLR in adolescent athletes ≤18 years old. The QT demonstrated the lowest failure rate in adolescents but also the lowest proportion of patients represented due to a paucity of published QT data, indicating a need for future studies with larger sample sizes that include QT autografts, reduced risk of bias, and consistent reporting on skeletal maturity and surgical technique to better determine the ideal autograft for active athletic populations ≤18 years old.
In the United States alone, an estimated 100,000 to 200,000 anterior cruciate ligament (ACL) injuries occur each year, corresponding to an estimated 64,000 to 100,000 ACL reconstructions (ACLRs).8,9,40 ACL injury rates are highest in young athletes due to participation in high-risk sports such as soccer, basketball, and football that involve cutting and pivoting motions with corresponding deceleration and valgus knee moments.6,9 ACL injuries in pediatric athletes continue to rise, likely attributable to increased youth sport participation and early single-sport specialization.16,19,47 ACL injuries result in significant time lost from sport, increase the risk of developing early-onset knee osteoarthritis, and alter the quality of life for young athletes.1,36 ACLR is the standard-of-care for treatment in young ACL-injured athletes to restore mechanical stability of the knee, irrespective of skeletal maturity. 16 Graft type surgical technique, management of concomitant meniscal pathology, and graft fixation strategy may contribute to postoperative outcomes.24,67
Optimal graft type for ACLR remains a source of debate and active research. 24 Despite efforts to determine optimal return-to-sport timing and requirements, graft failure continues to be a major burden, particularly among young athletes. Patients <25 years old have graft failure rates as high as 23% 66 and are 6 times more likely to reinjure their knee within 2 years of returning to sport participation compared with athletes who have no history of ACL injury. 45 These outcomes prompted exhaustive investigation into risk factors for secondary ACL injury in this population, leading to identification of young age, high activity level, sex, and allograft use as contributors.2,3,23,44,45,61,66 As surgeons have recognized the important role of the meniscus as a secondary knee stabilizer, propensity for meniscal repair alongside ACLR has increased.26,53
Notably, given the risk of growth disturbance, ACLR in skeletally immature patients provides a unique challenge, due to the open distal femoral and proximal tibial physes. No single graft type has been determined to be most appropriate for this skeletally immature population. 67 Hamstring tendon (HT) remains a common graft type for young patients outside of North America due to reduced risk of patellar fracture, anterior knee pain, and quadriceps inhibition. 30 HT autograft has become the most commonly selected autograft among surgeons worldwide, with bone–patellar tendon–bone (BPTB) the second most used but significantly less common choice for ACLR.28,58 However, HT has been questioned for use in younger athletic populations due to the potential for undersizing in small patients, tunnel widening, and evidence indicating higher failure rates for HT autografts compared with BPTB autografts in young patients.2,24,26,30,43,52,37 BPTB has been considered the gold standard for ACLR in the United States due to high rates of return to sport and lower rates of failure.15,48 Over the past decade, the quadriceps tendon (QT) autograft has received increased interest for use in ACLR in pediatric patient populations due to increased size and strength of the graft and outcomes of reduced postoperative anterior knee pain. 30 However, few studies have compared failure rates using QT with those of other autograft types in these patients. 26 Due to a paucity of published data on the QT autograft, its widespread adoption for ACLR has been limited.
While graft type is an identified risk factor for ACL graft failure, the rising rates of primary ACL injury among young patients underscore a need to understand how graft selection and subsequent failure rates vary in this age group. 16 Therefore, the purpose of this review was to compare graft failure rates between BPTB, HT, and QT autografts in patients aged ≤18 years with a minimum follow-up (FU) of 24 months. The secondary aim of this review was to stratify graft failure rates by sex, skeletal maturity, and concomitant meniscal surgery. We hypothesized that BPTB would demonstrate reduced failure relative to QT and HT autografts.
