
Abstract
Background:
Quadriceps weakness is a common barrier to effective rehabilitation after anterior cruciate ligament (ACL) surgery. Neuromuscular electrical stimulation (NMES)—the application of electrical currents to induce muscle contraction—has been used as part of the postoperative rehabilitation regimen.
Purpose:
To investigate the effects of NMES on the recovery of quadriceps strength and knee function after ACL surgery.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
A search was conducted in the Web of Science, Embase, Cochrane Library, and PubMed databases between inception and August 2023 according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Included were randomized controlled trials of patients undergoing NMES as postoperative rehabilitation after ACL reconstruction or repair, with standard physical therapy as the control intervention. The quality of the included studies was assessed according to the Cochrane Collaboration risk-of-bias tool. Lower limb function was assessed qualitatively, and standardized mean differences (SMDs) in muscle strength and Lysholm scores were analyzed quantitatively and pooled using a random-effects model.
Results:
Eleven studies (N = 202 patients) met our inclusion criteria. The meta-analysis of muscle strength values, which included 9 studies, showed that patients who underwent physical rehabilitation with adjunctive NMES had better recovery and improvement in quadriceps muscle strength compared with standard physical therapy at both short- and long-term follow-ups (≤6 weeks: SMD, 0.53 [95% CI, 0.27-0.79] vs >6 weeks: SMD, 0.59 [95% CI, 0.18-0.99]; p < 0.001). Moreover, subgroup analyses showed that earlier physical rehabilitation with the assistance of NMES resulted in better muscle strength recovery (≤1 week: SMD, 1.48 [95% CI, 0.80-2.17] vs >1 week: SMD, 0.44 [95% CI, 0.21-0.67]; p < 0.001). The meta-analysis of Lysholm scores, which included 3 studies, did not indicate any significant differences between the assisted NMES and control groups.
Conclusion:
Our study demonstrated that in both short- and long-term follow-up studies, postoperative rehabilitation with NMES after ACL surgery significantly increased quadriceps muscle strength compared with standard rehabilitation alone.
Keywords
Anterior cruciate ligament (ACL) injuries are a common knee injury, with an annual incidence of 78 cases per 100,000 inhabitants worldwide4,8,13,24,31 and approximately 25,000 injuries per year in the United States. 24 The incidence of ACL reconstruction (ACLR) has been widely reported as varying between 30 and 74 procedures per 105 person-years, but the numbers have been rising. 19 With advances in basic research, surgical equipment, and surgical techniques, ACLR is becoming the most common treatment for patients with ACL injuries. 28 Nonetheless, quadriceps weakness is a common barrier to effective rehabilitation after ACL injury and reconstruction. 2 It can lead to many serious consequences—including gait abnormalities, 17 quadriceps atrophy, 18 persistent knee pain, and early osteoarthritis.24,25 A systematic review showed that only 65% of people regained their preinjury level of exercise after ACL surgery while 55% regained their competitive level of exercise. 3 Failure of quadriceps activation leads to a reduced ability to actively contract the muscle and is thought to be the source of persistent muscle weakness after ACLR. The simultaneous occurrence of quadriceps activation failure in the reconstructed limb and the contralateral limb has also been reported. 32 This is attributed to arthrogenic muscle inhibition—a process in which failure of quadriceps activation is caused by neural inhibition. Although the exact mechanism of quadriceps weakness is unknown, there is evidence that quadriceps activation failure and muscle atrophy can lead to persistent strength deficits.21,35
Neuromuscular electrical stimulation (NMES) is the application of electrical currents to induce muscle contraction and help build muscle strength. In recent years, there has been an increase in the number of studies regarding the use of NMES in orthopaedic and neurological rehabilitation.9,23,27,33,36 NMES can directly depolarize motor axons, leading to involuntary contraction. 36 Therefore, it may be an effective therapy to overcome the failure of quadriceps activation. Several randomized controlled trials (RCTs) have shown that NMES combined with functional exercise restores quadriceps muscle strength and improves physical function more than functional exercise alone,6,10,16,20 and a previous meta-analysis indicated the same results. 11 However, some studies have questioned these results.10,22,30 The results of long-term follow-ups on strength after ACL surgery are inconclusive.
