
Abstract
Background:
The updated Oslo Sports Trauma Research Questionnaire on Health Problems (OSTRC-H2) has been translated into a limited set of languages and lacks full validation of its new measures.
Purpose:
To (1) translate, cross-culturally adapt, and evaluate the measurement properties of the OSTRC-H2 for the Slovenian population and (2) investigate the construct validity for the severity score and time lost due to a health problem.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
The OSTRC-H2 was translated from English to Slovenian (OSTRC-H2-SLO) according to international guidelines. A 15-week study was conducted among 188 elite athletes, with a test-retest performed in the 10th week. Internal consistency, reliability, content validity, feasibility, and potential ceiling effects were investigated. Internal consistency was measured using the Cronbach alpha coefficient, while reliability was measured with the intraclass correlation coefficient (ICC). Construct validity was measured with the Spearman rank correlation coefficient (rS).
Results:
There was a 95% response rate and an 18% mean weekly prevalence of health problems. The OSTRC-H2-SLO showed excellent test-retest reliability (ICC, 0.94 [95% CI, 0.67-0.99]), with a Cronbach α of .93. A strong positive correlation was found between the OSTRC-H2-SLO severity score and days lost due to an acute injury (rS = 0.754), overuse injury (rS = 0.785), and illness (rS = 0.894) (P < .001 for all). Moderate to strong negative correlations were observed between severity score and total load (training and competition load in hours) as well as between days lost and total load (P < .001 for all).
Conclusion:
The OSTRC-H2-SLO was found to be valid, reliable, and well accepted among Slovenian athletes. The authors confirmed the questionnaire's construct validity and identified total load as an indicator of an increase in the severity score.
Registration:
NCT05471297 (ClinicalTrials.gov identifier).
The process of injury and illness surveillance entails the systematic and continuous collection and analysis of data pertaining to injuries and illnesses. Such monitoring can be used to capture health data during shorter time periods such as major sports events (eg, the Olympic Games)6,18,25,37,38 and it can facilitate the evaluation of injury and illness risk and athletes’ health throughout an entire season.10,12 In doing so, it can be used to determine risks related to sport participation, measure injury trends between 2 or more seasons, and identify the effectiveness of preventive interventions.
Many sports organizations worldwide have adopted injury surveillance programs with their own monitoring tools. These include the National Football League, 17 the National Collegiate Athletic Association, 27 the Fédération Internationale de Football Association, 24 the Union of European Football Associations Champions League Injury Study, 20 the International Ski Federation, 19 and others. 15 However, these monitoring tools lacked a clear methodology, particularly in terms of consistency and frequency of data collection as well as differences in injury definitions and research reporting practices. There was also the challenge of implementing these methods among individual athletes or those without a centralized team structure. 10 Consequently, they often failed to capture certain health problems such as overuse injuries.
In 2013 and 2014, researchers from the Oslo Sport Trauma Research Center (OSTRC) proposed 2 new approaches to injury surveillance: the OSTRC Overuse Injury Questionnaire 9 (OSTRC-O) and the broader OSTRC Questionnaire on Health Problems 10 (OSTRC-H, updated in 2020 to OSTRC-H28). The OSTRC-H2 questionnaire includes 4 key questions, which are used to calculate a severity score. 8 It also includes questions to capture the injury mechanism and activity and identify whether the health problem is an exacerbation, recurrence, or a subsequent issue. Additionally, the OSTRC-H and OSTRC-H2 moved from the traditional “time-loss” definition, which considers only the health problems causing an athlete's absence from training or competition, to a broader health problem definition. This includes any health problem that impairs an athlete's ability to train or compete as usual, regardless of time lost from training or competition, which leads to the questionnaire's capturing more overuse injuries. Thus, the OSTRC-H2 captures both time lost and ongoing health problems, with the severity score indicating changes in performance/intensity/pain domains. Although these measures might be valuable, they are not yet fully validated. 8
Due to its practical value for sport and medical professionals, the OSTRC-O has been translated and validated for Norwegian athletes 9 ; German Paralympians 21 ; Spanish youth 3 and adult athletes 29 ; and Danish, 23 Swedish, 16 Brazilian, 33 Japanese, 30 and Thai-speaking athletes 26 to date. However, the OSTRC-H2 has been translated and validated only in Japanese, 31 Spanish, 3 and French. 5 Moreover, construct validity for the severity score and time-loss data has not yet been investigated.
