
Abstract
Background:
Rotator cuff calcific tendinitis is a common shoulder joint disorder. Nonsurgical treatment methods, including multiple needling and extracorporeal shock wave therapy (ESWT), can effectively treat calcific tendinitis.
Purpose:
To evaluate the clinical results and radiological outcomes of treatment with ultrasound-guided needling (UGN) alone versus UGN with high-energy ESWT (UGN-H) or UGN with low-energy ESWT (UGN-L) in patients with calcific tendinitis of the rotator cuff.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Outpatient records for patients with calcific tendinitis of the rotator cuff were evaluated retrospectively. Patients were grouped into those treated with UGN-H, UGN-L, or controls with UGN alone. The visual analog scale (VAS) for pain, American Shoulder and Elbow Surgeons (ASES) scores, Constant-Murley scores, and radiographic evaluation to assess calcification size were available before treatment and at 3, 6, and 12 months after the first treatment. Post event pairwise analysis to analyze score differences between treatment groups was used.
Results:
Overall, 130 patients were included for analysis (42 UGN-H, 44 UGN-L, and 44 with UGN alone). At 3 months, the VAS scores were UGN-H (4.13 ± 0.84; P < .001) and UGN-L (4.47 ± 1.01; P < .001) which were significantly better than UGN alone (5.35 ± 1.00) in terms of the VAS score; however, the difference was not significant between UGN-H and UGN-L. These differences persisted at months 6 and 12 (6 months: UGN-H, 2.66 ± 1.00; P < .001; UGN-L, 3.16 ± 1.05; P = .033; 12 months: UGN-H, 1.93 ± 0.43; P < .001; UGN-L, 2.04 ± 0.46; P < .001). The results of the ASES and Constant-Murley scores were similar to those of the VAS score. In terms of radiographic outcome, follow-up at months 3, 6, and 12 revealed that UGN-H and UGN-L were superior to UGN alone at removing calcification (median 95% CI; 3 months: UGN-H, 1.4 mm2 [1.08, 7.25 mm2); P = .002; UGN-L, 5.79 mm2 (1.17, 7.85 mm2]; P = .041; 6 months: UGN-H, 0.91 mm2 [0, 1.15 mm2); P < .001; UGN-L, 1.13 mm2 [0.84, 5.10 mm2]; P < .001; 12 months: UGN-H, 0 mm2 [0, 0 mm2]; P < .001; UGN-L, 0 mm2 (0, 4.33 mm2]; P = .023). There was no significant difference between UGN-H and UGN-L at the month 3 follow-up, but the month 6 and 12 follow-ups revealed that UGN-H was more effective at removing calcification compared with UGN-L.
Conclusion:
The study demonstrated that, for pain relief and recovery of shoulder joint function, UGN + ESWT was significantly superior to UGN alone. No significant difference was observed between different energy levels of ESWT. UGN + ESWT was significantly superior to UGN alone on radiographic evaluation. Furthermore, UGN-H performed better radiographically with reducing calcifications compared with UGN-L at 12 months.
