
Abstract
Background:
Acromioclavicular joint (ACJ) disruption occurs frequently in athletes engaged in contact sports. However, the current understanding of ACJ biomechanics during muscle-driven functional activities and the influence of different treatment approaches (eg, reconstruction surgery vs nonoperative methods) on ACJ kinematics and stability remains limited. The absence of precise in vivo biomechanical measurement modalities for scapular and clavicular kinematics contributes significantly to this lack of understanding.
Purposes/Hypothesis:
The purposes of this study were to determine whether dynamic stereo x-ray (DSX) imaging can be used to evaluate the in vivo kinematics of the ACJ and to provide preliminary comparative data on ACJ kinematics, range of motion, and isometric strength of surgically reconstructed or nonoperatively treated ACJ shoulders and their uninjured contralateral shoulders. It was hypothesized that ACJ kinematics could be measured successfully using DSX and that surgically and nonoperatively treated shoulders would show abnormal 3-dimensional (3-D) ACJ kinematics compared with the uninjured contralateral.
Study Design:
Controlled laboratory study.
Methods:
In this cross-sectional study, 11 participants who had undergone unilateral ACJ reconstruction surgery and 3 patients who received nonoperative treatment were enrolled. ACJ kinematics were assessed during active forward flexion, scaption, and abduction through high-speed DSX imaging, complemented by 3-D bone models obtained via computed tomography (CT) scans. To gauge kinematic differences, a 1-dimensional statistical parametric mapping method was employed, which compared outcomes in the index limb to those in the uninjured counterpart. In addition, the range of motion and isometric strength at various abduction angles were analyzed, employing a repeated-measures analysis of variance to compare the affected and uninjured sides.
Results:
Leveraging a combination of DSX imaging and patient-specific CT bone models, ACJ kinematics was measured successfully during movements along anatomic planes. Preliminary findings from this investigation revealed no detectable differences between the surgically reconstructed and uninjured sides in ACJ biomechanics, shoulder range of motion, and isometric strength outcomes. However, on average, the nonoperatively treated shoulders demonstrated increased internal rotation, upward rotation, and posterior tilting of the scapula relative to the clavicle (no statistical analyses were performed due to the small sample size).
Conclusion:
DSX imaging is a promising tool for evaluating potential in vivo kinematic abnormalities in the ACJ during muscle-driven activities, laying the groundwork for further investigations in both ACJ-reconstructed and nonreconstructed patients. This study furnished essential data for conducting power analyses and designing future studies with an adequate sample size to investigate the impact of different treatment approaches on shoulder girdle mechanics.
Clinical Relevance:
With its potential for accurately characterizing shoulder girdle kinematics post-ACJ injury, DSX imaging can offer valuable insights for future clinical studies, facilitating informed decisions regarding the short- and long-term impacts of treatment choices on shoulder health and function.
Keywords
Acromioclavicular joint (ACJ) injury is a common shoulder injury in young contact-sports athletes. This joint is a synovial diarthrodial articulation linking the medial acromion and distal clavicle, 18 facilitating gliding and rotational motions while coupling scapular and clavicular movements during arm elevation.24,33 The ACJ is kept stable by passive (acromioclavicular and coracoclavicular ligaments and joint capsules) and active (trapezius and deltoid muscles) structures. The joint can be injured by direct high-energy trauma or falling with an adducted arm. The ACJ injury accounts for up to 10% of all shoulder injuries 7 and a half of all shoulder girdle injuries in contact athletes (primarily young male athletes in their 20s).4,11-13,15,16,17,18,32 In addition to disrupting ACJ-dependent motion, this injury could compromise the function of the entire shoulder complex by altering the scapular and glenohumeral joint mechanics, which could undermine its long-term health and function.
Per Rockwood classification conservative treatment for types I and II and surgical treatment for types IV-VI are typically suggested,5,25 treatment for type 3 remains controversial.5,6,19,23 However, surgical reconstruction is often indicated in persons with significant instability or failed conservative treatments. The treatment goal after ACJ injury is the restoration of physiological joint biomechanics, range of motion, and mechanical stability. 21 Traditionally, surgical reconstruction of the ACJ was performed using rigid nonanatomic fixations such as Kirschner-wire or hook-plate, which resulted in high rates of complications and failure. Modern anatomic suspensory fixations are emerging to address the shortcomings of the older methods to improve surgical success and patient outcomes. However, there needs to be more evidence regarding the effectiveness of anatomic surgical techniques in restoring ACJ biomechanics and shoulder function in living patients during muscle-driven activities.
