
Abstract
Background:
The use of bone–patellar tendon–bone (BPTB) and hamstring tendon (HT) autografts is common in anterior cruciate ligament reconstruction (ACLR). After ACLR, patients typically progress through specific rehabilitation milestones, and graft type may play a role in patient progression.
Purpose:
To compare the time to meet rehabilitation milestones between BPTB and HT autografts after ACLR.
Design:
Cohort study; Level of evidence, 3.
Methods:
This was a single-institution study on patients who underwent ACLR with either BPTB or HT autograft between June 2018 and July 2021. The primary outcomes were time to meet return-to-sport criteria, including >90% limb symmetry index (LSI) for isokinetic quadriceps and hamstring strength, horizontal hop, 4-crossover hop, and single-hop height. The time to satisfaction of each criterion was compared between graft groups using Wilcoxon tests and Cox proportional hazards models.
Results:
Included in the analysis were 410 participants who underwent ACLR with either BPTB (n = 232) or HT (n = 178). The BPTB group took longer to achieve >90% LSI for knee extension than HT (11.1 ± 4.1 vs 7.63 ± 2.8 months; P < .001). Similarly, the BPTB group took longer than the HT group to achieve >90% LSI for horizontal hop (11.4 ± 3.5 vs 9.82 ± 2.8 months; P < .001), 4-crossover hop (11.8 ± 3.6 vs 10.4 ± 2.8 months; P = .002), and single-hop height testing (11 ± 3.7 vs 8.81 ± 3.2 months; P < .001). The median time to achieve >90% LSI for hamstring strength was similar between groups (7.18 ± 3 vs 7.56 ± 3.1 months; P = .2).
Conclusion:
Patients that underwent ACLR with BPTB autograft took longer than patients with HT to meet commonly used postoperative rehabilitation milestones. Clinicians should consider these differences when guiding patients regarding graft choice, postoperative expectations, and rehabilitation.
Anterior cruciate ligament (ACL) injuries are common in athletes, with an incidence of 68.6 per 100,000 person-years, and these injuries often prevent them from returning to their prior activity level. 28 ACL reconstruction (ACLR) is the standard option for athletes that plan to return to sports. 27 However, the decision regarding graft type when performing ACLR is still heavily debated.15,16,33 Bone–patellar tendon–bone (BPTB) and hamstring tendon (HT) autografts are the mostly commonly used graft types, although both grafts have complication risks.15,33 BPTB grafts are associated with anterior knee pain, damage to the knee extensor mechanism, and infrapatellar contracture.13,31 In contrast, HT grafts are associated with dysfunction of the hamstring muscle itself, as well as both tibial and femoral tunnel widening.2,4,7,19 Although these complication risks are considered during graft selection, guidelines on when to use specific graft types are still debated.
The expected time needed to safely return a patient to his or her previous level of activity (deemed “return to sports” [RTS]) is another key area of consideration when selecting graft type. 6 After ACLR, patients typically follow specific strength and functional testing timelines and progress as they meet specific criteria. RTS criteria have been defined as a limb symmetry index (LSI) of 90% on all hop tests as well as on isokinetic strength testing,10,24,25 where LSI is defined as the value of the involved limb divided by the value of the uninvolved limb multiplied by 100 to obtain a percentage. However, these criteria continue to be an active area of research, and multiple variations of these guidelines have been established.6,23,29 Some evidence indicates that recovery time after ACLR is the strongest criterion associated with significant reduction in reinjury, where the lowest reinjury incidence occurs >9 months after ACLR. 1 An LSI of >90% for isokinetic strength testing of the quadriceps and hamstring and for functional testing (single-leg hop, triple hop, crossover hop) has also been suggested.11,26 Currently, most practices use some combination of the abovementioned criteria. 16
Using these functional tests as a guide, patients typically improve dramatically during the first 6 months after ACLR, with the majority of improvements occurring within the first 9 months.3,8,9 Previous studies examining knee stability and patient-reported outcomes between graft types have not shown significant differences,11,31 although some small studies have demonstrated that HT grafts may lead to faster improvements in strength and functional testing.13,34 There is currently limited evidence regarding the impact of graft type on the timeline of improvement.