This systematic review and meta-analysis aimed to investigate the effect of NMES on the recovery of quadriceps strength and knee function after ACL surgery (reconstruction or repair). We hypothesized that postoperative rehabilitation with NMES after ACL surgery would significantly increase quadriceps muscle strength and improve lower limb function.
Methods
Data Sources and Search Strategy
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Relevant literature on NMES-assisted post-ACL rehabilitation training was searched from the Web of Science, Embase, Cochrane Library, and PubMed databases up to August 2023 using Medical Subject Headings terms, free text terms, and indexed word lists. There were no restrictions on the time of publication. The search strategy can be found in Appendix Table A1.
Inclusion and Exclusion Criteria
We included studies that met the following study criteria: (1) RCTs; (2) NMES as an adjunct to standard physical therapy and as the primary intervention; (3) a control group receiving standard physical therapy without any adjunctive treatment with NMES intervention; (4) all study patients having undergone ACLR or repair; (5) the study population of adults and adolescents (age ≥13 years); (6) quadriceps or hamstring strength measured by isometric or isokinetic tests; and (7) studies published in English. Studies were excluded if (1) they were quasi-experimental or observational, (2) if NMES was not the primary intervention, and (3) if the study involved animal or cadaveric testing.
Screening
Two independent authors (Z.L. and Z.C.) screened the titles and abstracts of the combined search results and selected the qualified studies after removing duplicates. Subsequently, a full review of the qualified studies was then conducted according to the selection criteria. Any disagreements were resolved by discussion between the review authors or by consultation with a third author (J.D.).
Data Abstraction
All information was extracted by the first author (Z.L.) according to a predesigned data extraction form. The main data extracted were the intervention parameters of NMES, basic characteristics of the study population, the mean and standard deviation of strength before and after the intervention for quadriceps or hamstrings, and data related to knee function. If important data in the article were unclear or not reported, attempts were made to contact the corresponding author for access.
Quality Assessment
The risk of bias for the studies included in this meta-analysis was assessed according to the Cochrane Collaboration risk-of-bias tool. 12 This tool includes the following 7 components: random sequence generation, allocation concealment, patient and personnel blinding, incomplete outcome data, selective reporting, blinding of outcome assessment, and other biases. Each component is evaluated as low risk, unclear risk, or high risk of bias.
Data Analysis
A meta-analysis was performed when ≥3 studies with the same results were identified. A random-effects model of the DerSimonian and Laird method, which considers variations within and between studies, was used. Forest plots were developed to visualize individual study summaries and pooled estimates. Standardized mean differences (SMDs) are a valid measure of variability across studies measuring the same outcome. The SMDs represented differences in postintervention measures that were standardized as a percentage of the mean of the uninvolved lower limb. If the study authors did not standardize these methods to the uninvolved limb, we standardized them by dividing by the mean score of the uninvolved limb in the same group or by dividing the mean score of the uninvolved limb in the control group only by (if NMES was used in both) the limb intervention group. The Cochran Q statistic and the I2 value were used to study heterogeneity between studies, where an I2 of ≥50% represents a medium to high degree of heterogeneity and requires heterogeneity analysis. A simple sensitivity analysis was performed by removing each study and replacing the overall pooled estimates from each model examined to identify potentially influential studies. The Cohen d was calculated for each original study and was the overall estimator, and a 2-sided P < .05 was considered statistically significant.
When the quantitative analysis was not performed, a qualitative synthesis was provided for each outcome separately, describing potential reasons why some studies showed effective effects and others did not by looking for differences in populations, intervention protocols, control groups, and adherence.
Results
A total of 1046 studies were retrieved from the databases, with 966 studies remaining after removing 80 duplicates. After reviewing the titles and abstracts, a further 946 studies were excluded. The remaining 20 studies were reviewed in full, and 9 studies were excluded for not being RCTs, not having a control group receiving standard physical therapy, and/or not reporting relevant outcomes. A total of 11 studies ‡ met the inclusion criteria, of which 9 studies5-7,16,22,26,29,30,34 were included in the meta-analysis on quadriceps muscle strength and 3 studies6,10,20 were included in the meta-analysis on Lysholm scoring. The study selection process is shown in Figure 1.