The primary challenge in obtaining such evidence is that ACJ biomechanics is difficult to measure using standard biomechanical measurement techniques (eg, motion capture camera system). In the past 2 decades, dynamic stereo x-ray (DSX) imaging combined with patient-specific 3-dimensional (3-D) bone models paved the way for measuring intricate joint biomotion with submillimeter and subdegree accuracy. This system has been validated and used to study shoulder biomechanics of rotator cuff pathology or after shoulder arthroplasty. 1,2,8,23,31 However, there is a paucity of research using DSX imaging to evaluate the kinematics of the ACJ in healthy persons and those who have undergone surgical treatment.
The main objective of our study was to investigate the feasibility of DSX imaging for evaluating the in vivo kinematics of the ACJ. Second, this study aimed to provide preliminary data on ACJ kinematics, range of motion, and isometric strength of surgically reconstructed or nonoperatively treated ACJ shoulders and uninjured contralateral shoulders. It was hypothesized that ACJ kinematics would be measured successfully using DSX, and the surgically and nonoperatively treated shoulders would demonstrate abnormal 3-D ACJ kinematics compared with the uninjured contralateral.
Methods
Patient Selection
The patient recruitment process, detailed in Figure 1, spanned several stages, beginning with initial screening and culminating in the final enrollment in the study. For eligibility, patients of both sexes, aged 18 to 60 years, within 1 to 3 years posttreatment with an acute unilateral ACJ disruption (classified as types 3-5 due to traumatic injuries) were identified. Candidates met the following inclusion criteria: no previous history of shoulder issues or bilateral injuries and no neuromusculoskeletal conditions impacting shoulder function. Exclusions were made for lactating/pregnant women, severe obesity (body mass index [BMI] >35 kg/m2), contralateral shoulder injury history, upper extremity fractures, scapulothoracic dislocations, rotator cuff tears, or documented cervical spine pathologies. These criteria were evaluated via clinical notes and participant-reported information during screening.

Flowchart of patient recruitment process.
Initially, 81 patients were screened, resulting in 55 meeting the inclusion criteria. Eventually, 18 patients consented to join the study. However, 2 patients missed their computed tomography (CT) scan appointments, and 2 had suboptimal DSX imaging quality, leading to their exclusion. Consequently, the statistical analyses included outcomes from 11 surgically treated and 3 nonoperatively treated patients.
Range of Motion, Isometric Strength, and Self-reported Outcomes
To detect any range of motion deficits, a goniometer was used during the study visit to measure the active range of motion in both shoulders 3 times each for the following 4 motions: forward flexion, external rotation at 0° of abduction, internal rotation at 90° of abduction, and external rotation at 90° of abduction. A handheld dynamometer (MicroFET Wireless, Hoggan Scientific LLC) was used to measure the participant's maximum isometric load in different anatomic directions to assess potential strength deficits. Each measurement was performed 3 times, with the participants maintaining a 90° flexed elbow. They were instructed to exert maximal force while pressing against the dynamometer. The current study strictly followed the measurement protocols prescribed by the manufacturer to ensure accuracy and consistency. The patient underwent 6 measurements, initially while in the supine position for activities 1 to 4, followed by a transition to the seated position for activities 5 and 6:
Internal rotation at 0° of abduction: the dynamometer transducer was positioned on the posterior surface of the upper arm, proximal to the wrist.
External rotation at 0° of abduction: the transducer was placed on the anterior surface of the upper arm, proximal to the wrist.
Internal rotation at 90° of abduction: the patient remained in a supine position, and the transducer was located on the posterior surface of the upper arm, proximal to the wrist.
External rotation at 90° of abduction: the transducer was situated on the posterior surface of the upper arm, proximal to the wrist.
Abduction starting from 0°: the transducer was placed on the lateral surface of the upper arm, proximal to the elbow.
Abduction starting at 90°: the transducer was positioned on the lateral surface of the upper arm, proximal to the elbow.