In this study, we aimed to assess the association between time to meet common rehabilitation milestones and ACLR with either BPTB or HT autograft.
Methods
Cohort Selection
This study was deemed exempt from requiring institutional review board approval given that the data collection was part of the typical postoperative standard of care. The rights of the study patients were protected throughout the entire study. A registry of all ACL surgical procedures using either BPTB or HT at University of Wisconsin Health facilities was searched for patients who underwent ACLR between June 2018 and July 2021. We then identified patients who met >90% LSI for either strength testing, functional testing, or both, as well as those who had ≥6 months of follow-up for our analysis. Additional details regarding specific participants were obtained through medical records as needed.
Functional Outcome Performance Measurements
Starting at 3 months after ACLR surgery, functional testing was initiated to help objectively guide physical therapy interventions and was repeated approximately every 2 months (typically at 3, 5, 7, 9, and 12 months). At these visits, functional outcome performance testing and quadriceps and hamstring strength measurement testing were performed until passing criteria were met.
Quadriceps and hamstring strength measurements were collected using an isokinetic dynamometer (Biodex Medical Systems) for both the involved and the uninvolved limbs. Prior to isokinetic testing, all patients performed an active warm-up on a stationary bicycle for 5 minutes. For all testing procedures, patients were allowed a graded warm-up before data collection to acclimatize to the effort on the isokinetic dynamometer, then the uninvolved limb was tested first, followed by the involved limb. Isokinetic testing was performed at 60 deg/s, with 5 trials completed. When a patient met ≥70% LSI of the quadriceps peak torque on isokinetic testing, he or she was allowed to advance to impact training in the home program. For most individuals, this occurred at the 5- and 7-month testing time points.
Force plate countermovement jumping was also used during the rehabilitation program to help with offloading and overloading compensations as the patient initiated impact. Once the patient had moved from double-leg to single-leg impact activities in the home program, single-limb impact testing (3 tests) was initiated. A graded warm-up was completed before each maximal impact test. A single-leg hop for height was recorded using force plates (AMTI). Height (in meters) was computed using the time-in-air method,
Statistical Analysis
Data are presented as means ± SDs for continuous variables with a normal distribution and as medians with interquartile ranges for nonnormally distributed continuous variables. Categorical variables are presented as counts and percentages. Wilcoxon rank-sum tests and Wilcoxon effect sizes were used to compare differences between groups for continuous variables. The chi-square test and Cohen h effect size were used to compare differences between groups for categorical variables (effect sizes: <0.2 = small, 0.5 = moderate, and >0.8 = large). 32 Time-to-event analyses using Cox proportional hazards models and Kaplan-Meier curves were used to compare the probability of achieving >90% LSI over time between groups for all functional outcomes and isokinetic quadriceps and hamstring strength at 60 deg/s. Statistical significance was set at P < .05.
Results
A total of 609 patients were identified as having undergone ACLR. Within this cohort, 410 patients (232 in the BPTB group and 178 in the HT group), met >90% LSI for either strength testing, functional testing, or both and were included in this study. Significant differences were identified between the groups with respect to age, but not with respect to body mass index, weight, sex, leg length, height, or surgical side (Table 1).