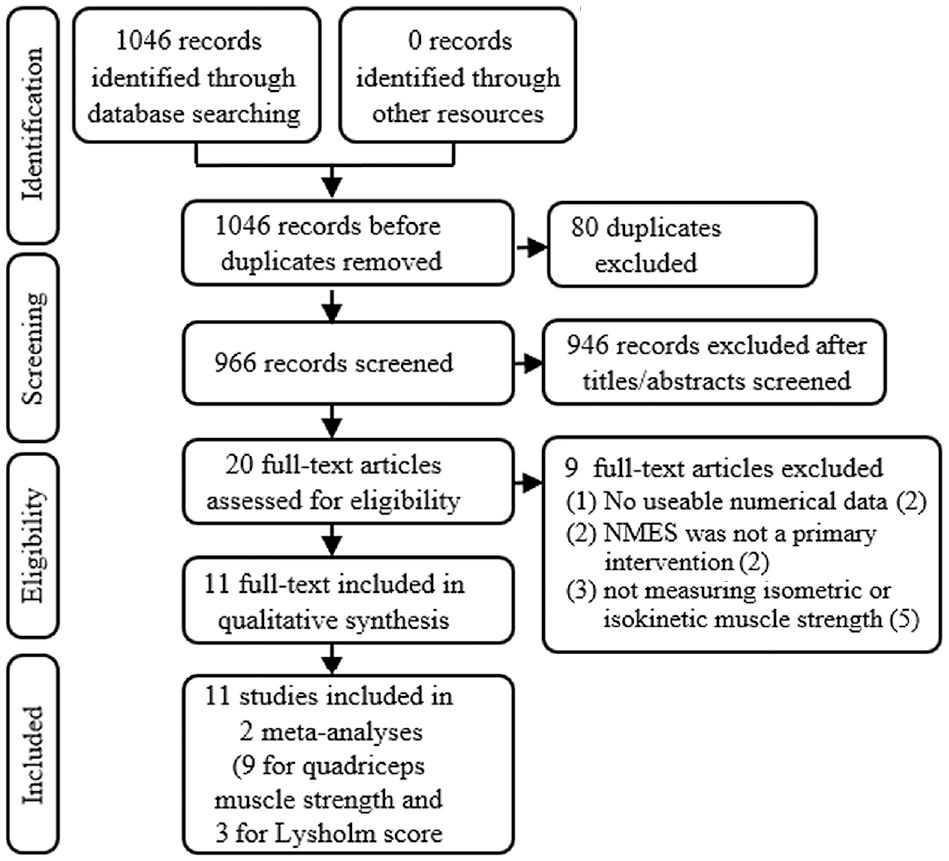
The PRISMA flow chart of the study inclusion process. NMES, neuromuscular electrical stimulation; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Characteristics and Quality Assessment
The characteristics of the included studies are shown in Table 1. Overall, 202 patients were in the intervention group and 200 in the control group, all of whom had undergone ACLR or ACLR/repair as in the study by Paternostro-Sluga et al. 22 Patients from both sexes were included in most studies, except the study by Taradaj et al, 29 who included only male athletes, and Labanca et al, 16 Delitto et al, 5 Feil et al, 6 and Ogrodzka-Ciechanowicz et al, 20 who did not specify patient sex. Isometric or isokinetic strength was the primary outcome, while Ogrodzka-Ciechanowicz et al 20 reported physical function-related scores.
Characteristics of the Included Studies a

All patients underwent ACLR, except for those in the study of Paternostro-Sluga et al, 22 who underwent either ACLR or repair. ACLR, anterior cruciate ligament reconstruction; C, control group; ext, extension; F, female; flex, flexion; HiToP, HighTone Power Therapy; KOOS-ADL, Knee injury and Osteoarthritis Outcome Score–Activities of Daily Living; KOS-ADLS, Knee Outcome Survey–Activities of Daily Living Scale; M, male; NMES, neuromuscular electrical stimulation; NR, not reported; PS, Polystim device; postop, postoperative; standard, standard rehabilitation; STSTS, sit-to-stand-to-sit; T, treatment group; VAS, visual analog scale.
The risk-of-bias scores for the included studies are presented in Figure 2. Most studies had a low risk of bias in most categories. Areas with a high risk of bias were mainly in allocation concealment, blinding of participants, and blinding of outcome assessment.

The Cochrane risk-of-bias assessment results (A) for each study and (B) summarized across all studies.