Calcific tendinitis is a condition in which calcium carbonate hydroxyapatite crystals are formed in tendons, causing inflammation and decreased mobility.1,2 It occurs mainly in the supraspinatus tendon.2,3,7 The incidence of calcific tendinitis in asymptomatic shoulder arthritis is 2.7% to 20%, and that in rotator cuffs is as high as 54% in patients with shoulder joint pain.2,7,11,29 Calcific tendinitis occurs mostly in the age group of 30 to 50 years and is more frequent on the right side.7,17 The incidence rate of calcific tendinitis is 1.5 times greater in women than in men. 17 Its pathogenesis is not very clear. The basic pathological reaction process is divided into 3 distinct stages: precalcification, calcification (formation and absorption phase), and postcalcification. 21 Symptoms are typically most noticeable at the absorption point. 22 Patients have the best probability of nonsurgical recovery at this stage. 22
Treatment can be divided into nonsurgical and surgical treatments. Nonsurgical treatment includes observation, oral nonsteroidal anti-inflammatory drugs (NSAIDs), steroid injections, physical therapy, multiple needling, and extracorporeal shock wave therapy (ESWT).4,5,19,27 Surgical treatment includes open removal of calcification and arthroscopic debridement of calcification.5,6,20 Multiple needling can reduce the internal pressure of the tendon and promote the absorption of calcifications to relieve symptoms.4-6,8 Some researchers believe that the therapeutic effect of multiple needling is equivalent to the arthroscopic debridement of calcifications, and multiple needling has no risk compared with surgery.5,6,8 When conservative treatments fail, more invasive treatments like ESWT and ultrasound-guided needling (UGN) are used as alternatives to surgery for the treatment of calcific tendinitis.1,18 ESWT can relieve pain through direct mechanical disintegrating effect, long-lasting hyperstimulation analgesia, and cellular mechanisms.4,16,24 Based on the different energy flux density (EFD), ESWT can be classified into low-energy shock waves (EFD < 0.28 mJ/mm2) and high-energy shock waves (EFD > 0.3 mJ/mm2). Several studies have confirmed that ESWT is effective in treating calcific tendinitis and can dramatically increase the joint function of the shoulder.10,12,15 The difference in the therapeutic effect of UGN combined with ESWT with different energy densities on calcific tendinitis is still not conclusive.
The main purpose of this study was to evaluate the clinical and radiological effects of UGN + ESWT with 2 different energy levels compared with UGN alone in the treatment of chronic calcific tendinitis. We hypothesized that UGN + high-energy ESWT (UGN-H) or low-energy ESWT (UGN-L) would result in better pain and functional scores and better radiological outcomes compared with UGN alone. We also hypothesized that UGN-H would perform better compared with UGN-L on radiologic outcomes.
Methods
This retrospective cohort study was performed using a sports medicine outpatient clinic database. A retrospective query of our institution was performed to identify patients with a history of calcific tendinitis (ICD10: M75.300), presenting with shoulder pain and limited shoulder motion, who underwent 1 of 3 interventions (UGN alone, UGN-H, or UGN-L) between 2011 and 2016 with complete preprocedure and minimum 1-year postoperative patient-reported outcome measures. The radiograph readers were blinded to the treatments the participants received. Our study was approved by the ethics committee of the Second Hospital of Jilin University (No. 2016-101). Inclusion criteria were as follows: (1) age >18 years; (2) symptomatic patients with calcific tendinitis of the rotator cuff diagnosed by radiograph; (3) a longest axis of calcification >20 mm, with morphologic type 1 and type 2 deposits corresponding to the classification of Gärtner and Simons 9 (radiographs were viewed by the same specialist reader); (4) previous treatment was ineffective, including use of oral NSAIDs, physical therapy and intra-articular cortisone injections; and (5) duration of symptoms exceeded 3 months. Exclusion criteria were as follows: (1) patients with full-thickness tear of rotator cuff tendon as confirmed by magnetic resonance imaging or ultrasound; (2) medical or radiographic signs of resorption process described as a recent duration of increased pain in conjunction with a morphological type 3 deposit (cloudy and translucent in structure) on radiographs; (3) osteoarthritis of the glenohumeral or acromioclavicular joint, adhesive capsulitis, instability of the shoulder, rheumatoid arthritis, and neurologic disorders or dysfunction of the upper limb; (4) previous shoulder surgery; and (5) patients with cognitive impairment or memory loss who could not be tracked.
The patients were divided into 3 cohorts: UGN-H, UGN-L, or UGN alone, depending on the type of intervention administered to them.
Extracorporeal Shock Wave Therapy
In this study, ultrasound was used to locate calcifications with the patient placed in the seated position. The patient first adapts with a lower energy pulse and is treated with the target energy density. The patients were treated with 2 sessions of ESWT at a 2-week interval. The energy density for high- and low-energy ESWT was 0.302 and 0.16 mJ/mm2, respectively (4 Hz, 1500 impact frequency).