Comparison of Demographic and Anthropometric Variables by Graft Type Among the Study Patients (N = 410) a
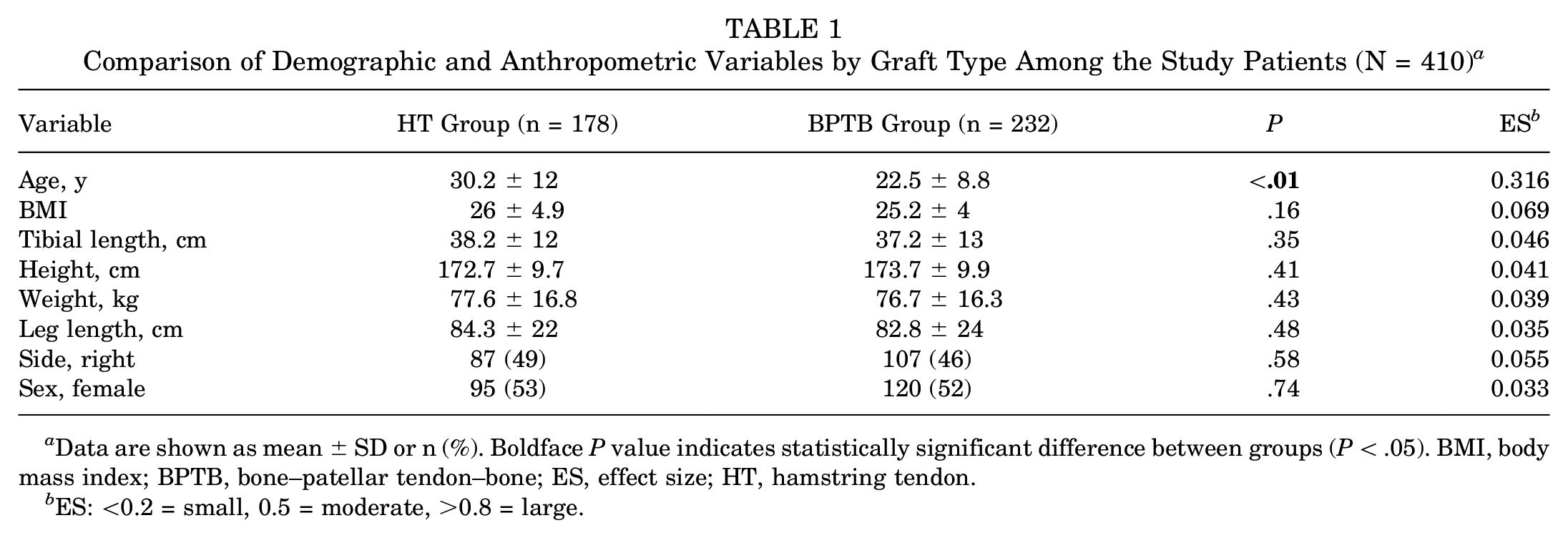
Data are shown as mean ± SD or n (%). Boldface P value indicates statistically significant difference between groups (P < .05). BMI, body mass index; BPTB, bone–patellar tendon–bone; ES, effect size; HT, hamstring tendon.
ES: <0.2 = small, 0.5 = moderate, >0.8 = large.
Strength Testing
First, we examined the median time to achieve >90% LSI between groups. The BPTB group had a greater median time to achieve >90% LSI for isokinetic quadriceps strength testing compared with the HT group. There was no statistically significant group difference in the median time to achieve >90% LSI for isokinetic hamstring strength testing (Table 2). In our time-to-event comparison between groups, the HT group had a greater probability of achieving >90% LSI at an earlier time point than the BPTB group with respect to quadriceps strength. Conversely, the BPTB group demonstrated a greater probability of achieving >90% LSI at an earlier time point with respect to hamstring strength testing (Figure 1, A and B).
