
Abstract
Background:
Medial hamstring tendons harvesting can be performed through either an anterior or a posterior approach. It has been suggested that using a posterior approach may result in a longer length of harvestable tendon compared with an anterior approach.
Hypothesis:
There would be no difference in the length of the harvestable tendon between the anterior and posterior approaches.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A retrospective study was conducted at the primary institution using prospectively collected data from skeletally mature Chinese patients who underwent medial hamstring tendons harvesting between January 2008 and December 2021. Patients were excluded if they had experienced graft harvesting complication or if only 1 medial hamstring tendon was harvested. One-to-one exact matching was performed between the 2 approaches based on body height and sex. The outcome assessed was the length of the harvested tendon.
Results:
A total of 536 patients underwent medial hamstring tendons harvesting using an anterior approach, while 58 underwent it using a posterior approach, all of whom met the inclusion criteria. A group of 54 matched pairs were identified. The length of the harvested semitendinosus tendon was 263 ± 29 mm in the anterior approach and 256 ± 28 mm in the posterior approach (P = .09; Student t test). The mean difference in the length of the harvested semitendinosus tendon between the 2 approaches was 7 mm. The length of the gracilis tendon was 226 ± 29 mm and 223 ± 29 mm in the anterior approach and the posterior approach, respectively (P = .30; Student t test).
Conclusion:
In a retrospective 1:1 case-control study with exact matching of body height and sex, it was found that there was no difference in the length of the semitendinosus tendon and the gracilis tendon harvested using a posterior approach compared with an anterior approach. The mean difference between the 2 approaches was 7 mm for the semitendinosus tendon and 3 mm for the gracilis tendon, respectively.
The harvesting of the medial hamstring tendons in anterior cruciate ligament reconstruction (ACLR) is conventionally performed using an anterior approach, which involves the same incision as the preparation of the tibial tunnel of ACLR. Most surgeons prepare the ACLR graft by doubling the harvested semitendinosus and gracilis tendons. Some surgeons prefer to triple 15 or even quadruple the harvested grafts 3 to yield an ACLR graft of satisfactory diameter. Despite its being a safe procedure, complications can occur during harvesting of the medial hamstring tendons through the anterior approach, including premature graft rupture, unintentional graft harvesting, and injury to the infrapatellar branch of the saphenous nerve. 6 Premature graft rupture compromises the length of the harvested tendon, which is a concern when tripling or quadrupling the semitendinosus and gracilis tendons is required to produce an ACLR graft of adequate length and diameter.17,18
A posterior approach is proposed as an alternative method for harvesting the medial hamstring tendon graft during ACLR. 13 The potential benefits include a lower risk of premature graft rupture and unintentional graft harvest. 16 In the posterior approach, the harvesting of the medial hamstring tendons begins in the middle portion of the tendon, which has been recommended in order to increase the chance of harvesting the maximal length of the tendon. 13
Despite the proposal that adopting the posterior approach in harvesting medial hamstring tendons may theoretically increase the length of the harvestable tendon, 13 this potential advantage has not yet been proven. There is only 1 study in the adult population that compares the harvested tendon length between the anterior approach and posterior approach. 4 In a randomized controlled trial comparing anterior and posterior approaches in medial hamstring tendons harvesting, Franz and Baumann 4 reported that the length of the harvested semitendinosus tendon was on average 20 mm shorter in the posterior approach compared with the anterior approach. However, data concerning body height were not reported in the study by Franz and Baumann. It is known that body height is the most important factor in predicting the length of the harvested tendon.7,9 In the absence of data about body height, potential selection bias in the study by Franz and Baumann cannot be excluded. Additionally, even for the most carefully designed randomized controlled trial, exact matching of the body height between the 2 treatment arms is difficult unless the sample size is large enough.
To investigate whether there is a difference in the length of the harvested medial hamstring tendons between the anterior approach and posterior approach, a retrospective case-control matching study was conducted at the primary institution. The hypothesis was that there would be no difference in the length of the harvestable tendon between medial hamstring tendons harvesting done using an anterior approach and that using a posterior approach.
Methods
The current retrospective study was approved by the local ethics committee of the primary institution. The need for obtaining informed consent from the patients was waived by the local ethics committee.
A retrospective study was conducted for patients who underwent medial hamstring tendons harvesting between January 2008 and December 2021. The inclusion criteria were the following: harvesting of medial hamstring tendon autograft in the author’s institution between January 2008 and December 2021; patients who were Chinese; and patients who were skeletally mature. Exclusion criteria were graft-harvesting complications, including premature graft rupture, and if only 1, not both, medial hamstring tendons were harvested.