Methods
Search Strategy
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement was used as the guideline for performing this review. The protocol for the review was not registered. An information specialist/librarian (M.S.W.) searched PubMed/MEDLINE (National Library of Medicine: 1946-), Embase (Elsevier: 1966-), Cochrane CENTRAL (Cochrane Library 1996-), and Web of Science Core Collection (Clarivate: 1900-) between origin of database and March 3, 2022. A combination of controlled vocabulary and text words related to autografts was combined with the Boolean operator “AND” with controlled vocabulary and text words associated with ligaments, tendons, and bone grafts related to the patella (Appendix Table A1). Language was limited to English, and the following types of studies were excluded: case reports, comment, commentary, editorial, any type of review, or letter. Age filters were not added to the searches to avoid inadvertent exclusion of relevant records.
Data Extraction
In total, 6220 records were retrieved and imported into the citation manager EndNote 20. 62 EndNote’s “find duplicates” feature was used to remove 2110 duplicates, and 4110 records were uploaded to Covidence (Veritas Health Innovation; www.covidence.org). Covidence removed an additional 602 duplicates; thus, along with 28 records removed manually, a total of 3480 records were advanced for the initial title/abstract screening. Of 3480 records reviewed, 3188 studies were deemed irrelevant or out of scope. Team members (C.B.P., Z.B.H.) reviewed the records; for any records that were disputed, 3 additional team members (J.D.L., A.M., G.D.M.) provided conflict resolution. A total of 292 studies were determined to be eligible for full-text review, and ultimately 24 papers were included for this study (Figure 1). b

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart for inclusion and exclusion of articles.
Selection Criteria
Included studies covered autograft ACLR using HT, QT (comprising a combination of quadriceps tendon–bone [QTB] and all–soft tissue quadriceps tendon [ASTQT]), or BPTB autograft in patients ≤18 years old with a minimum FU of 2 years. Included studies also had to report ACL graft failure rates (indicated by revision ACLR, grade 2+ or worse Lachman, grade 2+ or worse pivot shift, overall International Knee Documentation Committee grade C or D, instrumented laxity with side-to-side difference of >5 mm) 14 in patients ≤18 years old. Studies on outcomes of revision ACLR, allograft, and/or allograft augmentation ACLR; ACLR with concomitant lateral extra-articular tenodesis; and studies without graft failure rates reported by both graft type and young age (≤18 years) were excluded. If >1 study reported outcomes on the same patient population, only the study with complete outcome data was included in the meta-analysis. Inclusion and exclusion criteria are also detailed in Table 1.
Inclusion/Exclusion Criteria a

ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PLC, posterolateral corner.
Assessment of Level of Evidence
Two independent reviewers (C.B.P., Z.B.H.) evaluated each study and created a classification based on the level of evidence reflecting published criteria. 31
Methodological Quality Assessment
To assess the methodological quality and risk of bias of the included studies, the Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) tool was utilized. 60 ROBINS-I tool criteria assessed by the 2 independent reviewers (C.B.P., Z.B.H.) were biases (1) due to confounding, (2) in selection of participants into the study, (3) in classification of interventions, (4) due to deviations from intended interventions, (5) due to missing data, (6) in measurement of outcomes, and (7) in selection of the reported result. Each criterion was rated as low risk, moderate risk, serious risk, critical risk, or no information in accordance with the ROBINS-I tool. 60
Statistical Analysis
Graft failure rates were pooled and estimated using random-effects models via the inverse variance method and logit transformations.4,55 For cells with zero counts, a continuity correction of 0.5 was applied. 65 The metaprop function within the metafor package in the statistical software environment (RStudio, Posit Software, PBC) was used to estimate the failure rates. 64 Subgroup analysis and pairwise comparisons were conducted by graft type. The metabin function was used to estimate the risk rates based on sex and odds ratio (OR) for the HT versus BPTB comparison. 64 Due to the small sample size, QT was not included in the OR comparison/estimation. Moderator analysis was conducted using the metareg function with between-study variance estimated using restricted maximum likelihood. Sensitivity analysis was conducted to assess if the rate estimates were similar utilizing only 2-arm studies. Statistical significance was set at P < .05. Where applicable, 95% CIs were reported.
