
Abstract
Background:
Patients with large labral tears represent a subset of traumatic shoulder instability cases. Outcomes after arthroscopic stabilization in these patients have been studied less compared with other tears.
Purpose:
To establish minimal clinically important difference (MCID), Patient Acceptable Symptom State (PASS), and substantial clinical benefit (SCB) thresholds for patients after arthroscopic repair of labral tears ≥270°. Patient-reported outcome measures (PROMs) included the Rowe instability score, American Shoulder and Elbow Surgeons (ASES) score, Single Assessment Numeric Evaluation (SANE), and visual analog scale (VAS) for pain.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 52 arthroscopic large labral repairs (52 patients, mean age 28.7 years) performed in male active-duty military patients with a mean follow-up of 79.2 months (range, 24-117 months) met inclusion criteria and were included in the final analysis. All included patients completed the Rowe, ASES, SANE, and VAS pain preoperatively and at final follow-up, and the MCID, PASS, and SCB were calculated for each PROM score. Factors associated with achieving clinically relevant improvement were also calculated.
Results:
The MCID, PASS, and SCB, respectively, for each PROM were as follows: 10.4 points, 90, and 35 points for the Rowe; 9.7 points, 80, and 43 points for the ASES; 9.9 points, 87, and 65 points for the SANE; and 1.1 points, 3, and 6 points for VAS pain. More than 90% of patients improved according to the MCID for each PROM, while >75% achieved the PASS threshold for each score. The percentage of patients who improved according to the SCB ranged from 9.6% for the ASES to 75% for the SANE. Maintenance of active-duty status was associated with achieving the MCID for the ASES and SANE, while recurrent instability was associated with lower rates of Rowe MCID achievement and SANE PASS achievement. Higher preoperative scores were also associated with lower rates of achieving clinical improvement.
Conclusion:
Thresholds found for the MCID, PASS, and SCB in active-duty patients undergoing surgery for shoulder instability with labral tears ≥270° were similar to those for all-comers with anterior instability. Factors associated with achieving success or lack thereof on PROMs included maintenance of active-duty status and lower preoperative PROM scores.
Patient-reported outcome measures (PROMs) are critical for determining the success of surgical treatment of shoulder instability. Prior studies have investigated the thresholds for clinical success following shoulder procedures including arthroscopic Bankart repair,17,18 Latarjet procedure, 15 posterior labral repair, 23 and rotator cuff repair. 8 Shoulder instability represents a wide spectrum of pathology, with many options available for surgical stabilization, ranging from isolated arthroscopic Bankart repair to more complex arthroscopic or open procedures. Large labral tears (≥270°) represent a unique and uncommon subset of shoulder instability, and little has been published regarding outcomes and/or PROMs in the setting of these tears.
Large tears have a low prevalence compared with labral tears isolated to the anteroinferior labrum, and they are associated with male sex, contact-sport participation, and lower baseline PROM scores. 4 A recent study also found a higher prevalence of 270° tears in a military population. 7 The lesions may also be referred to as “triple tears,”“circumferential tears,” or “panlabral tears.” 5 This type of tear was initially described by Lo and Burkhart, 10 who observed anterior, posterior, and inferior labral tears in a small percentage of patients who underwent surgery for anterior instability. These tears typically lead to a primary complaint of anterior instability, but symptoms and/or additional complaints of posteroinferior instability may also be present. 14 Diagnosis of tears ≥270° based on physical examination and magnetic resonance imaging remains a challenge. 21 While magnetic resonance arthrography may help improve diagnostic rates and aid in preoperative planning, arthroscopic identification remains the most accurate method. 5
There is relatively little evidence regarding outcomes after repair of labral tears ≥270°. In a systematic review, Ernat et al 6 identified 6 studies reporting outcomes on a total of 128 patients with short- to midterm follow-up. Despite heterogeneity, these studies demonstrated generally satisfactory outcomes and return to sport ranging from 75% to 100%; however, there was a high rate of recurrent complications, primarily related to recurrent instability and the need for additional surgery.