High-resolution CT
A high-resolution 3-D shoulder CT scan (0.6 × 0.6 × 0.6 mm voxels; Cannon, Aquilion One 640, Dual-Energy CT Scanner) was acquired bilaterally for each patient. This detailed scan included the clavicle and the superior aspect of the shoulder complex down to the distal humeral condyles. Using these CT scans, the patient-specific 3-D bone models of the clavicle, scapula, and humerus were created in Mimics (Materialize) and were then used during the registration process. The bone models were also used to identify the anatomic coordinate systems (according to International Society of Biomechanics [ISB] standards) and digitize ACJ insertion points, as detailed in the following sections. 35
In Vivo Shoulder Kinematics Evaluation
DSX Imaging
The DSX system measured 3-D shoulder kinematics at 20 Hz with a maximum voltage of 85 kVp, 125 mA current, and 2-ms pulse width (Figure 2). The DSX system uses 2 x-ray sources (Figure 2), which capture high-speed x-ray videos from the shoulder from 2 calibrated, nonoverlapping view angles. The 3-D bone models of the clavicle, humerus, and scapula (acquired through CT) were aligned with both views simultaneously to estimate their pose in each frame, enabling calculations of joint kinematics. The source-to-detector distance was ~180 cm with an interbeam angle of ~30°; x-ray radiation parameters were adjusted for minimum exposure parameters to acquire optimal tissue and bone contrast for each patient.

DSX set up for shoulder imaging. (A) The participant is positioned in the field of view approximately where the 2 x-ray beams intersect. (B) 3-D bone models (acquired through CT) will be aligned simultaneously with both views in each frame. (C) Positions of humerus, scapula, and clavicle in each frame will be estimated to calculate shoulder kinematics. 3-D, 3-dimensional; CT, computed tomography; DSX, dynamic stereo x-ray.
Dynamic Activities
After determining the ideal radiation parameters and patient positioning, at least 3 practice trials per movement (without radiation) were conducted to ensure that patients understood the movements. Using the DSX system, 3 repetitions of the activities listed below were recorded, with the patients’ hand initially resting by their side: (1) abduction in the coronal plane, (2) abduction in the scapular plane (also known as scaption; ~30° anterior to coronal), and (3) forward flexion. The patients maintained a straight back during each activity to prevent compensatory leaning. They followed a metronome beat (70 beats per minute) for even and uniform movement, keeping their elbows extended and palms facing forward. A heavy-based upright round post was placed at arm's length from each patient to ensure consistent movement, with its position adjusted to accommodate each activity. The patients were instructed to move their palm behind and near the post, lightly brushing against it during each activity.
Postprocessing
3-D kinematics of the ACJ were calculated using established and rigorous methods with a validated accuracy of 0.5 mm of translation and 0.5° of rotation or better for shoulder kinematics.3,8 Briefly, the 3-D poses of the humerus, scapula, and clavicle were determined using DSX-Suite (C-Motion) by registering simultaneously the bone-model contours acquired through CT to the DSX images in both views in each frame, according to standardized procedures (Figure 2). 22 In addition, the anatomic coordinate system was determined for each bone, and ACJ kinematics were calculated in Visual-3D (C-Motion) and described using the Euler rotation sequence along superior-inferior-medial-lateral-anterior-posterior axes, respectively, per ISB standards. 35
The functional Euclidean ACJ distance was measured by calculating the instantaneous Euclidean distance between the centroid of the articulating surfaces of the distal clavicle and the acromion digitized directly from CT scans, as shown in Figure 3. This measurement was used to approximate ligament length changes during functional activities to better understand the kinematics of ACJ reduction.