Results
Demographic Characteristics
Across all 24 included studies, there were 1237 patients who underwent primary ACLR using HT (17 studies); 913, BPTB (8 studies); and 149, QT (109 with QTB [3 studies]20,51,63 and 40 with ASTQT [2 studies]25,46). Mean ages of patients by graft type were 14.2 years (range, 11.0-18.6 years) for HT, 15.6 years (range, 11.5-18.7 years) for BPTB, and 14.6 years (SD, 10.0-18.0 years) for QT. Mean FU duration was 59.1 months (range, 24.0-246.0 months) for patients who underwent HT ACLR, 79.9 months (range, 24.0-246.0 months) for BPTB autograft ACLR, and 35.3 months (range, 24.0-116.4 months) for QT autograft ACLR. On average, according to graft type, the proportion of patients completing FU was 88.2% for patients who underwent HT ACLR, 71.4% for patients who underwent BPTB ACLR, and 92.0% for patients who underwent QT ACLR. On average, according to graft type, 44.8% of HT, 67.3% of BPTB, and 36.4% of QT were in female patients (Table 2). Four percent of patients receiving QT had concomitant meniscal surgery, compared with 50% of patients receiving HT and 56% receiving BPTB.
Study Demographics a

NR, not reported.
All 24 included studies reported graft failure data; 11 studies included graft failure data according to sex, c 6 included mean time to graft failure,7,17,35,42,46,49 16 included skeletal maturity (open/closed physes) data, d 7 studies directly compared 2 graft types,5,12,38,41,46,51,54 and 6 included concomitant meniscal surgery data.7,11,12,18,20,49 There were no level 1 studies, 1 level 2 study, 57 7 level 3 studies,17,18,29,41,46,51,54 and 16 level 4 studies. e
Methodological Quality Assessment
For each study, risk of bias levels for each bias category using the ROBINS-I tool 60 are displayed in Table 3 and Figure 2. 34 In total, 21 (87.5%) studies had “serious” risk of bias due to confounding factors. The other bias categories were rated on average as low or moderate risk of bias.
Risk of Bias Assessments for Included Nonrandomized Studies Using the ROBINS-I a

ROBINS-I, Risk of Bias in Non-Randomized Studies of Interventions.

Risk-of-bias assessments for included studies using the Risk of Bias in Non-Randomized Studies of Interventions tool, with green representing low risk for a given criteria, yellow representing moderate risk, and red representing serious risk.
Meta-analysis
Chi-Square Test for Overall Proportion of Patients for Each Graft Type
There was a significant difference in the proportion of patients undergoing QT, HT, and BPTB ACLR (χ2 = 814.5; df = 2; P < .01), with HT consisting of the most data/patients (n = 1237), followed by BPTB (n = 913), then QT (n = 149). All differences in pairwise comparisons were significant (P < .001).
Overall Graft Failure Rates
Pooled failure rates for each graft type were 11.8% for HT autografts (95% CI, 9.0%-15.4%) (Figure 3), 7.9% for BPTB autografts (95% CI, 6.2%-10.0%), and 2.7% for QT autografts (95% CI, 1.0%-7.5%). There was a significant difference between group failure rates (χ2 = 10.5; P < .01).