Ultrasound-Guided Needling
Ultrasound is used to make a radiation-free 3-dimensional localization and evaluation of the calcific deposit. Supported by real-time ultrasonic guidance, the deposit is further needled and irrigated with saline and aspirated to break it away. This method essentially extracts a part of the calcific deposit and facilitates further reabsorption of the calcific content. Our study used the double-needle technique to reset and extract the calcification. Before starting the operation, we used 70% alcohol solution to disinfect the ultrasound transducer. The patient was placed in the supine position. After sterile prepping (7.5%-10% iodopovidone solution and benzalkonium chloride solution) and draping of the surgical area, local anesthesia (2% lidocaine 100 mg + 0.5% bupivacaine 25 mg) was administered to the skin and subcutaneous tissue. Most of the anesthetic drug solution is injected into the subacromial-subdeltoid bursa, and the remaining solution is injected into the subcutaneous tissue and around the calcification lesions. Under the guidance of ultrasound, a puncture needle (18-gauge) was used to puncture the calcified foci repeatedly at different angles and the area was irrigated with normal saline to break down calcification (Figure 1). The 2 needles were inserted as parallel to the ultrasound machine probe as possible. The angle between the needles is 25° to 30°, with the bevel of the first needle rotating upward and the bevel of the second needle rotating downward, with the bevels of the 2 needles facing each other. In this process, a part of the sediment is removed, and reabsorption of the remaining calcifications is promoted. We did not use steroids in place of saline because previous studies have demonstrated that the effect of injectable steroids is limited to posttreatment pain relief. 5 After the procedure, the needle entry point was sterilized again, and a sterile dressing was used to cover the needle entry site.
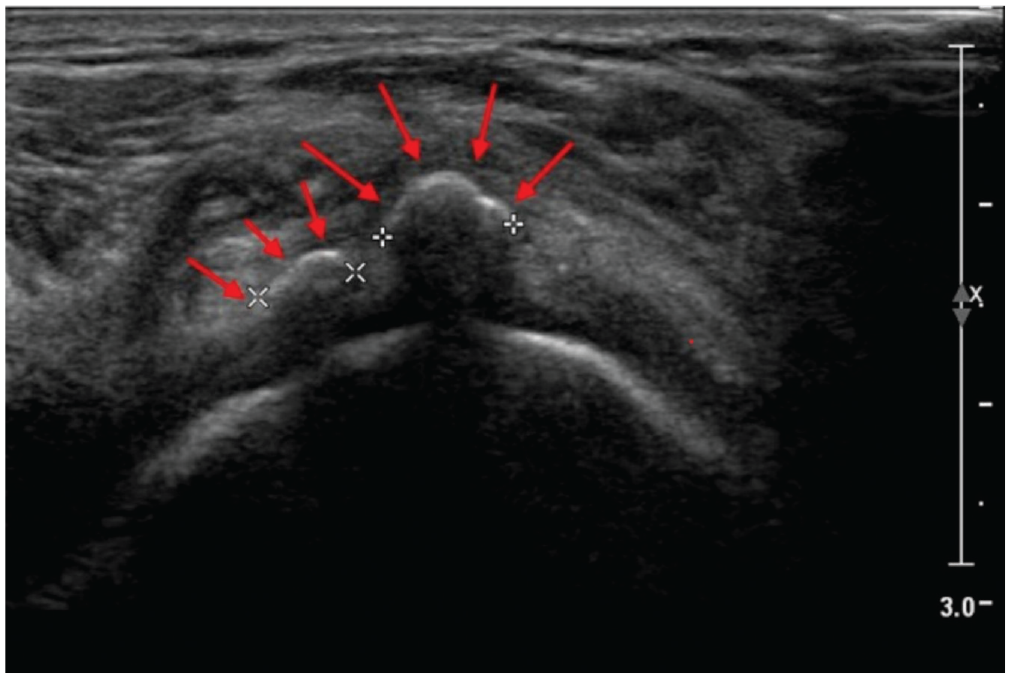
Ultrasound image of the supraspinatus muscle in calcific tendinitis, showing the lobed calcific deposit (red arrows) with partial acoustic shadow.