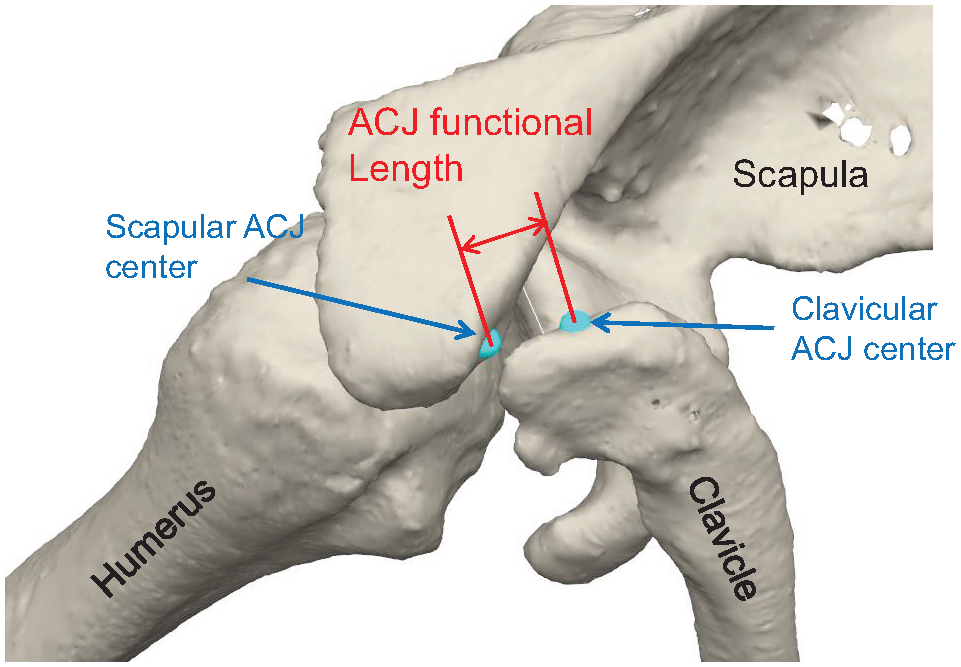
Functional ACJ distance (shown in red) is determined by calculating the instantaneous Euclidean distance between the acromial and clavicular insertions of the AJC (shown in blue). ACJ, acromioclavicular joint.
Statistical Analysis
Statistical analyses were conducted with an alpha level of .05 followed by a Bonferroni correction to prevent type 1 errors from multiple comparisons. The side-to-side differences of waveforms were compared using repeated-measures 1-dimensional statistical parametric mapping for the limb side (ACJ reconstructed vs uninjured contralateral). 28 The range of motion and isometric strength outcomes were compared using a repeated-measures analysis of variance between limb sides in the surgical group. Due to the small sample size, no statistical analyses were conducted between nonoperatively treated shoulders and their uninjured contralateral shoulders. However, for completeness, means and standard deviations of outcome measures were reported.
Results
Patients
Institutional review board approval was gained for our study (HSC-MS-20-0585). The demographic details and self-reported outcomes of study participants are shown in Table 1. A total of 11 patients (2 female; height, 179 ± 10.0 cm; body mass, 89 ± 19.2 kg; BMI, 27.7 ± 4.6 kg/m2; Rockwood types III and V; 24 ± 7 months postsurgery; coracoclavicular (CC) distance of 22.9 ± 4.0 mm at ~1 month before surgery; CC distance of 10.7 ± 4.9 mm ~3 months after surgery), with a unilateral ACJ injury consented and participated in our study. The CC distance was measured as the vertical distance from the clavicle's inferior cortex to the coracoid process's superior cortex on an anteroposterior radiograph. All participants were right-hand dominant. ACJ reconstructions were performed using suspensory anatomic fixation (details provided in Appendix Table A1). Briefly, 7 patients received reconstruction of CC ligaments alone (2 open and 5 arthroscopically assisted), whereas 4 patients received concomitant reconstruction of CC ligaments and AC joint capsule (1 open and 3 arthroscopically assisted). After the surgery, patients were required to wear a sling for 6 weeks. Range of motion exercises started afterward, followed by strengthening exercises 3 months later. In addition, 3 nonoperative patients (height, 179 ± 10 cm; body mass, 99.4 ± 13.6 kg; BMI, 30.9 ± 2.4 kg/m2; Rockwood Type III; 21 ± 9 months postinjury; radiographic pretreatment CC distance of 18.9 ± 1.7 mm) were included. The patients who received nonoperative treatment were given standard physiotherapy exercises after their injury. At their study visit, none of the surgical or nonoperative patients demonstrated scapular winging or other visible forms of scapular instabilities.
Patient Demographics a

AC, acromioclavicular; BMI, body mass index; CC, coracoclavicular; F, female; L, left; M, male; R, right.
Clinical Outcomes
No noticeable differences were detected in the range of motion and isometric strength between the surgically treated limbs and the uninjured contralateral limbs for each patient (Table 2). The mean side-to-side differences in the range of motion and strength were comparable between operatively and nonoperatively treated patients.