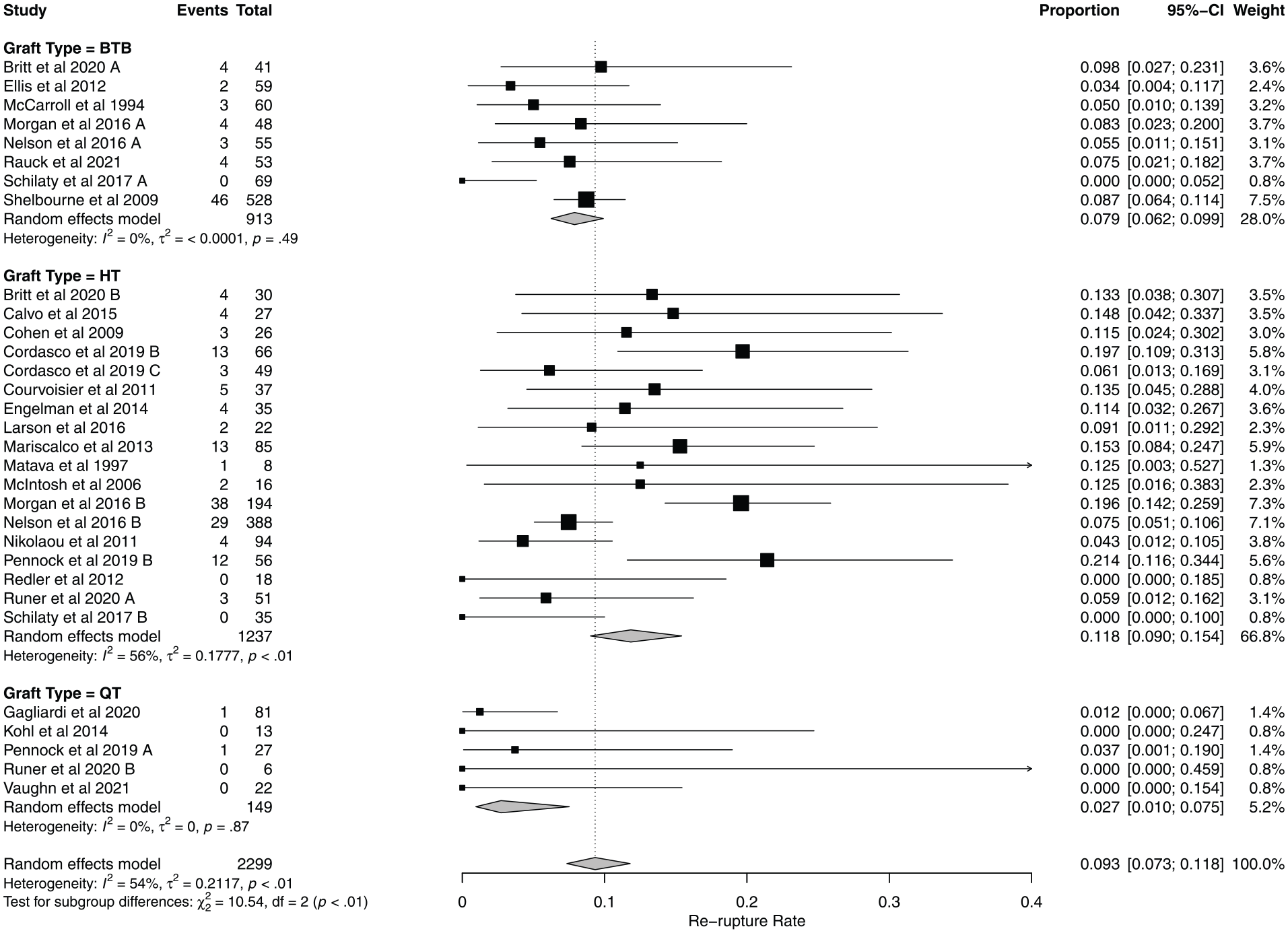
Pooled risk of graft failure by graft type for all included studies. BTB, bone–patellar tendon–bone; HT, hamstring tendon; QT, quadriceps tendon. A/B/C designations were added to author groups that included more than one autograft type in ther study in order to distinguish between graft type groups when performing statistical analysis.
Pairwise Graft Failure Comparisons
HT demonstrated significantly increased failure rates relative to BPTB ACLR (Q = 5.01; P = .025) and QT ACLR (Q = 7.70; P = .006). BPTB had significantly increased graft failure rates relative to QT ACLR (Q = 4.01; P = .045), indicating QT demonstrated the overall lowest graft failure rates in the current data set of pediatric patients.
Graft Failure by Sex
Male patients were less likely than their female counterparts to experience graft failure after ACLR with HT (OR, 0.48; 95% CI, 0.25-0.95) (Figure 4). In contrast, there were no differences in risk of graft failure by sex after BPTB ACLR. There were insufficient data to evaluate sex differences in graft failure after QT ACLR.
