
Abstract
Background:
Management of isolated medial meniscus posterior root (MMPR) tears is challenging, especially in older patients, where indications for repair must be weighed against potential repair failure and osteoarthritic progression.
Purpose:
To compare patient-reported outcomes and incidence of failure after anatomic transtibial pullout repair for isolated MMPR tears in patients >60 versus ≤60 years of age.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included in the study were patients aged ≥18 years who underwent isolated anatomic transtibial pullout repair using either the single- or double-tunnel technique for MMPR tears at a single institution between January 2016 and September 2020. Patients with a minimum 2-year follow-up were divided based on age at surgery (>60 vs ≤60 years). Patients completed the International Knee Documentation Committee (IKDC), Knee injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS JR), and Veterans RAND 12-Item Health Survey (VR-12) Physical score preoperatively and at final follow-up. Differences between age groups in outcome scores as well as repair failures (defined as the need for repeat arthroscopy) were analyzed using the 2-sided Student t test or chi-square test.
Results:
A total of 20 patients aged >60 years (mean age, 65.7 ± 4.1 years; range, 60.2-74.9 years) were identified and compared against 40 patients aged ≤60 years (mean age, 49.3 ± 9.0 years; range, 23.4-59.8 years). Significant improvement on all outcomes scores was observed in both groups at final follow-up when compared with preoperative values, with no significant between-group difference on any of the scores at final follow-up. Revision repair was required in 1 patient (2.5%) in the ≤60-year group but not in patients in the >60-year group.
Conclusion:
Anatomic transtibial pullout repair for isolated MMPR tears resulted in improved IKDC, KOOS JR, and VR-12 Physical scores at minimum 2-year follow-up, with no significant differences between our cohorts of patients >60 versus ≤60 years of age.
The menisci serve an essential role within the knee, absorbing and transmitting compressive forces within the tibiofemoral joint during loading.20,39,42 The integrity of the medial meniscus posterior root (MMPR) is vital to ensuring proper function of the medial meniscus, serving to anchor the medial meniscus to the tibial plateau and effectively dispersing axial forces into hoop stresses during loading. 2 Tears involving the MMPR, either through avulsions at the tibial insertion or radial tearing within 1 cm of the root insertion,26,37 result in disruption of the circumferential fibers, leading to the loss of hoop stress generation.2,30 Consequently, MMPR tears effectively decrease the contact surface area of the meniscus, increasing articular cartilage contact pressures up to 25%2,18 and elevating the risk for chondral damage and the development of premature osteoarthritis.
MMPR tears comprise 10% to 21% of all meniscal tears,7,13,21,23,25 occurring in both younger and older patients. In younger patients, MMPR tears generally occur in the setting of athletic activity and usually in conjunction with ligamentous injuries. In older patients, tears are common in the setting of preexisting arthritic changes with or without a traumatic mechanism. 36 In patients with symptomatic MMPR tears, treatment options consist of an initial trial of nonoperative management, with surgical debridement or repair reserved for patients failing nonoperative treatment. While meniscal debridement of the torn root has been shown to provide moderate relief,8,22,40 excision of the posterior root has been reported to result in a knee that is functionally and biomechanically comparable with a meniscus-deficit knee given the crucial role of the MMPR to overall meniscal function and stability.2,32 The resultant increase in contact pressures accelerates the progression of degenerative changes within the medial compartment, leading to inferior patient-reported outcomes16,20 and a greater risk for conversion to total knee arthroplasty (TKA). 27 Meanwhile, anatomic repair of the MMPR has been reported to restore native anatomy, re-establishing the ability of the meniscus to absorb hoop stresses and effectively decrease tibiofemoral contact pressures to levels comparable with a native knee.10,32,35 As a result of the deleterious effects on knee health after debridement, preservation of the MMPR through repair is generally recommended in patients without high-grade, bipolar degenerative changes within the medial compartment. 1
While MMPR repair is generally considered the gold standard for younger patients to restore function and enable return to activity, concerns exist in older patients due to decreased vascularity to the meniscal tissue, which may impair successful healing as well as the greater likelihood for preexisting arthritic changes.4,17,38 Traditionally, older age has been viewed as a contraindication to MMPR repair; however, with an increasing number of MMPR repairs performed in the United States in patients of all ages, 1 renewed focus has been placed on outcomes in older patients after MMPR repair.
The purpose of this investigation was to compare patient-reported outcomes and failure rates in patients aged >60 years versus patients ≤60 years after MMPR repair using an anatomic transtibial pullout technique with minimum 2-year follow-up, while also recording the incidence of repair failures.17,20 We hypothesized that based on prior investigations,16,20,29 no significant difference in patient-reported outcomes or failure rates would be found between these age groups.