Range of Motion and Isometric Strength Assessments a

Data presented as mean ± SD unless otherwise indicated. The measurements were taken by following MicroFET's testing procedures. For activities 1 to 4, the dynamometer was placed on the wrist, while for activities 5 and 6, it was placed on the elbow.
P values for surgical group were calculated based on paired t test.
Statistical analysis was not performed due to small sample size.
Difference = Uninjured - Surgical.
ACJ Rotational Kinematics
ACJ rotational kinematics during the abduction, scaption, and forward flexion are shown in Figure 4. During concentric arm elevation from rest to the maximum point, the scapula (relative to the clavicle) rotated upward and internally while displaying increased posterior tilt. The pattern was, for the most part, symmetrically reversed (turned downward and outward) during the eccentric arm lowering. No statistical differences were detected between the shoulder that underwent surgery and the contralateral, uninjured shoulder.

Mean ± SD of the rotational kinematics of the ACJ (scapula with respect to clavicle) in surgical (n = 11), uninjured contralateral (n = 11), and conservatively treated (n = 3) shoulders during abduction, scaption, and forward flexion. ACJ, acromioclavicular joint.
The waveforms of the 3 nonoperative patients were included for completeness. It was observed that nonoperative shoulders, on average, demonstrated increased internal, upward, and posterior tilting rotations compared with operative shoulders. A summary is provided for the range of motion of the scapula relative to the clavicle for various movements and limb conditions in Table 3. The increased mean range of motion in all directions can be seen in the nonoperative group compared to surgical or uninjured shoulders in Table 3.
Scapular 3-D Rotations Relative to the Clavicle a

Data presented as mean ± SD. Abd, abduction; Flex, forward flexion; Scap, scaption; 3D, 3-dimensional.
ACJ Translational Kinematics
Functional ACJ distances are shown in Figure 5 for surgical, contralateral, and conservatively treated AC joints during the abduction, scaption, and flexion activities. Across all activities, on average, the ACJ distance was smaller in surgically treated compared to uninjured shoulders (see means in Table 4), but this difference was not statistically significant. However, the surgically treated and the contralateral uninjured shoulders maintained similar ACJ distances throughout the range of motion during all activities, suggesting overall successful reduction maintenance during dynamic activities (see ranges in Table 4).

Mean ± SD of functional ACJ distance for the surgical (n = 11), contralateral (n = 11), and nonoperatively treated (n = 3) shoulders during (A) abduction, (B) scaption, and (C) forward flexion. ACJ, acromioclavicular joint; 3-D, 3-dimensional.
Mean and Range of ACJ Euclidean Distance a
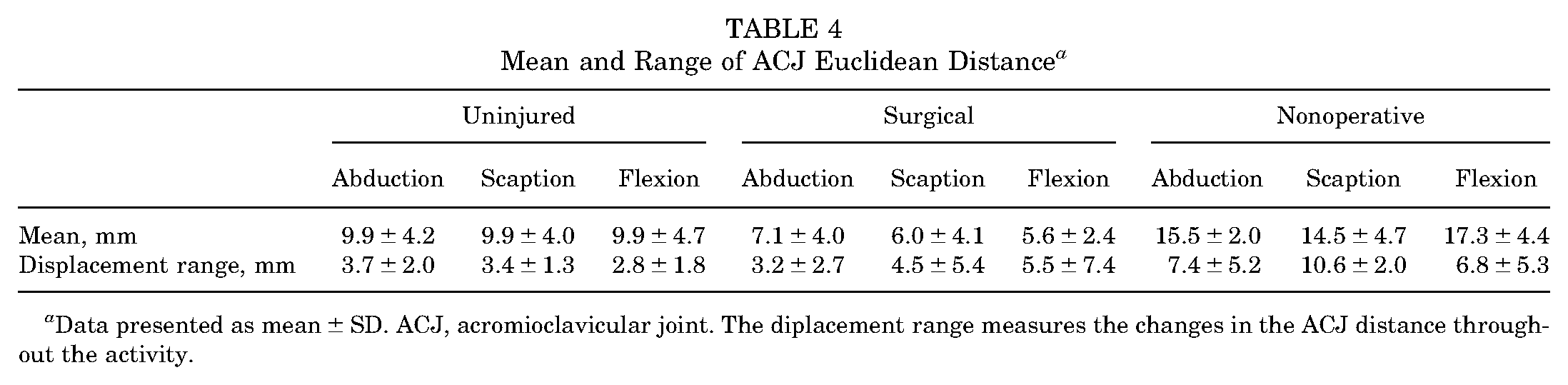
Data presented as mean ± SD. ACJ, acromioclavicular joint. The diplacement range measures the changes in the ACJ distance throughout the activity.