The purpose of the current study was to investigate the threshold for clinical success based on shoulder-specific and instability-specific PROMs after arthroscopic stabilization of labral tears ≥270°. Specifically, the Rowe instability score, American Shoulder and Elbow Surgeons (ASES) score, Single Assessment Numeric Evaluation (SANE), and visual analog scale (VAS) for pain were evaluated. Success was determined based on whether patients met minimal clinically important difference (MCID), Patient Acceptable Symptom State (PASS), and substantial clinical benefit (SCB) thresholds.
Methods
Study Design
This study was a retrospective analysis of shoulder PROMs; institutional review board approval was obtained for the study protocol. All active-duty military patients who underwent arthroscopic labral repair for tears ≥270° between January 2011 and December 2019 by a single surgeon (N.P.) were screened for possible inclusion. All patients had anterior, inferior, and posterior labral tears. The outcomes for these patients have been previously reported in a separate study investigating outcomes after arthroscopic stabilization 7 ; the repair technique has also been previously described. 23 Patients were diagnosed with labral tears ≥270° if the tear pattern extended from the anteroinferior labrum posteriorly and superiorly to include the superior labrum. A trans–rotator cuff portal was used to place double-loaded suture anchors (Gryphon BR biocomposite suture anchors [DePuy Mitek] or Suturefix all-suture anchors [Smith & Nephew]). All knots were tied using cinch knots.
Outcome Measures
All patients completed the shoulder-specific PROMs (Rowe, ASES, SANE) and the VAS pain score both preoperatively and at follow-up. Pain level on the VAS was measured from 0 (no pain) to 10 (maximium pain).
Functional Outcome Evaluation
To determine the clinically significant threshold that corresponded to meaningful outcome achievement, the MCID, SCB, and PASS were calculated for the Rowe, ASES, SANE, and VAS pain utilizing either an anchor- or a distribution-based method. As many patients undergoing combined labral repair will have improvements in outcomes,11,12,25 the MCID was calculated utilizing a distribution-based method, using half of the standard deviation for the overall change in each outcome score across the entire cohort. Patients were classified as surpassing the MCID if their improvement in the outcome score was greater than the calculated MCID value.
The PASS was calculated using an anchor-based method. At final follow-up, patients were asked the following anchor question: “Taking into account all activities you have done during your daily life, your level of pain and also your functional impairment, do you consider that your current state is satisfactory?” 9 PASS values were then determined through receiver operating characteristic (ROC) curve analysis. The PASS threshold was determined by selecting the cutoff that maximized the Youden J statistic (defined as sensitivity+specificity– 1). Patients were classified as meeting the PASS if the value of the outcome score in question at final follow-up met or exceeded the cutoff score as calculated above.
Calculation of SCB was also performed using an anchor-based method. Prior evidence has demonstrated that questions related to both pain and physical function are acceptable as anchor questions to identify clinically meaningful improvements in pain and function. 16 To determine SCB for the functional outcome scores (Rowe, ASES, and SANE), patients were asked the following anchor question at final follow-up: “Since your surgery, how would you rate your overall physical activity?” To determine SCB for VAS pain, patients were asked the following anchor question at final follow-up: “Since your surgery, how would you rate your overall shoulder pain?” For all SCB measures, patients who answered much improved were considered substantially improved, while those who answered improved or slightly improved were considered improved. Patients who responded no change, slightly worse, or worse/much worse were considered unimproved. Using a similar ROC curve analysis methodology to that employed to calculate the PASS, the SCB threshold score was determined by selecting the absolute cutoff that maximized the Youden J statistic. Patients were classified as achieving SCB if the change in outcome score from preoperative state to final follow-up met or exceeded the cutoff score as calculated above.