In this study, patients undergoing UGN-H or UGN-L were first treated with ESWT (2 treatment sessions; treatment interval of 2 weeks). After the pain and swelling vanished (interval usually 1 week), the patients underwent a UGN intervention.
Management of Postoperative Analgesia
Patients were advised to take nonprescription analgesics for postprocedure pain. Routine use of the shoulder is tolerated without limits, but the patient is asked to have a relative rest (arm no higher than shoulder) for 15 days. Approximately 10 days after treatment, all patients can start a routine home-based physiotherapy program. Before beginning the program, a physiotherapist shows patients how to perform activities correctly. The patients are expected to maintain a daily regimen for 15 days, during which each training session is documented with the date and number of exercises conducted.
Data Collection
Baseline demographic data (age, sex, the affected side, location and size of calcific deposits, and body mass index); duration of complaints; Gärtner radiological grade of calcific deposits; and degree of shoulder pain reported on a visual analog scale (VAS) from 0 to 100 mm, the American Shoulder and Elbow Surgeons (ASES) scale, and Constant-Murley scores were collected.
At given timepoints after the first treatment (3, 6, and 12 months), we collected information on VAS score (primary outcome), ASES score, Constant-Murley score, and causes of treatment discontinuation. Radiographs (neutral, internal, and external rotation) were used to evaluate the changes in the shape, location, and size of the calcification in each checkpoint. The radiographic images were all reviewed by 2 experienced orthopedic surgeons (W.Z. and X.L.) who were blinded to patient treatment. The decrease in deposit size of calcification was classified qualitatively into no change, partial resorption, and complete resolution. Adverse events such as subacromial bursitis, infection, and frozen shoulder were recorded.
Statistical Analysis
Data were analyzed using SPSS software (Version 24.0; IBM Corp). To verify the adequacy of the sample size, we conducted a power analysis using G*Power Version 3.1.9.7 (Heinrich-Heine-Universität Düsseldorf). The confidence level for each group was 95%, the efficacy factor was 0.8, the alpha level was .05, and the effect size was 0.3, which led to the calculation of a sample size of 111 patients. Based on the available sample size, the calculated power was 86.6%, making our sample size adequate. The distribution of the data was analyzed for normality using the Kolmogorov-Smirnov test. The equality of variances was confirmed using the Hartley test. Differences in mean scores between groups were assessed using 1-way analysis of variance (normally distributed data), and ordinal variables were analyzed using Fisher exact test and Pearson chi-square test. Differences between groups were compared using Bonferroni correction in post event pairwise analysis (P ≥ .05 was considered statistically nonsignificant and P < .05 was considered statistically significant).
Results
Characteristics of the Study Population at Baseline
A total of 162 patients with calcific tendinitis were treated; 32 patients were lost to follow-up and excluded (12 UGN-H; 10 UGN-L; 10 UGN alone). Overall, 130 patients with calcific tendinitis were included who met all the inclusion criteria (42 UGN-H; 44 UGN-L; 44 UGN alone). Baseline patient characteristics are presented in Table 1. The baseline data of each group were compared.
Patient Demographics and Baseline Values of Considered Outcomes a

Data are presented as mean ± SD, frequency counts (%). ANOVA, analysis of variance; ASES, American Shoulder and Elbow Surgeons; BMI, body mass index; CMS, Constant-Murley score; ESWT, extracorporeal shock wave therapy; F, female; L, left; M, male; R, right; UGN, ultrasound-guided needling; UGN-H, UGN with high-energy ESWT; UGN-L, UGN with low-energy ESWT; VAS, visual analog scale.
Pearson chi-square test.
One-way ANOVA.
Fisher exact test.