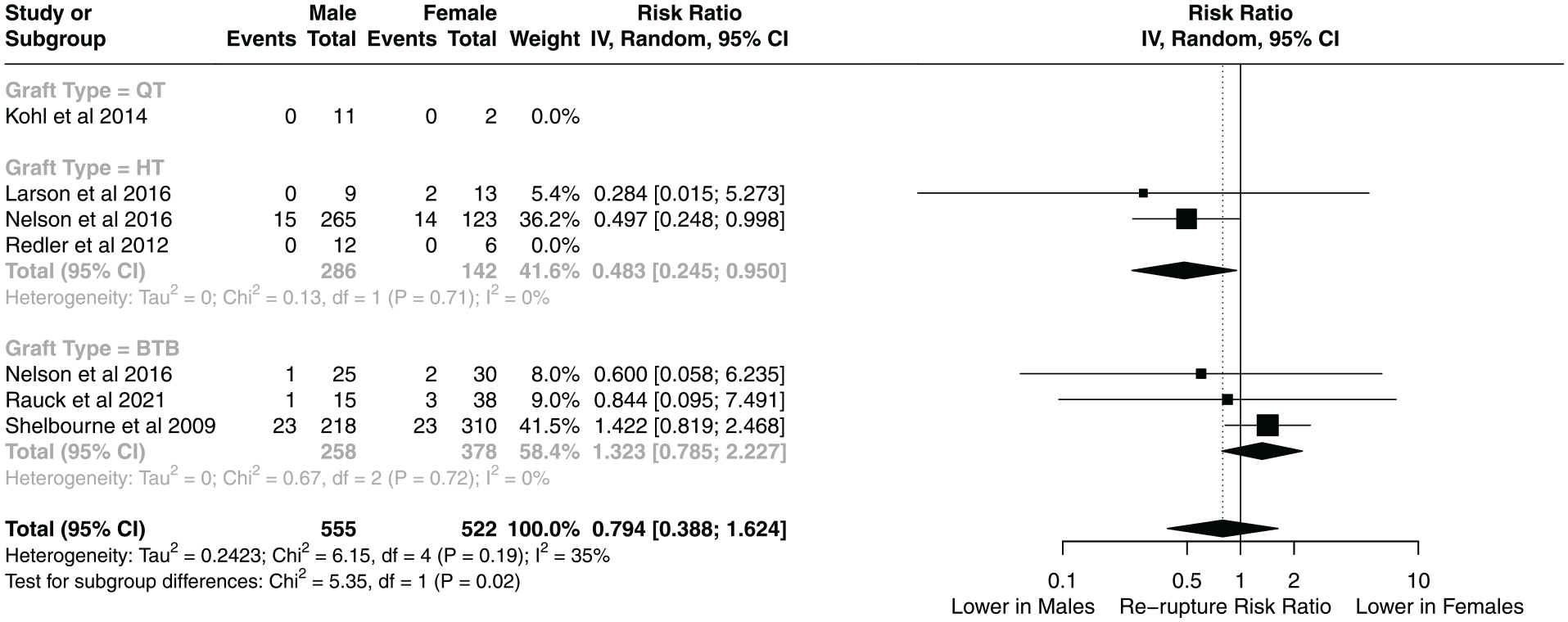
Risk of graft failure by sex for each graft type. BTB, bone patellar tendon bone; HT, hamstring tendon; QT, quadriceps tendon.
Sensitivity Analyses
Other Potential Moderators
There were no differences between graft types with regard to mean FU (Q = 0.620; P = .431), mean time to graft failure (Q = 0.242; P = .623), mean age (Q = 0.571; P = .450), and sex by proportion of female patients (Q = 0.017; P = .897). There was a statistical influence between concomitant meniscal surgery and graft type (Q = 7.843; P = .005). The proportion of patients receiving concomitant meniscal surgery with QT reported less meniscal pathology than BPTB and HT ACLR.