Statistical Analysis
All statistical analyses were performed with RStudio 2023 (Posit, PBC). Descriptive statistics for continuous demographic data were reported as means ± SD, whereas frequency statistics were reported for categorical variables. Paired-samples t tests were used to compare preoperative and postoperative outcome scores. Statistical significance was set at α < .05. Nonparametric ROC and area under the curve (AUC) analyses were utilized to calculate the PASS and SCB based on the anchor-based method. The degree of association was considered acceptable if the AUC were >0.7 and excellent if >0.8. These values were then used to determine which patients in the cohort achieved the MCID, the PASS, and SCB.
Univariate analysis was performed with respect to each demographic characteristic and preoperative variable using the chi-square or Student t test for categorical and continuous variables, respectively. Multivariate logistical regression analysis was performed on variables that achieved a P value of <.05 during the univariate analysis. Only variables that reached significance in the univariate regression were further analyzed for multivariate analysis. If only 1 variable was present, no multivariate analysis was performed. Variables were considered significant predictors of achieving clinical significance if the final P value was <.05. Odds ratios (ORs) and confidence intervals were calculated for each demographic and preoperative variable with respect to achieving MCID, PASS, and SCB.
Results
Study Population
During the study period, 92 arthroscopic labral repairs for tears ≥270° were performed in 92 patients. Of these patients, 13 were treated for concomitant glenoid osteochondral lesions with microfracture and 19 patients were treated for concomitant rotator cuff tears with rotator cuff repair and excluded from further analysis. Furthermore, 8 patients were lost to follow-up, leaving a total of 52 patients with a mean follow-up of 79.2 months (range, 24-117 months) available for final analysis (Figure 1). Patient demographic characteristics and surgical data are summarized in Table 1. A statistically significant pre- to postoperative improvement was noted on all PROM scores (P < .001 for all) (Table 2). Four patients were discharged from active-duty service before final follow-up as they were unable to perform physical job demands due to pain, with 1 patient reporting subjective instability.

Flowchart of patient inclusion in this study.
Patient Characteristics and Surgical Data a

Data are expressed as mean ± SD or n (%). MOS, Military Occupational Specialty.
Defined as infantry, artillery, or military police occupations.
Comparison of Preoperative Versus 5-Year PROM Scores a
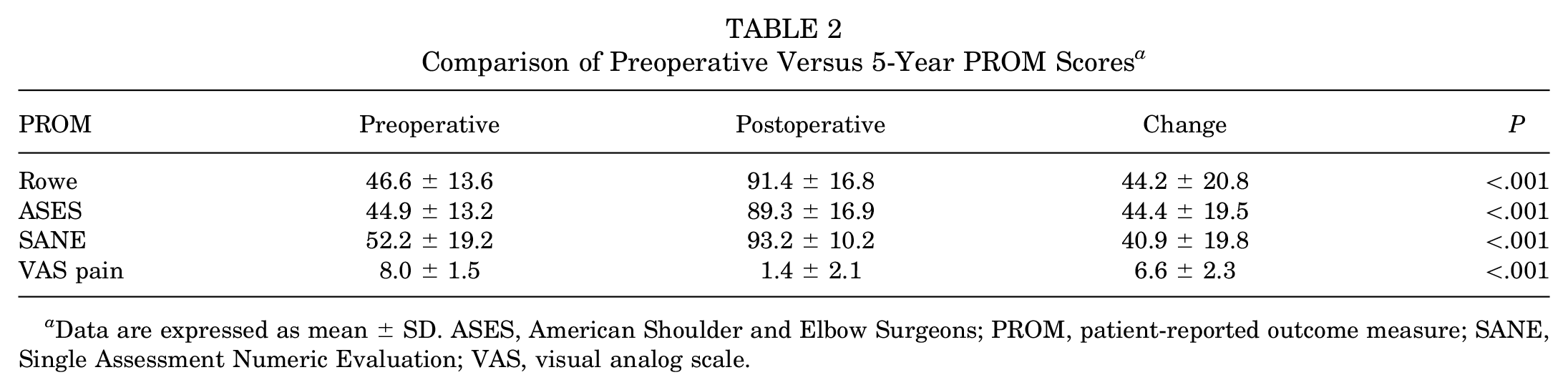
Data are expressed as mean ± SD. ASES, American Shoulder and Elbow Surgeons; PROM, patient-reported outcome measure; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Clinically Significant Outcomes
The calculated MCID, PASS, and SCB values for the Rowe, ASES, SANE, and VAS pain scores, in addition to the sensitivity, specificity, and AUC for the respective ROC curves (for the PASS and SCB), are summarized in Table 3. The frequencies with which patients in our cohort achieved clinically meaningful improvement based on the various outcome scores and values are summarized in Table 4.