Muscle Strength Measurements and Outcome Scores of the Included Studies
All included studies, except Ogrodzka-Ciechanowicz et al, 20 provided a method for standardizing the intervention and control groups to the original values of the uninvolved limb or the mean of both limbs (Table 2). Table 3 presents the details of the parameters used in the interventions. The on-time percentage and total on-time in minutes for the entire intervention and weekly were calculated from the ratio of on-time to off-time. The intensity (measured in mA) of the current used for stimulation was mostly reported as a qualitative perception of the maximum “tolerable” or “comfortable” intensity with a minimum requirement of achieving muscle contraction.
Muscle Strength Measurement of Hamstrings (Flexion) and Quadriceps (Extension) a
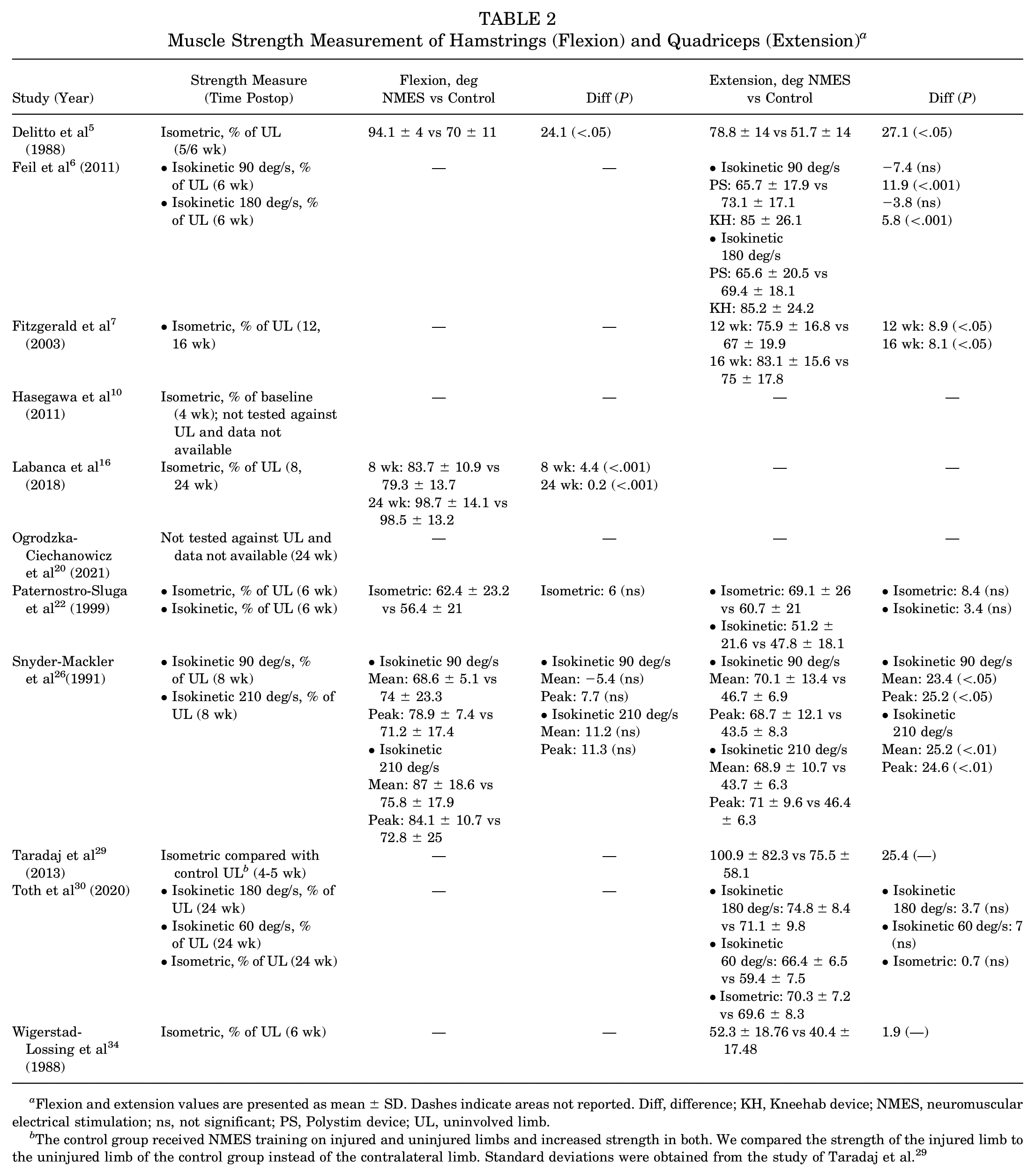
Flexion and extension values are presented as mean ± SD. Dashes indicate areas not reported. Diff, difference; KH, Kneehab device; NMES, neuromuscular electrical stimulation; ns, not significant; PS, Polystim device; UL, uninvolved limb.