Discussion
This study yielded several important findings, most notably that HT autograft provides a significantly higher graft failure rate than BPTB autograft in pediatric patients. However, the data did not support our hypothesis that BPTB would demonstrate reduced failure relative to QT autografts after ACLR in patients ≤18 years old. Specifically, despite limited available data, QT autografts were associated with significantly lower graft failure rates than BPTB autografts. In addition, male patients were significantly less likely than female patients to experience graft failure after ACLR, specifically with HT grafts. Interestingly, there was an unequal proportion of patients ≤18 years old that underwent HT, BPTB, and QT ACLR. The highest proportion of patients underwent HT ACLR, followed by BPTB ACLR, and last, QT ACLR. However, an increased sample size of patients with QT ACLR in addition to more consistent reporting on skeletal maturity and surgical technique are needed to better determine the ideal graft for adolescent athletes.
The meta-analysis indicated that QT autografts comprised the lowest proportion of patients ≤18 years old who underwent ACLR. Despite growing interest in the QT autograft due to its increased size and biomechanical strength, a paucity of QT ACLR patient-reported outcome measures in the literature has prevented its widespread adoption. Although the QT data were limited, the meta-analysis found that QT autografts had significantly lower failure rates than both BPTB and HT autografts. This finding aligns with previous work, in which a meta-analysis of 21 studies reported a 2.1% graft failure rate for QT in patients of all ages. 39 In addition to lower failure rates, QT autografts offer clinical and biomechanical benefits over BPTB autografts, such as increased cross-sectional area, increased ultimate load to failure, and increased stiffness. 56 Moreover, histological analysis revealed that QT autografts have more collagen fibrils and fibroblasts per cross-sectional area than BPTB autografts. 22 QT autografts also confer a lower risk of donor-site morbidity and easier graft harvesting procedures, which can result in less tissue damage and pain.10,59 However, previous research demonstrated equivalent patient-reported outcomes after ACLR with a QT autograft compared with BPTB and HT autografts. 10 Further, although the results of this meta-analysis support a benefit of QT autograft, it is important to note the smaller sample size representing QT in the included studies compared with those representing BPTB and HT autografts. Larger studies of QT ACLR in high-risk patient populations are needed to resolve these findings.
ACLR in a pediatric population involves unique considerations including factors such as graft type, graft fixation, and skeletal maturity.21,67 The current meta-analysis did not detect differences in graft type failure rates with respect to skeletal maturity. Specifically, there were no significant differences in failure rates between graft types for mean time to graft failure or patient age. However, conclusions should be tempered considering inconsistencies in how data were reported in the included studies. Limited available data on skeletal maturity prevented a comprehensive analysis of how this factor affects graft failure rates (chronologic age was similar between groups). While there was no statistical difference, soft tissue autografts (QT and HT) were used more commonly in younger patients. Future studies should report both skeletal maturity and graft failure rates to overcome the small sample size limitation encountered in this analysis of the effect of skeletal maturity on graft failure rates in pediatric patients.
Applying the ROBINS-I tool in the present meta-analysis revealed that 91.7% of the studies had an overall serious risk of bias. The domain most consistently rated as a serious risk was bias due to confounding factors. This assessment suggests that future studies should carefully consider and attempt to mitigate potential confounding factors, such as sex, age, sport, and level of activity, to reduce bias and improve reproducibility.
Limitations
The results of this meta-analysis should be interpreted in the context of its limitations. Overall, this study’s primary outcome of interest was graft failure, although it is known whether there are other factors, such as return to sport, contralateral ACL injury, anterior knee pain, and donor-site morbidity, that should be considered when determining the ideal autograft for pediatric patients. The unequal proportion of patients undergoing HT, BPTB, and QT ACLR could have influenced failure rate calculations, with a greater proportion of HT autografts included leading to increased capture of graft failures and vice versa for QT autografts. Moreover, only 7 studies directly compared 2 different graft types, which makes definitive conclusions more difficult. Additionally, inconsistent reporting of skeletal maturity hindered the ability to accurately pool and assess the effect of skeletal maturity on graft failure. Future studies should more carefully assess and report skeletal maturity. With these data focused on a pediatric population, who are at most risk of graft failure, we acknowledge that there is likely some variance in physeal status of subsets of the data reported and that physeal sparing techniques may have been employed. These data were not commonly reported and thus not included in moderator analyses, and results should not be generalized to specific physeal status or physeal sparing techniques. However, given similar chronologic ages between groups, it is unlikely that significant differences exist with regard to physiologic ages for the entire population. Additionally, while this analysis investigated the effect of graft type and other associated risk factors on graft failure, return-to-sport and functional knee outcomes after ACLR before graft failure were not considered. Rehabilitation programs and return-to-sport guidelines that differ between studies could influence graft failure rates. Heterogeneity in the definitions of graft failure used by each study also complicated the graft failure comparisons. For our analysis, QTB and ASTQT were consolidated into a single QT autograft type, and the effects of bone plug on clinical and functional outcomes remain poorly understood.