MCID, PASS, and SCB Threshold Scores for the Included PROMs a

Data are expressed as n (%). ASES, American Shoulder and Elbow Surgeons; AUC, area under the curve; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; PROM, patient-reported outcome measure; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
Patients Who Achieved Clinically Significant Improvement at Final Follow-up a
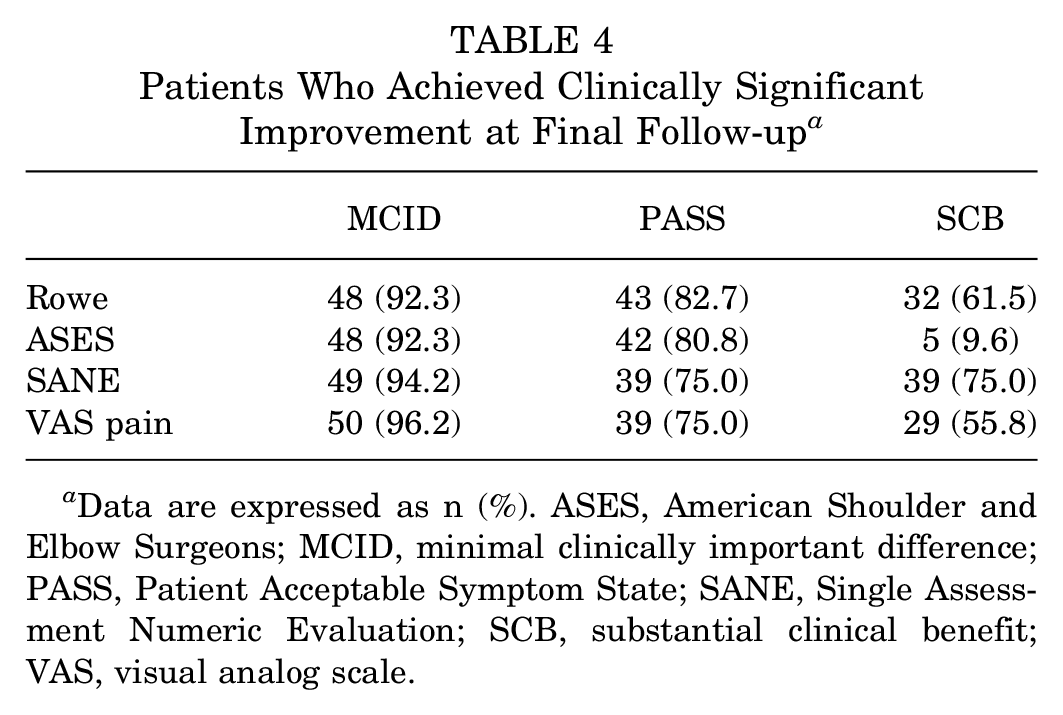
Data are expressed as n (%). ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
For achieving the MCID, recurrent instability (OR, 0.535; P < .001) was found to be a negative predictor for the Rowe score. Maintenance of active-duty status (OR, 1.879; P < .001) was found to be a positive predictor for the ASES score. Maintenance of active-duty status (OR, 1.939; P < .001) and higher preoperative Rowe score (OR, 1.004; P = .047) were found to be a positive predictor for the SANE, while a higher preoperative ASES score (OR, 0.994; P = .032) was found to be a negative predictor. Finally, maintenance of active-duty status (OR, 0.731; P = .006) was found to be a negative predictor for the VAS pain score (Table 5).