Patients were assessed in a preoperative assessment clinic 1 week before the ligament reconstruction surgery. The demographic data of the patients, including body height and body weight, were prospectively collected. Body height was measured to the nearest centimeter.
Case-Control Matching
A total of 676 medial hamstring tendon graft harvests were performed on skeletally mature Chinese patients at the primary institution between January 2008 and December 2021. Out of these, 573 patients underwent graft harvesting using the anterior approach, while 103 patients underwent the posterior approach. Among them, a total of 653 patients met the inclusion criteria, including 536 with the anterior approach and 58 with the posterior approach. A 1:1 matching ratio was performed between the patients receiving the anterior approach and those receiving the posterior approach with respect to the patients’ body height and sex, resulting in 54 exactly matched pairs (Figure 1).

Flowchart of patient inclusion criteria. ACLR, anterior cruciate ligament reconstruction; MPFLR, medial patellofemoral ligament reconstruction; PCLR, posterior cruciate ligament reconstruction.
Surgical Technique
The patient was positioned on the operation table in a supine position. General anesthesia with muscle relaxants was administrated. A pneumatic tourniquet was applied to the proximal thigh.
Harvesting of Medial Hamstring Tendons Through an Anterior Approach
With the knee flexed at a 90° angle, a longitudinal incision was made on the anteromedial aspect of the medial proximal tibia at the level of the tibial tuberosity. The subcutaneous tissue was dissected until the sartorial fascia was reached. The semitendinosus and gracilis tendons were located by palpation. An L-shaped incision was made in the sartorial fascia. The combined insertion of the medial hamstring tendons was sharply dissected from its attachment on the medial proximal tibia. The semitendinosus and gracilis tendons were separated from the sartorial fascia. The graft was harvested by removing its muscle in the proximal end using a closed tendon stripper (Figure 2). The surgeries were performed by 2 fellowship-trained sports medicine surgeons (including W.P.Y.).

Harvesting of the medial hamstring tendons through the anterior approach. A right knee with the harvesting of the medial hamstring tendons was done using an anterior approach. With the knee flexed at a 90° angle, a longitudinal incision was made on the anteromedial aspect of the medial proximal tibia at the level of the tibial tuberosity. The combined insertion of the medial hamstring tendons was sharply dissected from its attachment on the medial proximal tibia.
Harvesting of Medial Hamstring Tendons Through a Posterior Approach
The knee was flexed to approximately 20° to 30° of flexion. The hip was externally rotated to facilitate exposure of the popliteal fossa. The location of the medial hamstring tendons was palpated subcutaneously. A transverse incision was made at the posteromedial aspect of the popliteal fossa. The deep fascia was split, and the adipose tissue surrounding the tendons was removed. The middle part of the medial hamstring tendons was identified (Figure 3). The tendon was freed from its proximal muscle attachment using an open tendon stripper. Afterward, the tendon was extracted from the wound. The distal end of the tendon was then released from its tibial insertion using a closed tendon stripper. The surgeries were done by a single fellowship-trained sports medicine surgeon (W.P.Y.).

Harvesting of the medial hamstring tendons through the posterior approach. The knee was flexed to around 20° to 30° of flexion. The hip was externally rotated to facilitate exposure of the popliteal fossa. A transverse incision was made at the posteromedial aspect of the popliteal fossa. The middle part of the medial hamstring tendons was identified.
Measurement of the Tendon Length
The harvested tendon was prepared on a side table. The length of the harvested tendon was measured to the nearest 5 mm (Figure 4).

The length of the harvested tendon was measured. The tendon that was harvested was prepared on a side table. The length of the tendon was measured to the nearest 5 mm.
Statistical Analysis
The number of medial hamstring tendons harvesting using an anterior approach and a posterior approach was reported. Continuous data were compared using a Student t test, while categorical data were compared using a chi-square test. The length of the harvested tendons by the anterior approach and posterior approach was compared using a Student t test. Statistical significance was assumed when P < .05. Statistical analysis was performed using SPSS (Statistical Packages for the Social Science; Version 28; IBM).
Sample Size Analysis
The reported mean length of the semitendinosus tendon harvested using the anterior approach and the posterior approach in the study by Franz and Baumann 4 were 292 mm and 272 mm, respectively. The reported standard deviation was 31 mm. 9 Types 1 and 2 errors were set at .05 and .2, respectively. To detect a difference in length of 20 mm between harvesting through the anterior approach and through the posterior approach, a minimum of 38 samples were required in each group for an enrollment ratio of 1:1. Therefore, a total of 76 cases were required.