There is currently no available tool for health problem surveillance of athletes speaking the Slovenian language. Therefore, the objectives of this study were to (1) translate and culturally adapt the OSTRC-H2 into the Slovenian context (OSTRC-H2-SLO), (2) evaluate the measurement properties (construct validity, reliability, responsiveness, and floor and ceiling effects) of the OSTRC-H2-SLO, and (3) investigate the construct validity for severity score and time lost for each type of health problem (ie, acute injury, overuse injury, and illness). We hypothesized that there would be a moderate to strong correlation between the OSTRC-H2-SLO severity score and days lost due to a health problem. Furthermore, we hypothesized that the total load of an athlete (training and competition) would correlate negatively with both severity score and time lost due to a health problem.
Methods
Study Design and Participants
This study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines 11 and a CHecklist for statistical Assessment of Medical Papers. 28 The protocol for the study received ethics committee approval, and the project was registered on Clinical Trials.gov. The study consisted of 2 phases: First, the questionnaire was translated and culturally adapted from English to Slovenian and pretested on a sample of 15 elite athletes; second, a longitudinal study of 15 weeks was conducted, with a test-retest evaluation on week 10. During the test-retest assessment, athletes were asked to complete the questionnaire 2 times within 48 hours, with the purpose to evaluate the reliability of the questionnaire.
The initial cohort was defined as the Slovenian First League men's handball players. An estimated sample size of 149 participants was calculated prospectively for the purposes of the study. 14 We approached the Slovenian Handball Federation and its team coaches with a proposal for participation in the study. If teams expressed an interest, athletes and team staff were informed about the study purpose and asked to sign the consent to participate. Ten handball clubs, including 188 athletes competing at the elite level, accepted the invitation. The inclusion criteria were age >18 years of age and the ability to understand and speak the Slovenian language.
OSTRC-H2 Questionnaire
The OSTRC-H2 is a survey to capture health problems in athletes. The questionnaire consists of 4 main questions regarding an athlete's (1) participation in training/competition, (2) modifications in training/competition, (3) sports performance, and (4) symptoms, based on which the severity of a health problem is determined (severity score; range, 0-100 [worst]). If an athlete reports a problem, he/she is asked to provide further information such as type of health problem, location, mechanism, and symptoms. Additionally, the athlete reports days lost due to a health problem (number of days missed from training/competition), which serves as a time-loss measure. The updated OSTRC-H2 from 2020 also proposes a new logic; if an athlete reports “Full participation without health problems” on the first question, the questionnaire is completed, as all further questions are redundant, and a severity score of 0 is assigned. If an athlete reports “Could not participate due to a health problem,” a severity score of 100 is assigned, and the athlete continues to the additional questions about the health problem, without answering questions 2 to 4.
Translation, Cross-Cultural Adaptation, Responsiveness, Reliability, and Construct Validity
The 2020, English version of the OSTRC-H28 was used for the Slovenian translation. The translation of the questionnaire was conducted in accordance with guidelines by Beaton et al 4 and were as follows:
Stage 1: Initial Translation. Three bilingual Slovenian residents (T1, T2, and T3), who were native Slovenian speakers, independently translated the English questionnaire into Slovenian. T1 and T2 were familiar with the concepts being examined, while T3 was not. The project manager (K.D.), who was one of the translators, was involved in all stages of the adaptation process.
Stage 2: Synthesis. The results were synthesized from the 3 translations. A consensus and a written report were made about the issues addressed and resolved, which resulted in a new version of the questionnaire (T123).
Stage 3: Back Translation. The new version of the questionnaire was then back-translated into English by 2 translators who were unfamiliar with the original version of the questionnaire and unaware of the concepts being explored.