Logistic Regression of Factors Associated With Achieving the MCID a

ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; NA, not applicable; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale. Bold indicates p value < 0.05.
For achieving the PASS, recurrent instability (OR, 0.622; P = .042) was found to be a negative predictor on multivariate regression for the SANE, and a higher preoperative VAS pain score (OR, 0.942; P < .001) was found to be a negative predictor on univariate regression for the VAS pain score (Table 6).
Logistic Regression of Factors Associated With Achieving the PASS a

ASES, American Shoulder and Elbow Surgeons; NA, not applicable; PASS, Patient Acceptable Symptom State; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale. Bold indicates p value < 0.05.
For achieving SCB, a higher preoperative ASES score was found to be a negative predictor for the ASES (OR, 0.969; P = .033), while a higher preoperative SANE score was found to be a negative predictor for both the SANE (OR, 0.988; P = .001) and VAS pain score (OR, 0.989; P = .002) (Table 7). Predictors that reached statistical significance for >1 meaningful improvement metric are detailed in Table 8.
Logistic Regression of Factors Associated With Achieving SCB a

ASES, American Shoulder and Elbow Surgeons; MOS, Military Occupational Specialty; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale. Bold indicates p value < 0.05.
Notable Predictors for Achieving a Clinically Significant Outcome a
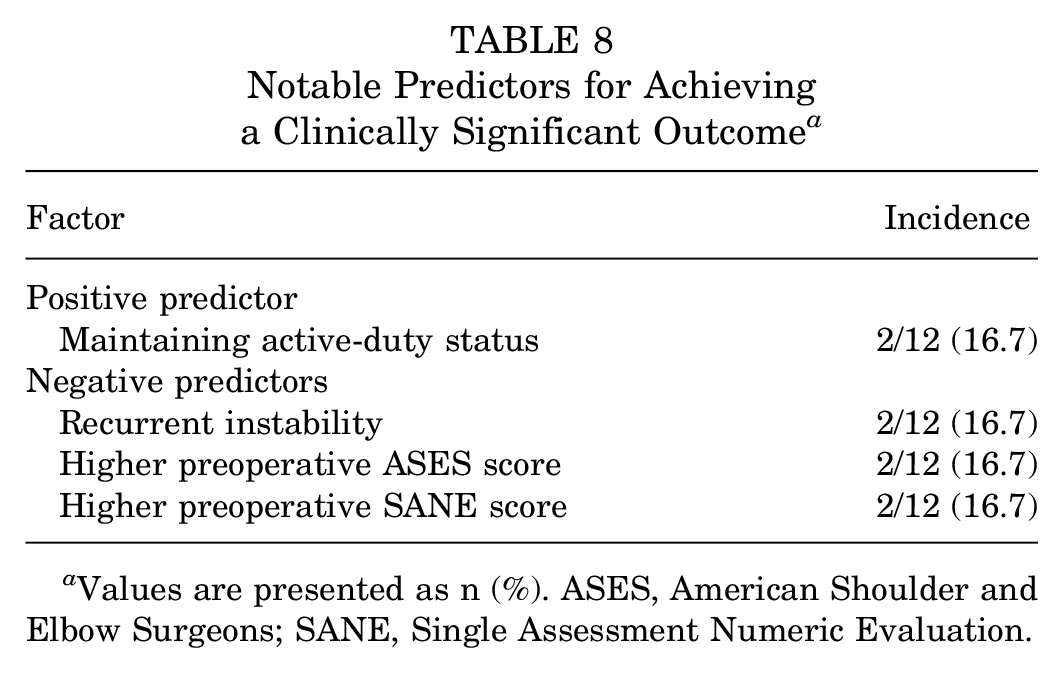
Values are presented as n (%). ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation.