Methods
Study Design
Before study initiation, institutional review board approval was obtained for the study protocol. A retrospective review of a prospectively collected institutional database (PatientIQ) was performed to identify all patients who underwent isolated MMPR repair between January 2016 and September 2020. Included were patients aged ≥18 years who underwent MMPR repair utilizing an anatomic transtibial pullout technique with either a single or double tunnel and who had minimum 2-year follow-up. Exclusion criteria consisted of the following: (1) patients with any history of prior procedures to the surgical knee, (2) performance of any concomitant procedures (ie, anterior cruciate ligament reconstruction, lateral meniscal repair, high tibial osteotomy) at the time of MMPR repair, and (3) incomplete or missing patient-reported outcome scores. The study patients were divided into 2 groups based on their age at the time of surgery: an experimental group of patients aged >60 years and a control group of patients aged ≤60 years who were matched 2:1 according to final follow-up (±5 months) and BMI (±3 kg/m2).
Surgical Technique and Rehabilitation
MMPR repair was performed using an anatomic transtibial pullout technique utilizing single or double transtibial tunnels, as previously described. 11 In brief, standard anterolateral and anteromedial portals were created. After a standard diagnostic arthroscopy, the location and type of MMPR tear was identified, while ruling out the need for any concomitant procedures. To increase visibility, fenestration of the medial collateral ligament can be performed to increase compartment size and decrease the risk of iatrogenic chondral injury. If necessary, releases may be performed to ensure the MMPR can be mobilized to its anatomic insertion on the tibia. An additional accessory anteromedial portal can be created to more easily access the torn root. The tibial footprint of the MMPR was then decorticated using a curved curette and arthroscopic shaver, while a rasp may be utilized to help stimulate vascularity along the root. An aiming guide was then positioned at the native attachment of the MMPR, and a 2-cm incision was created just medial to the tibial tubercle using the guide. A transtibial tunnel was then created using a drill, followed by the insertion of a passing suture. The necessary number of sutures (1-3) were passed through the MMPR with the use of an arthroscopic suture-passing device and were then shuttled through the transtibial tunnel with the assistance of the passing suture. For a double-tunnel repair, an offset guide was utilized to drill an additional transtibial tunnel, and the steps were repeated. Once satisfactory passage of the sutures through the transtibial tunnel was performed, the knee was placed in 90° of flexion, and the sutures were secured to the tibia using either a button or a suture anchor (Figure 1).
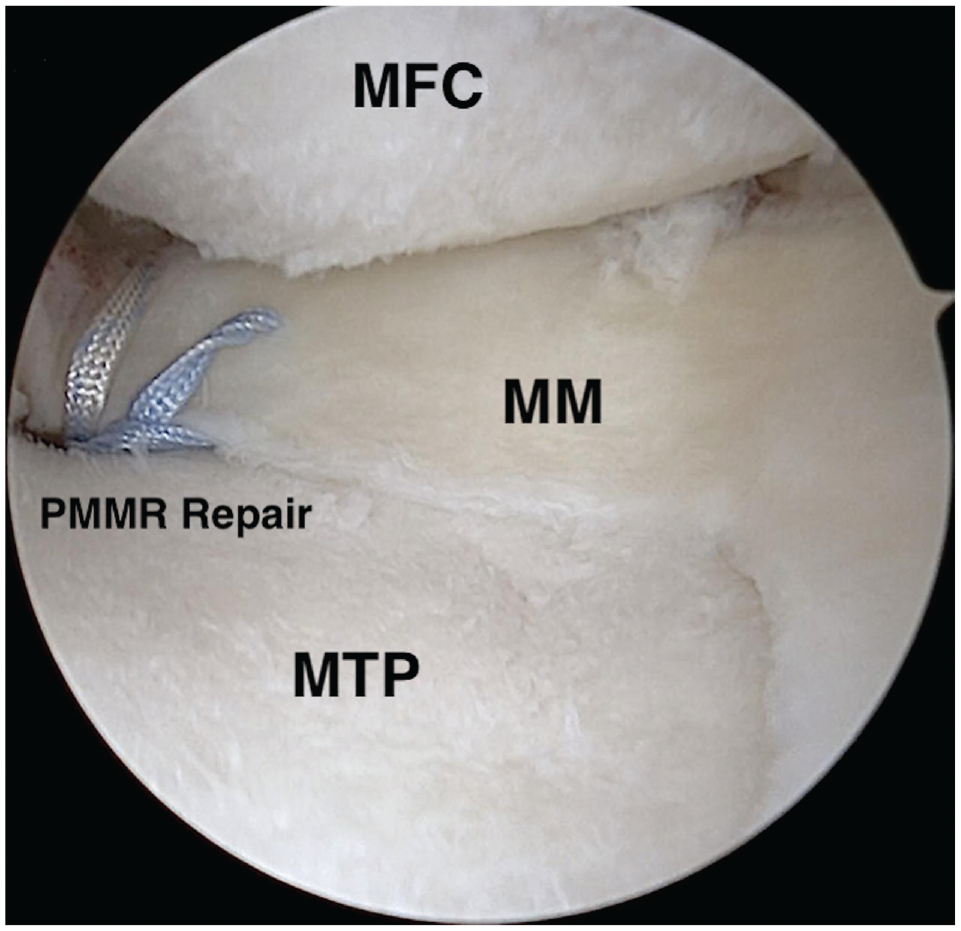
Arthroscopic view of the anteromedial compartment of the knee demonstrating successful restoration of the medial meniscus posterior root (MMPR) to the native tibial insertion using transtibial suture pullout technique. MFC, medial femoral condyle; MM, medial meniscus; MTP, medial tibial plateau; PMMR, same as MMPR as defined in caption.