Differences in Time to Achievement of 90% LSI With the Contralateral Limb by Graft Type a
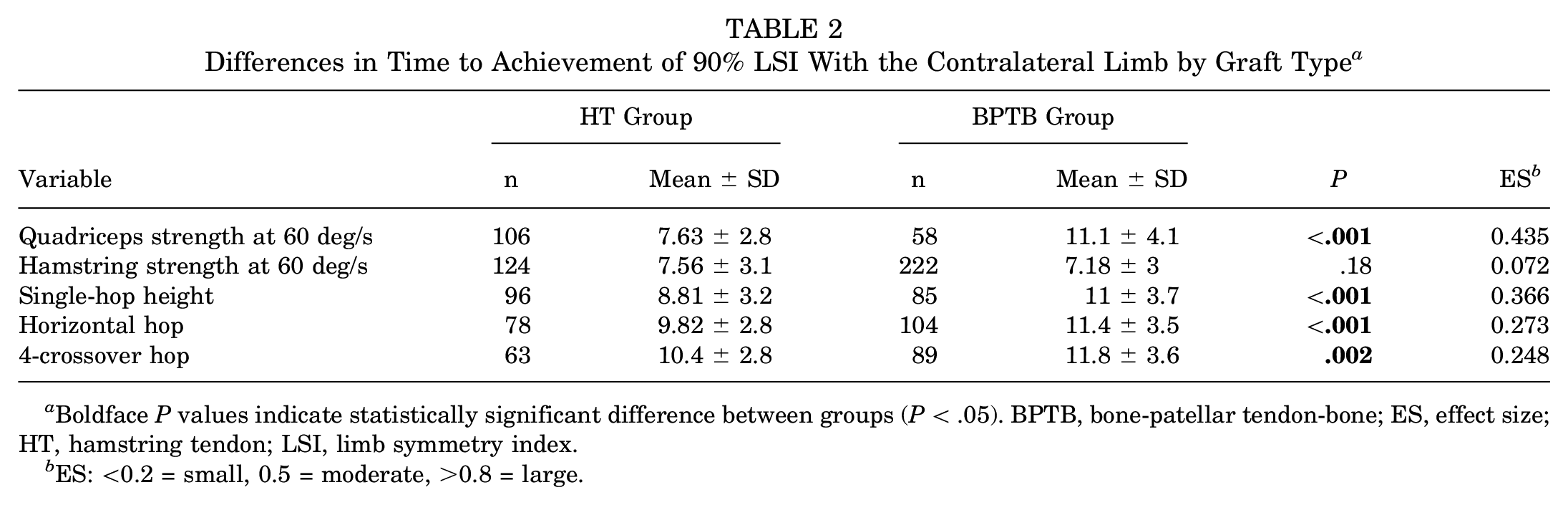
Boldface P values indicate statistically significant difference between groups (P < .05). BPTB, bone-patellar tendon-bone; ES, effect size; HT, hamstring tendon; LSI, limb symmetry index.
ES: <0.2 = small, 0.5 = moderate, >0.8 = large.

Results of Kaplan-Meier analyses demonstrating time to >90 LSI by graft type for (A) quadriceps strength at 60 deg/s, (B) hamstring strength at 60 deg/s, (C) single-hop height, (D) horizontal hop, and (E) 4-crossover hop. BPTB, bone–patellar tendon–bone; LSI, limb symmetry index.
Functional Testing
The BPTB group took longer than the HT group to achieve >90% LSI for all functional tests (single-hop height, horizontal hop, and 4-crossover hop) (Table 2; Figure 1, C-E).
Discussion
Strength Testing
Our primary finding was patients in the BPTB group took nearly 4 months longer to achieve >90% LSI for quadriceps strength when compared with the HT group. This agrees with previous research. Hart et al 12 demonstrated angle-specific weakness in knee extension in patients with BPTB grafts when compared with those with HT grafts. Among studies with smaller sample sizes, Miles et al 21 (n = 22) and Cristiani et al 5 (n = 40) demonstrated reduced isokinetic quadriceps strength in patients with BPTB grafts compared with those with HT grafts. These results may be due to anterior knee pain after ACLR using BPTB grafts. Anterior knee pain may inhibit performance during functional and strength testing as well as a patient’s ability to participate fully in rehabilitation exercises. 20 Given that the BPTB graft involves harvesting the middle one-third of the patellar tendon from the distal patellar pole to the tibial tubercle, this may compromise the extensor mechanism leading to residual quadriceps weakness.33,34 The BPTB group in the current study did demonstrate a greater probability of achieving >90% LSI at an earlier time point with respect to hamstring strength. However, there was no difference in the median time to meet >90% LSI in hamstring strength between groups when comparing those that ultimately met this criterion. This contrasts with previous literature, as Cristiani et al 5 demonstrated diminished hamstring strength in the HT group compared with the BPTB group, and Lesevic et al 17 showed diminished hamstring strength with HT grafts in female patients only. These findings suggest that while time to recover quadriceps strength after ACLR is greater among patients with BPTB grafts, time to recover hamstring strength may be similar among patients with HT grafts.