It was noted that nonoperative shoulders showed the most extensive ACJ functional distance on average for all movements. Specifically, the functional distance was the largest at small arm elevation angles (eg, 0%-20% and 80%-100% of the range of these movements), where ACJ ligaments are typically under maximum stress. In contrast to uninjured shoulders, the ACJ distance range in nonoperative shoulders fluctuated during arm elevation (see ranges in Table 4), indicating that the nonoperative joint's functional distance was not maintained uniformly during dynamic activities. Likewise, during forward flexion and scaption, the surgical group demonstrated a more extensive range than uninjured shoulders, albeit smaller than nonoperative shoulders.
Discussion
The finding from this study underscores the potential of DSX imaging as a valuable methodology for evaluating in vivo kinematics in the ACJ. This approach directly measures scapula and clavicle kinematics during muscle-driven activities through DSX imaging. Such an approach mitigates measurement errors introduced by skin motion artifacts - a common challenge encountered in conventional biomechanical assessments such as motion capture systems. By digitizing the insertion points of ACJ from patient-specific bone models acquired through CT, functional Euclidean ACJ distance was also approximated during different movements to probe dynamic translational instabilities of uninjured and treated ACJs. As such, DSX imaging could be a viable method for investigating the effects of ACJ treatment choices on shoulder girdle biomechanics.
The lack of accurate measurements has limited the understanding of the role of the ACJ in shoulder mechanics during muscle-driven functional activities. High-quality assessments of the scapular and clavicular coupling at the ACJ are restricted to a handful of in vivo clavicular biomechanics studies.10,14,24,26,27 Only a few of these studies focused specifically on changes to scapulothoracic kinematics following treatments (eg, hook-plate fixation), while still neglecting to report changes to the biomechanics of the ACJ itself.9,20 Otherwise, no relevant in vivo studies on modern anatomic ACJ treatments could be identified. Available studies have utilized static measurements (sequential MRI 29 or CT),20,30,31 invasive bone-pin markers that are unsuitable for large-scale clinical studies, 34 or skin-mounted markers or sensors that are inaccurate due to skin movement artifacts. 8 Specifically, these surface marker/sensor-based systems have significant measurement errors that typically exceed the ACJ range of motion, 33 limiting their ability to detect pathology- or treatment-related biomechanical differences. For example, based on measurements with bone pins, motion capture analysis consistently underestimated scapular rotations by 4° to 12°, even with modern cluster-based surface marker systems. 8 The DSX technique outlined in this article addresses these measurement error-related issues by directly measuring bone movements through biplane x-ray imaging.
The results of the uninjured contralateral shoulder align well with the available literature - for example, a study by Teece et al 33 examined the ACJ biomechanics during scaption for 30 healthy patients. An electromagnetic tracking system was used to track in vivo arm movement during elevation from a resting position to 90° of abduction, which represents 0% to 25% of the movement in the middle column of Figure 4. They reported 14.6° of upward rotation (current study, 17.2°), 4.3° of internal rotation (current study, 10.7°), and 6.7° of posterior tilt (current study, 4.2°) from rest to 90° of abduction. 33 As such, our study's results compare favorably with those of Teece et al, 33 while differences could be attributed to the measurement method, variations in the participants involved in the studies, discrepancies in the activities performed, and the generic definition of anatomic coordinate systems. In studies by Inman et al 14 and Conway, 10 an upward rotation of ~30° was reported during 2-dimensional measurements of forward flexion, which compares relatively well with the current result of 23.1°, considering that differences could be attributed to 2-dimensional static radiographic measurements versus the more accurate 3-D DSX imaging utilized in the current study. Overall, the present study offers distinctive insights into various movements that are absent for the most part in the available literature for cross-validation.