Results
All recruited patients were Chinese, and the graft harvesting was performed for ACLR. There were no demographic differences, including age, sex, laterality of the involved knee, body height, body weight, and body mass index, between patients who had hamstring tendons harvesting done using the anterior approach and those who had it using the posterior approach (Table 1).
Demographics of Patients a
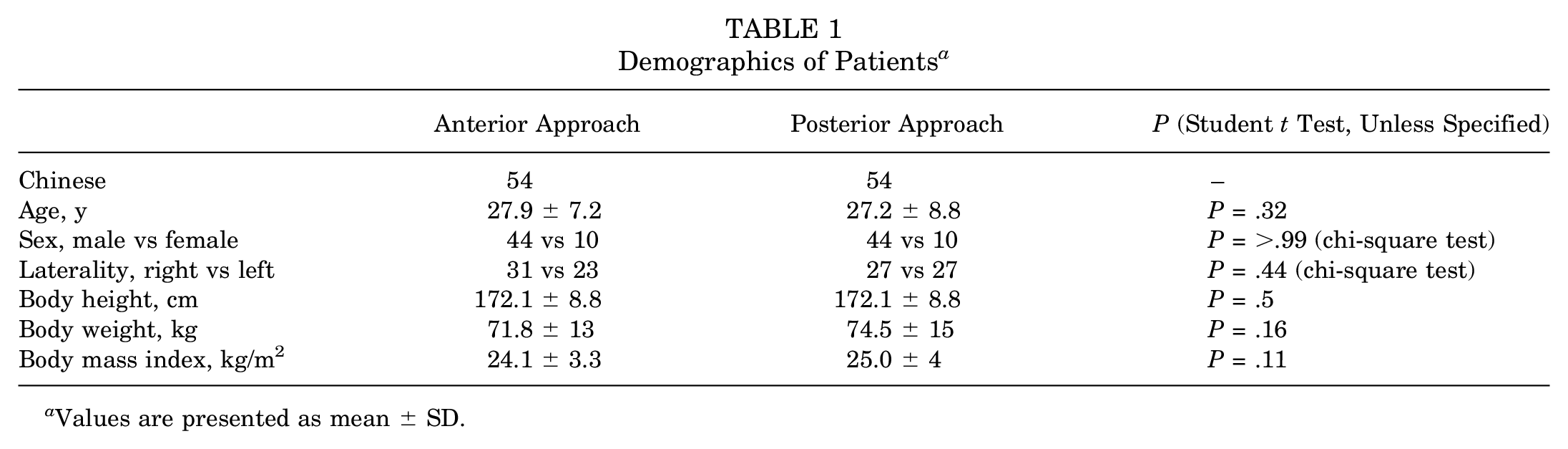
Values are presented as mean ± SD.
The length of the harvested semitendinosus tendon was 263 ± 29 mm in the anterior approach and 256 ± 28 mm in the posterior approach (P = .09; Student t test). The mean difference in the length of the harvested tendon between the 2 approaches was 7 mm. The length of the gracilis tendon was 226 ± 29 mm in the anterior approach and 223 ± 29 mm in the posterior approach (P = .30; Student t test).
Discussion
The most important finding of the current study was that there was no significant difference in the length of the semitendinosus and gracilis tendons when harvested using a posterior approach compared with an anterior approach (P = .09 and P = .30, respectively). The mean difference between the 2 approaches was 7 mm for the semitendinosus tendon and 3 mm for the gracilis tendon.
The medial hamstring tendon is one of the most harvested tendons for ACLR. Meta-analysis results suggest that failure after ACLR using medial hamstring tendons autograft is inversely related to the diameter of the graft.2,10 To minimize the chance of graft rupture, it is recommended that the implanted hamstring tendons autograft should have a minimum diameter of 8 mm. 11 However, several anthropometric studies have shown that a 4-stranded hamstring tendons autograft, prepared by doubling the semitendinosus and gracilis tendons, does not meet this requirement in a significant proportion of patients. The reported figure ranged from 5.8% to 16.9% in Caucasian patients9,14 and 43% to 77% in Asian patients.5,12 Short patients receiving ACLR are more prone to have a thin graft because body height is the most important factor in determining the diameter and length of the medial hamstring tendons.9,14,19 As a result, some surgeons triple 15 or even quadruple the harvested grafts to yield a graft of satisfactory diameter. 3 However, when quadrupling the graft, the length of the harvested tendon becomes a concern, especially if the patient is short.17,18 It would be beneficial to adopt a method of graft harvest that can yield the maximal length of the tendon.