Functional Testing
We found that on all 3 functional tests, the patients with HT grafts were more likely to meet >90% LSI at an earlier time than patients with BTPB grafts. With respect to the mean time to meeting each criterion, the single-leg hop had the largest difference of 2.2 months followed by horizontal hop with 1.6 months and the 4-crossover hop with 1.4 months. Although there are limited studies comparing functional testing between graft types, Cristiani et al 5 found the BTPB group had significantly lower LSI for single-leg hop at 4 months compared with HT. However, no differences were seen at other time points. Our findings as a whole corroborate a prior study by Smith et al, 30 who found that patients with BPTB grafts took longer than patients with HT grafts to meet RTS criteria including strength and functional testing. These discrepancies may be again due to anterior knee pain, as mentioned above, as well as quadriceps weakness or an increased feeling of knee instability, which could impair functional testing after BPTB. These results reinforce the role of building quadriceps strength in patients early in the postoperative period after ACLR. Additional techniques such as blood flow restriction 14 and neuromuscular electrical stimulation therapies 22 have been shown to preserve lower extremity muscle mass. While the evidence is limited, these techniques may be considered as adjunctive options to build and maintain strength and limit potential issues with knee pain and instability that may delay strength and functional outcomes.
Patient Characteristics
Despite the BPTB group’s being composed of a younger cohort, they were still slower to reach rehabilitation milestones. Considering the faster recovery of the HT group, HT grafts may be better suited for individuals with lower physical demands, as it may incur a quicker return to work and activity. Although quadriceps strength may lag behind in the BPTB group, this may be a good option for younger athletes due to a potentially stronger graft with a reduced risk of reinjury over the long term. 18
Time to meeting strength and functional rehabilitation outcomes is an important part of decision-making for patients, particularly for those who are looking to return to high-impact activities. This information can aid clinicians as they strive to best educate patients regarding postoperative outcomes and timelines, maximize results during rehabilitation, and help athletes prepare for the demands of RTS.
Limitations
There are several limitations to this study. Most importantly, the groups were not formed randomly and variables that were related to both graft selection and the likelihood of achieving certain RTS criteria may have confounded the results. We also included all patients who underwent ACLR, which allowed a larger sample in the analysis but could potentially be a source of bias if additional variables such as concomitant injuries or recurrent ACL injury are related to both graft type and outcome. In addition, due to variations in patient follow-up, progressive testing was not always done at identical intervals among patients and a number of patients were lost to follow-up, sometimes before satisfying rehabilitation milestones. Our cohort was a combination of athletes and nonathletes with various motivation to meet RTS criteria, and preoperative conditioning was not standardized. The surgical procedures were also performed by multiple surgeons within our health system, who may have different criteria for graft selection.
Conclusion
Patients who underwent ACLR with BPTB autograft took longer than patients with HT autograft to meet commonly used postoperative rehabilitation milestones. Clinicians should consider these differences when guiding patients regarding graft choice, postoperative expectations, and rehabilitation.
Footnotes
Final revision submitted February 14, 2024; accepted March 5, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.E.W. has received hospitality payments from Smith + Nephew and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by University of Wisconsin Madison.