Primary Outcome: VAS
As the primary outcome, the means of the VAS scores for 3-, 6-, and 12-month follow-up after treatment are presented in Table 2. Compared with baseline data, the VAS scores measured in the 3 follow-up nodes after treatment were improved significantly. In a secondary analysis after Bonferroni correction, patients treated with UGN + ESWT performed significantly better on VAS for pain scores compared with patients in the UGN alone group at 3-, 6-, and 12-month follow-up (3 months: UGN-H, 4.13 ± 0.84; P < .001; UGN-L, 4.47 ± 1.01; P < .001; 6 months: UGN-H, 2.66 ± 1.00; P < .001; UGN-L, 3.16 ± 1.05; P = .033; 12 months, UGN-H, 1.93 ± 0.43; P < .001; UGN-L, 2.04 ± 0.46; P < .001). UGN-H appeared to be superior to UGN-L; however, the VAS difference was not significant (UGN-H, 1.93 ± 0.43; UGN-L, 2.04 ± 0.46; P = .812). The trends of the 3 treatment groups are shown in Figure 2.
Primary Clinical Outcome Measure a

Data are presented as mean ± SD unless otherwise indicated. ANOVA, analysis of variance; CI, confidence interval; ESWT, extracorporeal shock wave therapy; UGN, ultrasound-guided needling; UGN-H, UGN with high-energy ESWT; UGN-L, UGN with low-energy ESWT; VAS, visual analog scale.
P values were obtained from a 1-way ANOVA. In groups determined to be significantly significant, a Bonferroni correction was applied to test for individual intergroup comparison with results summarized by presenting the point estimate (95% CI).

Development of the VAS for pain score after treatment. Data are presented as mean ± SD. b, baseline; ESWT, extracorporeal shock wave therapy; UGN, ultrasound-guided needling; UGN-H, UGN with high-energy ESWT; UGN-L, UGN with low-energy ESWT; VAS, visual analog scale.
Secondary Outcomes: ASES, CMS
In case of secondary outcomes for months 3, 6, and 12, the 3 treatments were not significantly different in terms of ASES score. In a secondary analysis after Bonferroni correction, UGN-H and UGN-L exhibited significantly greater ASES scores compared with UGN; however, no significant difference was observed between UGN-H and UGN-L groups (Table 3 and Figure 3).
Secondary Clinical Outcome Measures a

Data are presented as mean ± SD unless otherwise indicated. ANOVA, analysis of variance; ASES, American Shoulder and Elbow Surgeons; CI, confidence interval; CMS, Constant-Murley score; ESWT, extracorporeal shock wave therapy; UGN, ultrasound-guided needling; UGN-H, UGN with high-energy ESWT; UGN-L, UGN with low-energy ESWT.
P values were obtained from a 1-way ANOVA. In groups determined to be significantly significant, a Bonferroni correction was applied to test for individual intergroup comparison with results summarized by presenting the point estimate (95% CI).
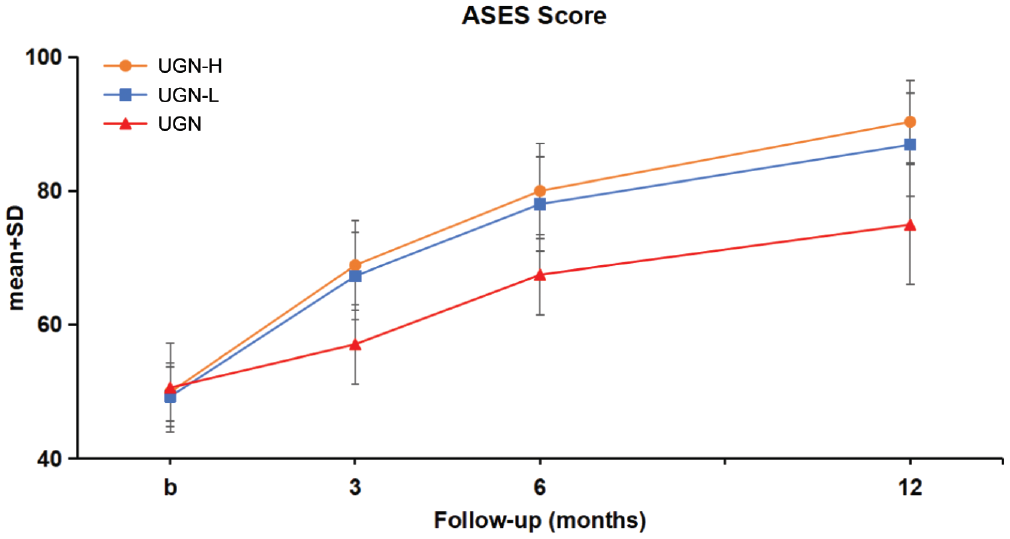
Development of the ASES score after treatment. Data are presented as mean ± SD. b, baseline; ASES, American Shoulder and Elbow Surgeons; ESWT, extracorporeal shock wave therapy; UGN, ultrasound-guided needling; UGN-H, UGN with high-energy ESWT; UGN-L, UGN with low-energy ESWT.