The control group received NMES training on injured and uninjured limbs and increased strength in both. We compared the strength of the injured limb to the uninjured limb of the control group instead of the contralateral limb. Standard deviations were obtained from the study of Taradaj et al. 29
Parameters of NMES Used by Included Studies a

KH, Kneehab device; Max, maximum; NMES, neuromuscular electrical stimulation; NR, not reported; PS, Polystim device.
Pulse width was obtained from the study of Taradaj et al 29 by email contact.
A total of 6 patient- and clinician-reported outcome measures—International Knee Documentation Committee (IKDC),6,30 Lysholm,6,10,20 cross-sectional area,30,34 Knee injury and Osteoarthritis Outcome Score–Activities of Daily Living (KOOS-ADL), 30 Knee Outcome Survey–Activities of Daily Living Scale (KOS-ADLS), 7 and visual analog scale for pain 7 —in 6 studies6,7,10,20,30,34 were used to assess the impact of NMES on the recovery of knee function after ACL surgery (Table 4).
Patient- and Clinician-Reported Outcome Measures a

Data are presented as mean ± SD unless otherwise indicated. CSA, cross-sectional area; Diff, difference; KH, Kneehab device; IKDC, International Knee Documentation Committee; KOOS-ADL, Knee injury and Osteoarthritis Outcome Score–Activities of Daily Living; KOS-ADLS, Knee Outcome Survey–Activities of Daily Living Scale; NMES, neuromuscular electrical stimulation; ns, not significant; Post, Postoperative; Preop, preoperative; PS, Polystim device; VAS, visual analog scale.
Meta-Analyses of Clinical Outcome Measures
Muscle Strength
Quantitative summaries of the 9 included studies showed significant improvements in strength in the involved limb compared with the unaffected limb. The results of the studies5-7,16,22,26,29,30,34 included in the meta-analysis were consistent, with estimates ranging from an SMD of 0.35 (95% CI, −0.34 to 1.03) to an SMD of 1.92 (95% CI, 0.28 to 3.57) across studies. No heterogeneity was observed between the studies (I2 = 0% [<50%] and P = .49 [>0.91] for the Q test); thus, the fixed-effects model was used for the meta-analysis. The results of the sensitivity analysis indicated that none of the 9 studies caused significant interference with the results of the meta-analysis, implying good stability. The SMD pooled across the 9 studies was 0.55 (95% CI, 0.33-0.76) and was statistically significant (Z = 4.92; P < .001), indicating that NMES was effective in enhancing quadriceps strength. Details are shown in Figure 3.

Forest plot of studies included in meta-analysis of quadriceps strength measurement. Std., standardized; IV, inverse variance.
Moderator Effect of Intervention Onset Time on Muscle Strength
Previous literature has examined several covariates as potential modifiers of the relationship between NMES and strength outcomes.6,10,26,34 Of these modifiers, intervention onset time was identified as a significant moderator of the relationship between NMES and strength increase. Three studies5,26,30 with an intervention time of ≤1 week were included in a subgroup analysis, which was rerun for the modifier of intervention onset time (≤1 vs >1 week) (Figure 4). The analysis showed that NMES enhanced muscle strength recovery in the quadriceps regardless of whether the intervention started at a time of ≤1 week (SMD, 0.55 [95% CI, 0.33-0.76]), but the pooling of the 3 studies,5,26,30 with an intervention time of ≤1 week, indicated a better effect of NMES on muscle strength recovery (≤1 week: SMD, 1.48 [95% CI, 0.80-2.17] vs >1 week: SMD, 0.44 [95% CI, 0.21-0.67]; p < 0.001).

Forest plot of studies included in the meta-analysis of intervention onset time (≤1 week vs >1 week) to evaluate quadriceps strength. Std., standardized; IV, inverse variance.