Stage 4: Expert Committee. An expert committee composed of the forward- and back-translators and a methodologist then compared the Slovenian and English translated versions with the original versions to ensure equivalence. A consensus was made about the final version of the questionnaire.
Stage 5: Pretest. A total of 15 elite athletes from the Slovenian First League men's handball league, were asked to assess the comprehensibility and clarity of the questionnaire.
Stage 6: Approval of the Final Version. A final version of the questionnaire underwent proofreading and checking for grammar errors and was approved by the expert committee.
Data Collection
The 188 study participants were asked to complete the OSTRC-H2-SLO questionnaire, administered through an online platform 1ka (www.1ka.si), every week for 15 weeks during the 2022-2023 handball season. The reminder with a link to the online questionnaire was sent to them via email every Sunday, and if not answered, athletes were reminded again within 2 days. The athletes who reported a health problem were contacted by a medical professional to clinically verify the reported issue.
The test-retest was conducted in the 10th week of the study, during which participants completed the OSTRC-H2-SLO twice within a 48-hour period. They received a regular reminder with a link to the questionnaire on Sunday, instructing them to complete the questionnaire twice within 48 hours. The athletes were instructed to answer questions during the same 7-day period (Monday to Sunday, with exact dates) both times. An additional reminder to complete the questionnaires was sent on Monday. Athletes who reported a health problem and those who did not were included in the analysis.
Other Measures
In addition to the OSTRC-H2-SLO responses, we collected the athletes’ age, height, weight, and training experience, defined by the number of years they had been playing team handball. Furthermore, we recorded the weekly training load, which was segmented into sport-specific (handball) training and strength and conditioning training, along with competition load (measured in minutes of games played). The competition load was then converted into hours and combined with the training load, resulting in the variable “total load.”
Data Analysis
All statistical analyses were conducted with SPSS statistical software (Version 29.0; IBM). Descriptive statistics, including means with standard deviations, were used to summarize demographic characteristics of the participants and questionnaire outcomes. The reliability of the study was assessed using internal consistency and test-retest reliability methods. Internal consistency measures the extent to which items within a scale are interrelated and was calculated using the Cronbach alpha (α), where values of .70, .80, and >.90 were considered acceptable, good, and superior, respectively. Based on the previous studies, we hypothesized a Cronbach α estimate of >.80.
Relative reliability (ie, test-retest reliability) was measured using the intraclass correlation coefficient (ICC), in which ICC values were classified as low (<0.40), moderate (0.40-0.75), substantial (0.76-0.90), or excellent (>0.90). In addition, absolute reliability was measured by calculating the standard error of measurement, followed by the coefficient of variation (CV). 22 To assess the relationship between severity score, days lost due to health problems, and total load, a bivariate correlation analysis was conducted. Due to nonparametric data distribution, the Spearman rank-order correlation coefficient (rS) was used. The following thresholds were used to assess magnitude of the relationships analyzed: weak, rS≤0.35; moderate, 0.36 ≤rS < 0.67; and strong, 0.68 ≤rS < 1.0. 39 Finally, we assessed the ceiling effect, which was defined as present if >15% of the athletes obtained the maximum score. Floor effects were not assessed, as a score of 0 on the OSTRC-H2 only indicated the absence of health issues during the follow-up period. Statistical significance for all analyses was accepted at P≤ .05.
Results
Translation and Adaptation of the OSTRC-H2
The forward translation process of the questionnaire encountered only minor issues, such as variations in terms for describing injury location; for instance, podlahtnica for podlaket (both meaning “lower arm”) and nadlahtnica for nadlaket (both meaning “upper arm”). Other minor discrepancies encompassed variations in noun usage for describing symptoms or injury location, choices between singular and plural, and differences in sentence structure.
Feasibility: Measurement Properties
The mean age of the 188 participants was 23.3 ± 4.3 years, and their mean weekly training load was 9.0 ± 4.7 hours. A total of 146 athletes (mean age, 23.5 ± 4.4 years) participated in the test-retest analysis on week 10 and answered the questionnaire 2 times within 48 hours. Participant characteristics are presented in Table 1.