For the Constant-Murley score, the follow-up results were similar to those of the ASES score, with significant differences between the 3 groups in months 3, 6, and 12. After Bonferroni correction, UGN-H and UGN-L groups performed significantly better compared with the UGN group; however, no significant difference was observed between the UGN-H and UGN-L groups (Table 3 and Figure 4).

Development of the Constant-Murley score after treatment. Data are presented as mean ± SD. b, baseline; ESWT, extracorporeal shock wave therapy; UGN, ultrasound-guided needling; UGN-H, UGN with high-energy ESWT; UGN-L, UGN with low-energy ESWT.
Regarding the radiographic appearance of calcification, the 3 groups of patients exhibited considerable improvement around the 3-month follow-up, and significant differences were observed between the 3 groups. Post hoc analysis showed that UGN + ESWT performed significantly better compared with UGN alone in terms of reabsorption of calcification, but no significant difference was observed between different energy levels (Table 4). At the 6-month follow-up, most of the patients’ calcifications had disappeared completely (Figure 5), and significant differences were observed between the 3 groups. Post hoc analysis showed that UGN + ESWT performed significantly better compared with UGN alone in terms of reabsorption of calcifications. There was no statistical difference between different energy levels (Table 5).
Comparison of Changes in Size of Calcification a

CI, confidence interval; ESWT, extracorporeal shock wave therapy; UGN, ultrasound-guided needling; UGN-H, UGN with high-energy ESWT; UGN-L, UGN with low-energy ESWT.
Data are presented as median (25th, 75th percentiles).
Pairwise treatment comparisons were performed using nonparametric methods with results summarized by the P value for the Kruskal-Wallis test.

Radiographic images of the shoulder joint of the same patient showing calcifications (black arrow) before treatment (left panel) that disappeared completely (black arrow) after treatment (right panel).
Resorption of Calcific Deposits After 12 Months of Follow-up a

Data are presented as frequency counts (%). ESWT, extracorporeal shock wave therapy; UGN, ultrasound-guided needling; UGN-H, UGN with high-energy ESWT; UGN-L, UGN with low-energy ESWT.
Pairwise treatment comparisons were performed using nonparametric methods with results summarized by the P value for the Kruskal-Wallis test.
Overall, there were no obvious adverse events and serious complications during the follow-up period. After treatment, 4 patients developed persistent pain (3 patients with UGN-H and 1 patient with UGN-L), and 1 patient developed subacromial bursitis (UGN-H). All patients had symptom relief after taking oral NSAIDs.
Discussion
Our study demonstrated that, after 12 months of follow-up, the 3 groups of patients exhibited satisfactory outcomes without significant complications. The major findings of our study demonstrated that UGN + ESWT was much more effective compared with UGN alone when restoring shoulder joint function and alleviating pain (12 months: UGN-H, 1.93 ± 0.43; P < .001; UGN-L, 2.04 ± 0.46; P < .001) and UGN-H and UGN-L had similar effects (P = .812). In terms of clearing calcification, the benefit of UGN + ESWT was significantly superior to UGN alone (respectively, P = .002; P = .041), and the effects of UGN-H and UGN-L were similar (P = .832). However, the long-term (>12 months) efficacy in removing calcification may be greater after UGN-H than that after UGN-L. Further research is needed to support this finding.