Subgroup Analysis by Follow-up Times
A meta-analysis of the standard rehabilitation time of 6 weeks has been performed in a previous study, 11 but no review has analyzed long-term follow-up studies on the recovery of muscle strength after ACL surgery in NMES. We used the standard rehabilitation time of 6 weeks as a cutoff and performed a subgroup analysis for the intervention factor of the follow-up time (Figure 5). Analysis showed that muscle strength recovery was better after NMES intervention compared with standard physical therapy at both short-(≤6-week) and long-term (>6-week) follow-ups (≤6 weeks: SMD, 0.53 [95% CI, 0.27-0.79] vs >6 weeks: SMD, 0.59 [95% CI, 0.18-0.99]; p < 0.001).

Forest plot of studies included in the meta-analysis of quadriceps strength measurement stratified by the follow-up time (≤6 weeks vs >6 weeks). Std., standardized; IV, inverse variance.
Lysholm Scores
The results of the meta-analysis of Lysholm scores in the 3 included studies6,10,20 are shown in Figure 6. The mean difference in Lysholm scores was not statistically significant, and the I2 was 55%, indicating a medium to high degree of heterogeneity.

Forest plot of studies included in the meta-analysis of Lysholm scores. NMES, neuromuscular electrical stimulation. Std., standardized; IV, inverse variance.
Discussion
The major findings of this study demonstrated that in short-term (≤6 weeks) or long-term (>6 weeks) follow-up, postoperative rehabilitation with NMES after ACL surgery significantly increased quadriceps muscle strength and improved lower limb function compared with standard rehabilitation alone. A total of 11 studies § were included in this systematic review, of which 9 studies5-7,16,22,26,29,30,34 were included in a meta-analysis to assess the effect of NMES on quadriceps strength recovery. For these 9 studies, we used the timing of NMES intervention initiation and postoperative follow-up time as entry points to further analyze the optimal timing of NMES-assisted intervention and the long-term outcomes after NMES-assisted treatment. We chose the 2 commonly used time frames of whether NMES was combined with rehabilitation within 1 week of ligament surgery and whether postoperative follow-up was >6 weeks, and a sufficient number of studies were analyzed for evaluation. In addition, 3 studies6,10,20 reported on postoperative Lysholm scores and were therefore also analyzed in a pooled manner.
The results of the meta-analyses indicated that NMES combined with standard physical rehabilitation achieved better quadriceps strength recovery after ACL surgery compared with the control group that received standard physical rehabilitation only. The start time of NMES-assisted treatment varied in many previous studies, and we chose the usual cutoff of 1 week, with interventions ≤1 week being early interventions and >1 week being late interventions. The analysis of the pooled data (Figure 4) indicated that quadriceps muscle strength improved regardless of whether the start time of the intervention was ≤1 week, but the improvement was significantly better in the early interventions than in the late interventions (≤1 week: SMD, 1.48 [95% CI, 0.80-2.17]; >1 week: SMD, 0.44 [95% CI, 0.21-0.67]; p < 0.001). Other studies6,10 have reported similar findings. As to why quadriceps strength was significantly higher in the NMES group than in the control group, we suggest that earlier NMES-assisted therapy effectively reduces the atrophy of skeletal muscle fibroblasts 30 and that NMES-assisted therapy has a postoperative analgesic effect that promotes the early initiation of functional exercise in patients, both of which can significantly improve quadriceps strength.
In the pooled analysis of long-term postoperative follow-up results, we compared strength measurements at 6 weeks because of the generality of the included studies. As rehabilitation after ACL surgery usually lasts 6 to 12 months or even longer, the clinical significance of measuring strength at 6 weeks may be controversial. The results of our subgroup analysis according to follow-up times (Figure 5) showed that quadriceps muscle strength was stronger in the NMES-assisted group than in the physical therapy alone group after both short- and long-term follow-ups (≤6 weeks: SMD, 0.53 [95% CI, 0.27-0.79]; >6 weeks: SMD, 0.59 [95% CI, 0.18-0.99]; p < 0.001). While Toth et al 30 reported no significant improvement in isokinetic or isometric knee extensor moments after 6 months of follow-up with postoperative NMES-assisted therapy, there are several possible explanations for their findings. For example, the data from the follow-up patients may have been lost, the equipment may have been introduced at a different time, or the rehabilitation process may have been performed in different hospitals, making it impossible to accurately assess the strength differences between the 2 groups. In addition, the activity level before surgery was not considered in their study.