Another important limitation of the current investigational results was the variance in FU reporting windows after ACLR. Longer FU time will likely result in a larger number of graft failures. While FU time was not statistically different, the BPTB group had generally longer FU times that may have influenced relative graft failure rates for the included studies.
Another consideration for graft failure rates is the presence or absence of concomitant procedures with ACLR. The percentage of patients that underwent concomitant meniscectomy and/or meniscal repair with ACLR demonstrated significant differences depending on graft type, most likely due to neglected meniscal pathology or lack of reported data. Only 4% of patients receiving QT had concomitant meniscal surgery, compared with 50% of patients receiving HT and 56% receiving BPTB. Further, concomitant meniscal surgery was related to significant differences in graft failure rate, but there were too few studies to better delineate this association. The low percentage of concomitant surgeries in the QT group likely reflects incomplete reporting, which suggests caution in interpreting the significant difference in failure rates. Further, the true prevalence of meniscal pathology is unknown since the extracted data included only the surgically treated meniscal pathology. Altogether, these data indicate that graft type and concomitant meniscal surgery may affect the risk of graft failure in pediatric patients undergoing ACLR. More research, and complete reporting on pathological/surgical data, is needed to evaluate the interaction between graft type and concomitant meniscal surgery on graft failure.
Finally, in the absence of high-quality evidence, excluding studies by level of evidence was not always appropriate or possible and should be considered. As such, this study is limited by quality of the available data and the scientific rigor underlying data collection. We therefore used the ROBINS-I tool to assess bias in these instances to evaluate these studies explicitly. The overall so-called “serious risk of bias” across 22 of 24 (92%) studies should not be dismissed. Finally, reporting heterogeneity limits the strength of conclusions that could be made.
Conclusion
While the HT remains a common choice for ACLR, the current aggregate data indicate that BPTB and QT demonstrated significantly lower failure rates than HT ACLR in adolescents ≤18 years old. The QT ACLR demonstrated the lowest failure rate in adolescents but also the lowest proportion of patients represented, indicating a need for future studies with larger sample sizes that include QT autografts, reduced risk of bias, and consistent reporting on skeletal maturity and surgical technique to better determine the ideal graft for highly active athletic populations ≤18 years of age.