This study used DSX imaging to generate preliminary data on the effect of treatment choices (nonoperative and surgical) on ACJ kinematics, range of motion, isometric strength, and self-reported outcomes 13 to 32 months posttreatment.No side-to-side differences in ACJ kinematics (Figures 4 and 5; Tables 3 and 4), range of motion, and isometric strength (Table 2) at 13 to 30 months post-ACJ surgery were detected for these unilaterally affected operative patients. In contrast, the nonoperative group showed increased side-to-side differences for internal, upward, and posterior tilting rotations (Figure 4 and Table 3) and a more extensive range of functional ACJ distance (Figure 5 and Table 4). In summary, these initial findings motivate future studies to investigate the long-term potential for achieving optimal ACJ biomechanics, shoulder strength, and range of motion by comparing different treatment courses after ACJ injuries.
Limitations
It is crucial to consider the limitations of this study when interpreting the results. First, the sample size is an explicit limitation, as the surgeries and the subsequent patient recruitment and testing were negatively impacted by the restrictions during the COVID-19 pandemic. However, this study represents a preliminary exploration of the biomechanical assessments using DSX imaging to assess the role of treatment choices on shoulder girdle biomechanics. This imaging technique holds significant potential for future studies with larger sample sizes and more stratified subgroup analyses. As such, this work sets the stage for more extensive investigations that can provide valuable insights into the outcomes of ACJ treatment postinjury. Second, 2 female patients participated in this study, which compromised the ability to study sex-specific differences in ACJ biomechanics after treatments. However, ACJ injuries are considerably more frequent in male patients compared with female patients,15,16,32 and this limitation reflects the nature of ACJ injuries. Third, it is critical to acknowledge that, although all patients underwent modern anatomic suspensory fixation, differences in the implementation of the surgery were present based on patient-specific considerations and anatomy variations, which could not be controlled due to the retrospective study design and the heterogeneous ACJ reconstruction techniques. However, upon close examination, it was noted that the standard deviations of study outcomes between surgical and uninjured shoulders were comparable (Tables 2 -4). This observation could suggest that the variability introduced by surgical procedures and baseline injury grades may not have significantly impacted the variability in calculated outcomes. Altogether, this initial investigation serves as a foundation upon which further in-depth research can be designed to assess ACJ treatments, with the goal of enhancing the short- and long-term shoulder girdle health in this predominantly young patient population.
Conclusion
DSX imaging is a promising tool for evaluating potential in vivo kinematic abnormalities in the ACJ during muscle-driven activities, laying the groundwork for further investigations in ACJ-reconstructed and nonreconstructed patients.
The study's findings furnished essential data for conducting power analyses and designing future studies with an adequate sample size to investigate the impact of different treatment approaches on ACJ kinematics.
Footnotes
Appendix
Surgical Procedures Performed a

| ID | Arthroscopic or Open | No. of Clavicle Tunnels | No. of Coracoid Tunnels | Fixation | Ligament |
|---|---|---|---|---|---|
| 1 | Artho. | 1 | 1 | Button × 2 | CC |
| 2 | Artho. | 1 | 1 | Button × 2 | CC |
| 3 | Open | 2 | 0 | Clavicle PEEK screw × 2 | CC |
| 4 | Artho. | 1 | 1 | Button × 2 | CC |
| 5 | Artho. | 1 | 0 | Button × 1 | AC + CC |
| 6 | Artho. | 1 | 1 | Button × 2 | CC |
| 7 | Artho. | 2 | 2 | Button × 2 | CC |
| 8 | Artho. | 0 | 0 | Cerclage | AC + CC |
| 9 | Artho. | 0 | 0 | Cerclage | AC + CC |
| 10 | Open | 0 | 0 | Cerclage | AC + CC |
| 11 | Open | 2 | 0 | Clavicle PEEK screw × 2 | CC |
Arthro., arthroscopic; AC, acromioclavicular; CC, coracoclavicular; PEEK, polyether ether ketone; ID, participant identification number.
Final revision submitted January 9, 2024; accepted February 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.G. has received consulting fees from Stryker, Arthrex, and Wright Medical Technology; nonconsulting fees from Arthrex and Wright Medical Technology; education payments from Medinc of Texas; and hospitality payments from Zimmer Biomet Holdings. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The University of Texas Health Science Center at Houston (reference no. HSC-MS-20-0585).