When we analyzed the postoperative Lysholm scores reported by 3 studies,6,10,20 we found that assisted NMES did not show a significant improvement in lower limb function after ACL surgery. Other outcome scores regarding lower limb function—such as the IKDC, KOOS-ADL, and KOS-ADLS—demonstrated some restorative effect of NMES-assisted treatment; nevertheless, the results were not statistically significant.
We conducted a statistical analysis of the cross-sectional area of the quadriceps muscle after ligament surgery using the results of 2 of the included studies30,34 as well as another study that was not an RCT. 15 The 2 studies15,34 that used computed tomography to assess the cross-sectional area of the muscle showed that adjuvant NMES treatment was able to increase the muscle area of the quadriceps, regardless of the follow-up length. When the entry point is at the cellular level, for quadriceps muscle fibers, adjunctive NMES rehabilitation reduces atrophy and better preserves the contractility of skeletal muscle fibers. 15 Studies1,10,14 have also used ultrasound techniques to assess skeletal muscle thickness and evaluate volume to estimate muscle size and the degree of muscle atrophy, showing that the experimental group with NMES participation had a lower decrease in muscle thickness than the control group and similarly weaker muscle atrophy than the control group. The results of these studies may also explain why a more significant recovery of quadriceps strength was achieved after early intervention with NMES and further suggest the need for early NMES-assisted rehabilitation training.
Limitations
This review and meta-analysis has some limitations. When a study had multiple intervention groups, we selected data from only 1 of the intervention groups to include in the data analysis. When we screened the literature for inclusion, we did not restrict the publication date of the articles, which resulted in including several studies5,26,34 that were published earlier in the meta-analysis and, as the literature was screened up to August 2023, there may have been some more recent and relevant literature that was not included in the meta-analysis. In addition, there was some heterogeneity in the quality assessment of some studies however, this may be due to the fact that some of the studies on quality assessment were not explicit in the original study, and we were not able to contact the original authors, leading to possible inaccuracies in the assessment of study quality when we used the Cochrane risk-of-bias tool. In addition, many other factors can influence the outcome of rehabilitation, such as the fact that patients have different levels of compliance and that rehabilitation protocols are not entirely consistent. Other effective rehabilitation protocols should be further explored in future studies.
Conclusion
Our study demonstrated that in both short- and long-term follow-up studies, postoperative rehabilitation with NMES after ACL surgery significantly increased quadriceps muscle strength compared with standard rehabilitation alone.
Footnotes
Appendix
Search Strategies Used According to Database a

| Search Strategy: PubMed |
| (“anterior cruciate ligament reconstruction”[MeSH Terms] OR “anterior cruciate ligamentreconstruction”[tiab] OR “Anterior Cruciate Ligament/surgery”[Mesh] OR “Anterior Cruciate Ligament surgery”[tiab] OR (ACL[tiab] AND “reconstructive surgical procedures”[MeSH Terms])OR “ACL reconstruction”[tiab] OR “quadriceps muscle”[MeSH Terms] OR “quadriceps”[tiab]) AND (“electric stimulation”[MeSH Terms] OR Electric Stimulation Therapy[mesh] OR “neuro-muscular electrical stimulation”[tiab] OR NMES[tiab]) AND (randomized controlled trial[pt] OR controlled clinical trial[pt] OR randomized[tiab] OR randomised[tiab] OR randomization[tiab] OR randomisation[tiab] OR randomly[tiab] OR trial[tiab] OR groups[tiab] OR Clinical trial[pt] OR “clinical trial”[tiab] OR “clinical trials”[tiab] OR “evaluation studies”[Publication Type] OR “evaluation studies as