Participant Characteristics a

Data are presented as mean ± SD, with ranges in parentheses.
Throughout the 15-week period, a total of 2815 questionnaires were distributed and 2665 were returned, yielding a high overall response rate of 95%. Among the responses, 514 health problems were reported, comprising 330 acute injuries, 145 overuse injuries, and 39 reports of illnesses. Approximately 34 athletes per week (18%) reported a health problem. Among all reported cases, 39% represented first-time health issues, while the remaining 61% were recurrent cases. Overall, there were 1716 lost training days (3.4 ± 2.5 days/athlete), with 1237 days lost for acute injuries, 303 days for overuse injuries, and 176 days for illnesses. The time that participants needed to complete the questionnaire ranged from 13 to 104 seconds.
The highest severity scores were observed for illnesses, which were reported in 12 of the 15 weeks (mean score per week, 78.0 ± 27.4) and had 3 peaks within the 15 weeks (weeks 5, 11, and 14). A relatively stable severity score curve with no peaks was seen for acute injuries (mean score per week, 69.0 ± 31.3), which were reported every week. The lowest weekly severity scores were reported for overuse injuries (mean score per week, 47.0 ± 28.2) with a single peak in week 13 (Figure 1).
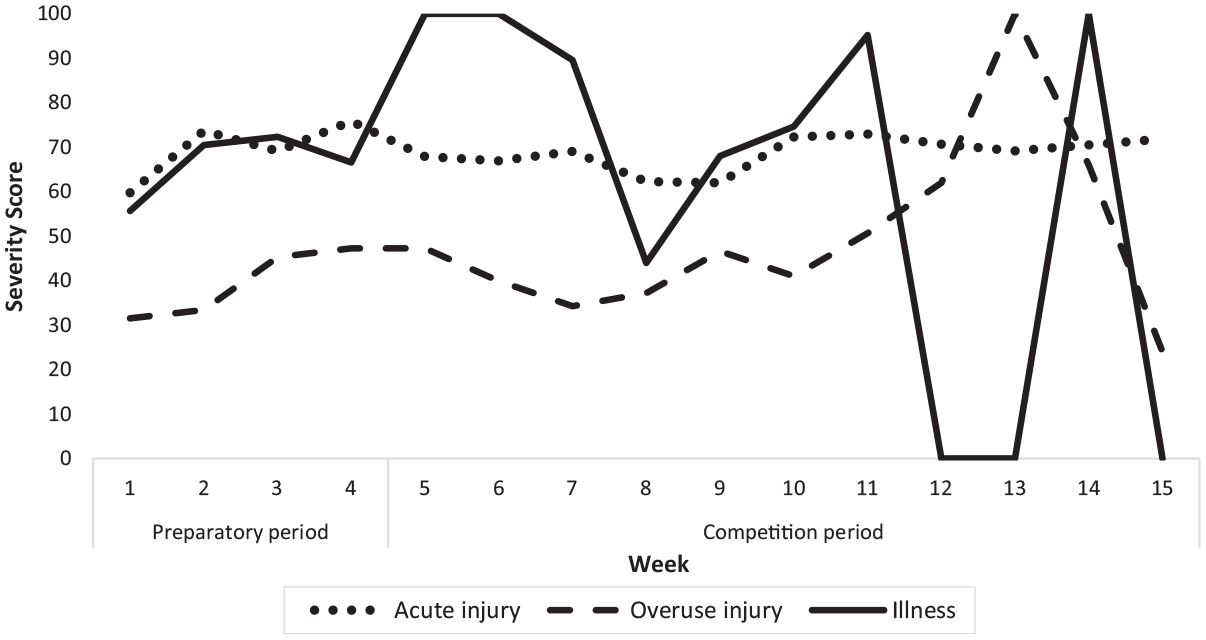
Oslo Sports Trauma Research Questionnaire on Health Problems, Slovenian translation, severity scores for acute injury, overuse injury, and illness over the 15-week study period. During the preparatory period, athletes train and compete in nonofficial games. Athletes continue training while official games begin during the competition period.