Discussion
This study established measures of clinical significance for Rowe, ASES, SANE, and VAS pain scores after arthroscopic repair of labral tears ≥270°. For the Rowe score, an MCID of 10.4 was determined, along with a PASS score of 90 and SCB of 35. For the ASES, an MCID of 9.7 was calculated, with PASS of 80 and SCB of 43. The SANE showed an MCID of 9.9, with PASS of 87 and SCB of 65. VAS pain was found to have an MCID of 1.1, with PASS of 3 and SCB of 6. The models used to determine PASS were found to have high strength, with AUCs >0.9 for each model. Models for SCB were fair to high strength, with AUCs ranging from 0.589 (SANE) to 0.905 (VAS pain). We also investigated variables associated with achieving clinical significance for each of these metrics for each PROM. No factors were universally associated either positively or negatively with reaching significance; however, several factors were significant in multiple models. As labral tears ≥270° represent a unique subset of shoulder instability, the thresholds established in this study will help to determine levels of clinical success and factors associated with achieving outcomes.
Previous studies have sought to determine measures of clinical success for patients undergoing surgery for shoulder instability. Park et al 17 used the Western Ontario Shoulder Instability Index (WOSI) and Rowe score to evaluate 198 patients undergoing arthroscopic stabilization for anterior shoulder instability. Using an anchor-based method, they reported an MCID of 9.7 points for the Rowe score, and using a distribution-based method, they reported MCIDs of 5.6 and 151.9 points for the Rowe and WOSI, respectively. In a separate study, Park et al 18 investigated the MCID for the ASES, reporting an improvement of 8.5 points to be clinically relevant. Additionally, they found that patients with a greater number of preoperative dislocations, longer duration of symptoms, and those with Hill-Sachs lesions required a larger improvement in ASES score to feel clinical improvement. Our study found slightly higher MCIDs for the Rowe (10.4 vs 9.7 points) and ASES (9.7 vs 8.5 points) compared with the studies by Park et al 17 and Park et al, 18 respectively, possibly due to the more complex pathology involved in large tears. Menendez et al 15 investigated the MCID for multiple shoulder scores following Latarjet procedures for shoulder instability with bone loss. They found values of 9.6 points for the ASES, 12.4 points for the SANE, 1.7 points for VAS pain, and 254.9 points for the WOSI. Our study found similar values, although slightly lower for SANE (9.9 vs 12.4 points) and VAS pain (1.1 vs 1.7 points). These findings suggest that MCID following stabilization is very similar between isolated anteroinferior labral tears and larger tears extending to involve the posterior and superior labrum.
There is little reported on the PASS for shoulder instability. Complicating matters is the fact that shoulder instability encompasses a wide spectrum of severity and associated pathology. The Cleveland Clinic OrthoMiDaS Episode of Care (OME) Sports Medicine group 3 recently looked at predictors of PASS in 234 patients undergoing surgery for shoulder instability, of which the majority of procedures were arthroscopic and involved primarily the anteroinferior labrum. They found that 76.1% of patients responded yes to the PASS question, which correlated with a mean 25-point ASES improvement and a mean 40-point SANE improvement. Additionally, they found that combined tears extending beyond the anteroinferior labrum were associated with a lower rate of responding yes to the PASS question. On univariate analysis, patients with a PASS answer of yes had mean ASES scores of 93.2 and SANE scores of 91.6. Our study expanded on these findings by establishing a PASS threshold for these scores in combined tears, with a score of 80 for the ASES, 87 for the SANE, and 90 for the Rowe. Our study showed similar rates of achieving the PASS for these scores (80.8% for ASES, 75.0% for SANE), but interestingly, the defined thresholds were lower, suggesting that patients with combined tears may be satisfied with the results of surgical stabilization despite lower functional scores. They may be a result of patients with large labral tears experiencing prolonged duration of symptoms and delayed surgical treatment resulting from diagnostic challenges. This could also be due to the severity of preoperative symptoms leading to higher satisfaction with lower postoperative scores compared with the scores required to achieve satisfaction after repair of smaller lesions.