Footnotes
Appendix
PubMed Search Query a

| PubMed (NLM): |
| Dates searched: January 1, 1946-March 3, 2022 |
| Filters: English |
| Filters: Use of Boolean “NOT” to exclude case reports, comments, reviews, letters, and editorials |
| 1. ("hamstring tendons/transplantation"[MeSH] OR ("hamstring tendons"[MeSH] AND ("transplantation"[MeSH:noexp] OR transplant*[TW])) OR "hamstring tendons transplant*"[TW] OR "Semitendinosus Tendon"[TW] OR "semitendinosus gracilis"[TW]) AND ("autografts"[MeSH Terms:noexp] OR "Transplantation, Autologous"[MeSH] OR "Autologous Transplant*"[TW] OR "autograft*"[TW] OR "autologous repair"[TW] OR autotransplant*[TW]) |
| 2. ("Patellar Ligament/transplantation"[MeSH] OR ("patellar ligament"[TW] AND ("transplantation"[MeSH:noexp] OR transplant*[TW] OR graft*[TW])) OR ("patella"[MeSH] AND "ligaments"[MeSH] AND ("transplantation"[MeSH:noexp] OR transplant*[TW]))) AND ("autografts"[MeSH:noexp] OR "Transplantation, Autologous"[MeSH] OR "Autologous Transplant*"[TW] OR autograft*[TW] OR "autologous repair"[TW] OR autotransplant*[TW]) |
| 3. ("Bone-Patellar Tendon-Bone Grafts"[MeSH] OR (("BPTB"[TW] OR "Bone patellar tendon bone"[TW] OR "bone patellar bone"[TW] OR "bone tendon bone"[TW] OR "Tendon Bone Graft*"[TW] OR ("patella"[MeSH] AND "tendons"[MeSH:noexp]) OR "patellar tendon"[TW]) AND ("transplantation"[MeSH:noexp] OR transplant*[TW] OR graft*[TW]))) AND ("autografts"[MeSH:noexp] OR "Transplantation, Autologous"[MeSH] OR "Autologous Transplant*"[TW] OR autograft*[TW] OR "autologous repair"[TW] OR autotransplant*[TW]) |
| 4. ((("Quadriceps Muscle"[MeSH Terms] AND "Tendons"[MeSH Terms:noexp]) OR "bone quadriceps tendon"[TW]) AND ("autografts"[MeSH Terms:noexp] OR "Transplantation, Autologous"[MeSH] OR "Autologous Transplant*"[TW] OR "autograft*"[Text Word] OR "autologous repair"[TW] OR autotransplant*[TW])) OR "soft tissue quadriceps tendon autograft"[TW] OR "Quadriceps tendon autograft"[TW] OR "quad tendon autograft"[TW] OR "quad autograft"[TW] OR "quadriceps autograft"[TW] OR "Quadriceps tendon autograft"[TW] OR "quadriceps autograft"[TW] |
| 5. "Anterior Cruciate Ligament Injuries/surgery"[MeSH] OR "Anterior Cruciate Ligament/surgery"[MeSH] OR "Anterior Cruciate Ligament Reconstruction"[MeSH] OR "anterior cruciate ligament*"[TW] OR ACLR[TW] OR ACL[TW] OR "Knee Joint/surgery"[MeSH] OR "knee injuries/surgery"[MeSH] OR ("knee joint"[TW] OR "knee injur*"[TW] AND (surg*[TW] OR repair[TW] OR reconstruct*[TW])) |
| 6. (#1 OR #2 OR #3 OR #4) AND #5 |
| 7. (#6 AND English[LA]) NOT ("review"[PT] OR "systematic review"[PT] OR "systematic review"[TI] OR "meta-analysis"[PT] OR "meta analysis"[TI] OR "case reports"[PT] OR case report*[TI] OR "literature review"[TI] OR "narrative review"[TI] OR "scoping review"[TI] OR letter[PT] OR letter[TI] OR editorial[PT] OR editorial[TI] OR comment[PT] OR comment*[TI] OR booksdocs[Filter] OR preprint[PT]) |
[MeSH]-Medical Subject Heading (Controlled vocabulary) in PubMed; [MeSH:noexp]- indicates do not explode the MeSH: do not search the more specific terms under the broad category; [TIAB]-search title and abstract; [PT]-publication type; [TI]-search title of article; [TW]-Text Word: all words and numbers in the title, abstract, other abstract, MeSH terms, MeSH Subheadings, Publication Types, Substance Names, Personal Name as Subject, Corporate Author, Secondary Source, Comment/Correction Notes, and Other Terms.
Final revision submitted April 7, 2024; accepted April 18, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.H.S. has received education payments from Evolution Surgical and Peerless Surgical and hospitality payments from Arthrex. J.D.L. has received hospitality payments from Arthrex and Smith & Nephew, education payments from United Orthopedics and Smith & Nephew; and consulting fees from DePuy Synthes Products. J.W.X. has received royalties from Arthrex, consulting fees from Arthrex and Trice Medical, nonconsulting fees from Arthrex, and education payments from United Orthopedics. G.D.M has current and ongoing research funding to his institution from Arthrex Inc. to evaluate ACL surgical treatment strategies. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.