Internal Consistency and Test-Retest reliability
Cronbach α values ranged from good (question 4 [symptoms], α = .82) to excellent (question 1 [participation], α = 1.00) (severity score, α = 1.00) (Table 2). The test-retest reliability showed substantial to excellent mean ICC values, ranging from 0.84 (95% CI, 0.24-0.97) for question 4 to 1.00 (95% CI, 1.00-1.00) for question 1 (Table 2). The measure of absolute variability, calculated as CV, ranged from 0% (question 1) to 0.53% (question 4) (Table 2).
Reliability Analysis of OSTRC-H2-SLO Between Time 1 and Time 2 (n = 146) a

Data are presented as mean ± SD unless otherwise indicated. ANOVA, analysis of variance; CV, coefficient of variation; ICC, intraclass correlation coefficient; MDC, minimal detectable change; SEM, standard error of measurement.
Construct Validity (Severity Score, Days Lost, and Total Load)
We found strong positive correlations between severity score and days lost due to an acute injury (rS = 0.754), overuse injury (rS = 0.785), and illness (rS = 0.894) (P < .001 for all). Furthermore, we observed moderate negative correlations between severity score and total load for acute injuries (rS = −0.468) and overuse injuries (rS = −0.410) (P < .001 for both). Correlations between days lost and total load were found to be moderately negative for both acute injury (rS = −0.543) and overuse injury (rS = −0.451) (P < .001 for both). Regarding illness, a moderate negative correlation was observed between the severity score and total load (rS = −0.589; P < .001), and a strong negative correlation was observed between days lost and total load (rS = −0.820; P < .001). Figure 2 shows a coordinated movement of the days lost and severity score curves within the 15 weeks for acute injuries and illnesses.

Correlation of Oslo Sports Trauma Research Questionnaire on Health Problems, Slovenian translation, severity score, days lost due to a health problem, and total load for (A) acute injuries and (B) illnesses.
Ceiling Effects
Only 14 of the 146 athletes (9.6%) obtained the maximum severity score; therefore, no ceiling effects were found.
Discussion
The findings from our study confirmed that the OSTRC-H2-SLO is a valid and reliable health problem surveillance tool and acceptable for use by Slovenian athletes. We observed a high response rate (95%) within a large sample (N = 188 and n = 146 for the longitudinal and test-retest study, respectively), which was comparable with those of other OSTRC-H2 validation studies made on Japanese (N = 101; 97%), French (N = 80; 95%), and Spanish (N = 63; 99%) athletes. The mean number of participants included in other OSTRC-H2 validations was N = 81 with a mean follow-up of 11 weeks. The questionnaire was shown to be feasible, as athletes needed very little time to answer the questions (13-104 seconds). The test-retest results showed excellent questionnaire reliability (ICC, 0.94 [95% CI, 0.67-0.99]) and very good internal consistency (Cronbach α = .93). Our results are comparable with studies for the French (ICC, 0.90 [95% CI, 0.68-0.98]; Cronbach α = .94) 5 and Spanish (ICC, 0.87 [95% CI, 0.79-0.92]; Cronbach α = .93) 3 versions. There were no major issues with the translation, apart from minor wording issues and sentence structuring that were resolved with the assistance of a third translator and an expert committee. These findings highlight the effectiveness of the OSTRC-H2-SLO in capturing health problems and underscore its utility as a standardized surveillance tool in Slovenian sports settings.
Studies have shown that many athletes continue to train and compete despite being injured, which is particularly significant for overuse injuries.1,9,32 This insight served as an argument to further develop methodology beyond capturing time-loss injuries/illnesses and instead create a proxy for assessing severity, leading to the development of a severity score. Our study confirms this trend as well (Figure 1), as athletes with overuse injuries reported fewer days lost due to a health problem than athletes with acute injuries. Acute injuries resulted in the longest time away from training and competition, followed by illnesses and overuse injuries. This highlights the need for a more complex approach to injury surveillance that goes beyond simply recording time loss and considers the severity and impact of health problems on athletes’ ability to train and compete effectively.