topic”[MeSH Terms] OR “evaluation study”[tiab] OR evaluation studies[tiab] OR “intervention study”[tiab] OR “intervention studies”[tiab] OR “case–control studies”[MeSH Terms]OR “case–control”[tiab] OR “cohort studies”[MeSH Terms] OR cohort[tiab] OR “longitudinal studies”[MeSH Terms] OR “longitudinal”[tiab] OR longitudinally[tiab] OR “prospective”[tiab]OR prospectively[tiab] OR “retrospective studies”[MeSH Terms] OR “retrospective”[tiab] OR “follow up”[tiab] OR “comparative study”[Publication Type] OR “comparative study”[tiab]) NOT(Editorial[ptyp] OR Letter[ptyp] OR Case Reports[ptyp] OR Comment[ptyp]) NOT (animals[mh]NOT humans[mh]) |
| Search Strategy: Web of Science |
| ((TS=(Anterior Cruciate Ligament Reconstruction) OR AB=(anterior cruciate ligament reconstruction OR Anterior Cruciate Ligament surgery OR ACL reconstruction)) AND (TS=(Quadriceps Muscle) OR AB=(Quadriceps Muscle OR Muscle, Quadriceps OR Muscles, Quadriceps OR Quadriceps Muscles OR Quadriceps Femoris OR Vastus Medialis OR Vastus Intermedius OR Rectus Femoris))) AND (TS=(Electric Stimulation) OR AB=(Electric Stimulation OR Electrical Stimulation OR Electrical Stimulations OR Stimulation, Electrical OR Stimulations, Electrical OR Stimulation, Electric OR Electric Stimulations OR Stimulations, Electric OR Electric Stimulation Therapy OR neuromuscular electrical stimulation OR NMES)) |
| Search Strategy: Cochrane |
#1 MeSH descriptor: [Anterior Cruciate Ligament] explode all trees [793 hits] #2 (Cruciate Ligaments, Anterior; or Ligaments, Anterior Cruciate; or Cruciate Ligament, Anterior; or Anterior Cruciate Ligaments; or Ligament, Anterior Cruciate; or Cranial Cruciate Ligaments; or Cruciate Ligaments, Cranial; or Cruciate Ligament, Cranial; or Ligament, Cranial Cruciate; or Anterior Cranial Cruciate Ligament; or Ligaments, Cranial Cruciate; or Cranial Cruciate Ligament):ti,ab,kw (Word variations have been searched) [3385 hits] #3 #1 or #2 [3385 hits] #4 MeSH descriptor: [Electric Stimulation] explode all trees [2298 hits] #5 (Electrical Stimulation; or Stimulations, Electrical; or Electrical Stimulations; or Stimulations, Electric; or Electric Stimulations; or Stimulation, Electrical; or Stimulation, Electric; or NMES):ti,ab,kw (word variations were searched) [15,938 hits] #6 MeSH descriptor: [Quadriceps Muscle] explode all trees [1116 hits] #7 (Quadriceps Muscle or Vastus Intermedius or Vastus Lateralis or Rectus Femoris or Quadriceps Femoris or Muscles, Quadriceps or Quadriceps Muscles or Muscle, Quadriceps or Vastus Medialis):ti,ab,kw (word variations were searched) [7528 hits] #8 #6 or #7 [7528 hits] #9 #4 or #5 [16,073 hits] #10 #3 and #8 and #9 [57 hits] |
| Search Strategy: Embase |
#1 anterior AND cruciate AND (‘ligament’/exp OR ligament) AND (‘reconstruction’/exp OR reconstruction) [22,395 hits] #2 ((anterior AND cruciate AND ligament AND reconstruction OR anterior) AND cruciate AND ligament AND surgery OR acl) AND reconstruction [21,591 hits] #3 quadriceps AND muscle [27,972 hits] #4 (((((((quadriceps AND muscle OR muscle,) AND quadriceps OR muscles,) AND quadriceps OR quadriceps) AND muscles OR quadriceps) AND femoris OR vastus) AND medialis OR vastus) AND intermedius OR rectus) AND femoris [7356 hits) #5 electric AND stimulation [32,440 hits] #6 (((((((((electric AND stimulation OR electrical) AND stimulation OR electrical) AND stimulations OR stimulation,) AND electrical OR stimulations,) AND electrical OR stimulation,) AND electric OR electric) AND stimulations OR stimulations,) AND electric OR electric) AND stimulation AND therapy OR neuromuscular) AND electrical AND stimulation OR nmes [10,454 hits] #7 #1 OR #2 [22,677 hits] #8 #3 OR #4 [33,180 hits] #9 #5 OR #6 [38,927 hits] #10 #7 AND #8 AND #9 [46 hits] |
NMES, neuromuscular electrical stimulation.
Acknowledgements
The authors thank the PubMed, Web of Science, Cochrane and Embase databases for sharing data.
Final revision submitted February 6, 2024; accepted February 26, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.