SCB is a metric that has previously had little investigation with regard to shoulder instability. This metric of clinical improvement has been investigated more heavily in shoulder arthroplasty; however, significant variation has been noted with time from surgery and geographic region of patients undergoing surgery. 24 Alben at al 1 looked at Patient-Reported Outcomes Measurement Information System (PROMIS) scores for patients undergoing arthroscopic rotator cuff repair, finding that SCB scores were slightly higher than MCID scores (10.9 vs 9.0). 1 Puzzitiello et al 20 looked at the ASES, SANE, and Constant-Murley scores in patients treated with biceps tenodesis. For the ASES, they found MCID, SCB, and PASS thresholds of 11.0, 16.8, and 59.6, respectively, with 3.5, 5.8, and 65.5 for the SANE. For the scores evaluated in our study, the SCBs ranged from 3.4 times the MCID for the Rowe score to 6.5 times for the SANE. These results demonstrate that, while a clinically relevant change may be detectable, a greater improvement in PROM scores may be needed before a patient is satisfied to a high degree after treatment for more complex pathology, such as instability resulting from large labral tears. Manderle et al 13 investigated the time required to achieve clinically significant improvement, finding that most patients achieved MCID for the ASES, SANE, and Constant scores after rotator cuff repair by 6 months after surgery. It is unknown whether the duration to obtain clinical success based on PROMs may be longer based on complexity of procedure and extent of pathology in shoulder instability. All PROMs included in our analysis were evaluated ≥1 year after surgery.
Our study also investigated factors associated with achieving clinical improvement. We found achieving the MCID for the ASES and SANE scores was associated with remaining on active duty. Active-duty status has been previously studied in posterior shoulder instability, with a recent study reporting clinical improvement, low recurrence, and a high rate of return to active duty following arthroscopic stabilization. 22 Recurrent instability was associated with lower rates of improvement by the MCID for the Rowe and for achieving PASS scores for the SANE. Recurrent instability remains a challenge to treat, with options including bony procedures or more extensive soft tissue stabilization.2,9,19 We also found that higher preoperative ASES and SANE scores were negatively associated with achieving SCB on the same outcome, likely related to the smaller margin for functional score increase in patients with higher baseline scores.
Limitations
Limitations of our study include the relatively small overall sample size, although the infrequency of tears ≥270° within the larger population of shoulder instability makes our study one of the larger on this specific topic. This was also a retrospective study, subjecting it to potential biases and flaws inherent to all retrospective reviews. PROMs were collected at a mean follow-up of 79 months rather than at a single standardized time point. All patients underwent surgery by a single surgeon, which may affect generalizability. Patients came from an active-duty military population and were primarily male, which also potentially limits generalizability. External validity is likely limited given the demands that active-duty military status placed on the shoulder.
Conclusion
This study identified MCID, PASS, and SCB thresholds for the Rowe, ASES, SANE, and VAS pain scores in male active-duty military patients undergoing arthroscopic stabilization for anterior shoulder instability associated with labral tears ≥270°. These patients represent a subset of shoulder instability patients with more severe soft tissue pathology, although thresholds were similar to patients with anterior shoulder instability. Factors associated with achieving clinically significant improvement on the evaluated PROMs included maintenance of active-duty status and lower preoperative PROM scores. These results provide context for assessing postoperative patient improvement in this specific subgroup of shoulder instability patients.
Footnotes
Final revision submitted April 8, 2024; accepted April 17, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.P.S. has received hospitality payments from Stryker. B.R.C. has received hospitality payments from Stryker. C.M.H. has received honoraria from Wright Medical. N.P. has received consulting fees from DePuy Synthes. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Carthage Institutional Review Board (reference No. 2023-001).