The efficacy of UGN and ESWT in the treatment of calcific tendinitis has been confirmed in previous studies. In a randomized controlled trial of 48 patients, De Witte et al 7 reported that, during the 1-year follow-up period, UGN lavage + subacromial steroid injection was better compared with simple subacromial steroids in the treatment of calcific tendinitis hormone injection. In a randomized controlled trial with 54 patients, Kim et al 13 reported that UGN was more effective than ESWT in the treatment of calcific tendinitis. In a prospective study, Daecke et al 4 found that, during a 6-month follow-up period, high-energy ESWT was effective in treating calcific tendinitis, and the effect was better after receiving 2 sessions than after only 1 session. The study did not further explore the effects of different energy ESWT treatments. Some studies have confirmed that high-energy ESWT is superior to low-energy ESWT.26,28 However, the comparison of the effects of ESWT of different energies + UGN has not yet been studied. This study aimed to compare different energy levels of ESWT with UGN in the treatment of calcific tendinitis.
UGN treatment and ESWT treatment have certain curative effects, and the combined effect of the 2 treatment methods garners the interest of many surgeons. In a study involving 66 patients, Pakos et al 23 found that UGN + ESWT was effective in treating calcific tendinitis, but patients were followed up for only 1 month and no control group was designed. The level of evidence was low. 23 Krasny et al 14 designed a randomized controlled trial and found that, compared with simple ESWT treatment, UGN + ESWT treatment had a 50% increase in the reabsorption of calcific tendinitis calcification. However, the study used only high-energy ESWT. No further research has been done on the efficacy of low-energy ESWT. 14 Compared with the recent related literature in this field, there is no research on the effect of UGN + different energy ESWT on the treatment of calcific tendinitis. UGN and ESWT have different principles for treating calcific tendinitis. After treatment of ESWT, calcification will be broken or loose. At this time, if the patient receives further treatment with UGN, the calcification may be removed more thoroughly. In this study, the high-energy ESWT group may have had smaller residual calcifications, but there was no statistical difference in the remaining area of calcification foci between the 2 groups.
Use of steroids in UGN treatment in treating calcific tendinitis of the rotator cuff remains controversial. Steroids can relieve pain after treatment but may affect the reabsorption of calcification and the healing of rotator cuffs. A 12-month randomized controlled trial found no significant difference in UGN treatment using normal saline in place of steroids, but the role of steroids was limited to 6 weeks after the treatment improved pain. 5 Therefore, all UGN treatments in this study used normal saline lavage. At present, the methods of UGN and ESWT positioning mainly include the most painful part of the patient and auxiliary positioning technology (ultrasonic positioning, fluoroscopy positioning, etc). A study compared the effects of positioning the maximum pain point and auxiliary positioning after the treatment of calcified tendons and found that the effect of auxiliary technology positioning treatment was significantly superior to the maximum pain point positioning. 25 Our study used ultrasound positioning technology in UGN and ESWT treatment.
Limitations
This study has some limitations. First, this is a retrospective study. This study did not set up a nonsurgical treatment group as a control group. Because calcific tendinitis is self-limiting, adding a nonsurgical treatment group would complement the current study's results. Second, only 130 patients were involved in our analysis, and further survey work is required. Third, we included 12 months of follow-up, and a study with longer-term follow-up is to be performed. Fourth, although all baseline data in this study were comparable, there may still be other unknown confounding factors and there are statistical differences between these confounding factors.
Conclusion
Our study demonstrated that, for pain relief and recovery of shoulder joint function, UGN + ESWT was significantly superior to UGN alone. No significant difference was observed between different energy levels of ESWT. UGN+ ESWT was significantly superior to UGN alone on radiographic evaluation. Furthermore, UGN-H radiographically performed better with reducing calcifications compared with UGN-L at 12 months.
Footnotes
Final revision submitted February 28, 2024; accepted March 18, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from the 2023 Science and Technology Project of the Jilin Provincial Department of Education (JJKH20231226KJ). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee of the Second Hospital of Jilin University (2016-101).