The results of the current study showed that the difference in approaches during hamstring tendons harvest is not important in determining the length of the harvestable medial hamstring tendons. Franz and Baumann 4 found that the harvested semitendinosus tendon through the posterior approach was, on average, 20 mm shorter than that via the anterior approach. They suggested that surgeons could make a sharp dissection of the most distal insertion of the semitendinosus tendon off the tibia under direct vision in an anterior approach, allowing the whole length of the graft to be harvested. On the other hand, using a closed tendon stripper from the popliteal fossa in the posterior approach to release the semitendinosus tendon distally left a small cuff of the tendon behind, resulting in a shorter graft harvested in the posterior approach. 4 It is easier to harvest the entire tibial insertion of the semitendinosus in the anterior approach. Unlike the findings of Franz and Baumann, the mean difference in the harvested semitendinosus tendon between the anterior and posterior approaches in this study was only 7 mm. This difference is unlikely to result in a clinically important difference in the length of the ACLR graft, especially if the tendon is to be quadrupled. The possible reasons explaining the difference between the findings of our study and those of Franz and Baumann are the possible difference in the technique used to harvest the semitendinosus tendon using a posterior approach.The harvesting the distal end of the hamstring tendon from its tibial insertion was done with caution in this study. The end of the closed tendon stripper was palpated percutaneously before stripping the tendon from its tibial insertion to ensure that the harvesting yielded the maximal length of the tendon. Another possible explanation is the racial difference between the 2 studies in terms of the recruited patients and possibly their body height.
There are several advantages to adopting the posterior approach in harvesting the medial hamstring tendons. The incidence of saphenous nerve injury is lower in the posterior approach than in the anterior approach.1,4,8 Furthermore, the patient has a weaker chance of having nerve entrapment. With that said, there are benefits in terms of incision length and esthetics.1,8 For one, the time for graft harvesting is shorter. 4 The chance of unintentional tendon harvest is also smaller. 16 Additionally, the current study shows that there is no clinically important difference in the length of the harvestable semitendinosus and gracilis tendons between using anterior and posterior approa ches. Surgeons can choose the most appropriate approach in harvesting the medial hamstring tendons, considering potential complications, without worrying about the harvestable length of the tendon.
The harvesting of the medial hamstring tendons through a posterior approach has been recommended by some surgeons due to a lower risk of premature graft rupture. 16 Premature graft rupture occurred for both the semitendinosus and the gracilis tendons in the first 2 cases of graft harvest using a posterior approach in this study. This potential learning curve should be made clear when adopting the posterior approach in graft harvest. However, it is worth noting that despite the premature graft rupture, the semitendinosus and gracilis tendons harvested using a posterior approach are always long enough to allow doubling and result in a quadrupled hamstring ACLR graft long enough for graft fixation. The likely explanation is that the harvesting of the tendon starts in the middle part of the tendon, making it not difficult to harvest a ≥80 to 100 mm–long tendon from both the proximal and the distal ends of the tendon.
Limitations
The current study was a retrospective case-control study and had all the bias associated with retrospective research. However, the adoption of a 1:1 matching policy in body height and sex helped minimize possible selection bias. All the data, including the length of the harvested tendon, were prospectively collected under the same research protocol using a standard research documentation form. This helped reduce recall bias.
The harvesting of medial hamstring tendons through the anterior approach was done by 2 fellowship-trained sports medicine surgeons (including W.P.Y.), while the harvesting using a posterior approach was done by one of the surgeons (W.P.Y.) only. There was a difference in personnel and experience in performing hamstring tendons harvest between the 2 treatment arms. Both surgeons were trained in performing the harvesting of medial hamstring tendons using an anterior approach and were experienced in this procedure before the start of the study. However, the patients recruited for the harvesting using a posterior approach were the first 103 cases performed by a single surgeon (W.P.Y.). This limitation should be noted before extrapolating the results of the current study to clinical practice. Finally, patients were excluded if they had experienced graft harvesting complication.
Conclusion
In a retrospective 1:1 case-control study with exact matching of body height and sex, it was found that there was no difference in the length of the semitendinosus tendon and the gracilis tendon harvested using a posterior approach compared with an anterior approach. The mean difference between the 2 approaches was 7 mm for the semitendinosus tendon and 3 mm for the gracilis tendon, respectively.
Footnotes
Final revision submitted March 6, 2024; accepted April 9, 2024.
The author declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Hong Kong (UW No. 23-594).