The measurement properties for time loss (ie, health problem severity) were unknown, as there were no other validated instruments for measuring similar constructs to date. Our results revealed that severity score, days lost, and total load are highly correlated, which further confirms the validity of the questionnaire. The construct of health problem severity was evaluated using 3 measures: severity score, days lost, and total load (represented as the sum of training and competition load). The results revealed a strong positive correlation between severity score and days lost, indicating that both variables represent the same construct: severity of the health problem. Specifically, a higher severity score corresponded to more days that athletes were absent from training and competition. Furthermore, the total load provided additional support for the construct validity. Moderate to strong negative correlations were found between severity score/days lost and total load. It was observed that when the severity score was highest (100), the total load was 0 (Figure 2B), thereby reinforcing the relationship between severity of health problems and athletes’ absence from training and competition. Additionally, since a pattern of acute injuries occurring approximately 2 weeks after a peak of total load was observed (Figure 2A), we may assume that total load is a precursor of an injury. Further studies with a longer follow-up are warranted to investigate this concept more thoroughly.
The development and validation of the severity score represents a significant step forward in this regard, providing a comprehensive measure of the severity of health problems experienced by athletes. By incorporating factors such as symptom severity and their impact on performance, the severity score offers a more holistic assessment of athletes’ health status. This allows sports medicine practitioners to better understand the nature and extent of injuries, enabling more targeted interventions and rehabilitation strategies tailored to individual athletes’ needs. 2 Our findings emphasize the importance of proactive injury prevention strategies aimed at mitigating the risk of overuse injuries and minimizing their impact on athletes’ performance. This requires a multidimensional approach that includes proper periodization, load monitoring, and training load optimization, implementing appropriate recovery protocols, particularly during intensified training periods, and fostering a culture of open communication between athletes and medical staff.35,36 The findings of our study underscore the need for ongoing monitoring and surveillance to detect early signs of injury and intervene promptly to prevent further deterioration. Injuries are recognized as one of the main mechanisms leading to premature termination of an athlete's sports career and can continue to cause pain and issues even after retirement.7,13,34 Therefore, it is crucial to invest efforts toward comprehensive athlete health care, which includes injury and illness surveillance, prevention, and rehabilitation. Continued research in this area is essential to further refine injury surveillance methods and enhance athlete well-being in elite sports.
Strengths and Limitations
Although this study has many strengths, such as high response rate, frequent questionnaire administration, and large and homogeneous sample size, our approach has some limitations. The homogeneous sample could be seen as a limitation, as the applicability to children, women, and other sports needs to be considered. Although we presume the applicability to other sports and female athletes would not affect the validity of the questionnaire much, collecting answers from children and adolescents may pose greater challenges due to limited comprehension and other potential barriers. There is a limitation stemming from the absence of other well-established instruments for assessing the construct of interest in the Slovenian language, which could not be addressed. Moreover, as in other questionnaires, the athlete's responses on the OSTRC-H2-SLO are subjective and might therefore under- or overestimate the presence of pain and potential health issues. The results also depend on the assumption that the athletes are providing honest information. However, we addressed this concern by providing an anonymized identification for each athlete, which only the athlete, the researcher, and the team's medical staff had access to.
Conclusion
Our study demonstrated that the OSTRC-H2-SLO was valid, reliable, and well accepted among Slovenian athletes. We confirmed the questionnaire's construct validity and identified total load as an indicat or of an increase in the severity score.
Footnotes
Acknowledgements
The authors thank the athletes and their support staff (physical therapists and coaches) for their participation in this study.
Final revision submitted May 6, 2024; accepted May 21, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research took place within the Kinesiology of Monostructural, Polystructural and Conventional Sports research program (code No. P5-0147), which was financed by the Slovenian Research and Innovation Agency (research fellowship grant No. 393/2020). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Republic of Slovenia, Ministry of Health (ref No. 0120-109/2022/3).