After surgery, patients remained nonweightbearing in a hinged knee brace in extension during ambulation using crutches for a total of 6 weeks. Active and passive range of motion was limited to 0° to 90° during the first 2 weeks, with progression to full range of motion by 4 to 6 weeks. Patients were allowed to gradually advance weightbearing to full beginning at 6 weeks, with the discontinuation of crutches and knee bracing when quadriceps strength was adequate. Beginning at 8 to 12 weeks after surgery, patients progressed with strengthening activities using closed-chain exercises and then to single-leg exercises at 12 to 16 weeks. Full return to sport and activity generally occurred at approximately 24 weeks after surgery.
Patient Evaluation and Data Analysis
Patient charts were retrospectively reviewed by 2 independent investigators (G.R.J., J.S.). Patient characteristics were collected using the electronic medical records and included age, sex, body mass index (BMI), time from injury to surgery, and final follow-up time. Preoperative standing, hip-to-ankle radiographs—which are standard-of-care for all patients in the practice of the senior author (J.C.)—were reviewed, with the mechanical axis of the knee calculated. This was performed in the following manner: a line (line 1) was first drawn from the center of the femoral head to the center of the tibial plafond, followed by line 2, drawn parallel to the tibial plateau starting from the medial border and ending on the lateral border of the tibial plateau. Line 3 was then drawn from the tibial plateau medial edge to the intersection of the first line. The mechanical axis was then calculated by dividing the length of line 3 by the length of line 2 and was expressed as a percentage. The medial border of the tibial plateau was equivalent to 0%, while 100% was equivalent to the lateral border.
The severity of osteoarthritis was graded by 2 independent investigators (D.J.K., J.R.M.) on preoperative weightbearing anteroposterior radiographs of the knee using the Kellgren-Lawrence (K-L) classification. Preoperatively and at final patient follow-up, International Knee Documentation Committee (IKDC), Knee injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS JR), and Veterans RAND 12-Item Health Survey (VR-12) Physical scores were recorded. The incidence of any repair failures, defined by the need for a revision of the primary MMPR repair during the study period, were recorded.
Statistical Analysis
Descriptive statistics were used to report differences in characteristics between the age groups (>60 vs ≤60 years). Categorical variables were reported as counts, and continuous variables were reported as means with standard deviations. Two-sided Student t tests and chi-square tests were used to assess differences in the continuous and categorical variables between the age groups. The level of significance was established at a 2-sided alpha level of P < .05. All statistical analyses were performed utilizing R (Version 4.2.2; R Foundation for Statistical Computing).
Results
Patient Characteristics
A total of 45 patients >60 years of age at surgery at the time of MMPR and with minimum 2-year follow-up were identified in our institutional registry. Of these patients, 8 (17.8%) were excluded due to a prior history of knee surgery and 5 (11.1%) were excluded due to concomitant ligamentous or cartilage procedures. Of the remaining 32 patients, 20 had complete patient-reported outcome scores at follow-up (62.5% overall compliance) and were included in the study as the experimental group. The mean age of the cohort was 65.7 ± 4.1 years (range, 60.2-74.9 years) and the mean final follow-up was 31.8 ± 9.4 months (range, 24.0-51.6 months). Meanwhile, a 2:1 matched cohort consisting of 40 patients aged ≤60 years (mean age, 49.3 ± 9.0 years; range, 23.4-59.8 years) and a mean follow-up of 31.3 ± 8.2 months (range, 24.0-56.3 months) was identified as the control group. There were no significant differences between the groups based on sex (P = .84), follow-up time (P = .85), BMI (P = .95), or mechanical axis measurements (P = .79) (Table 1).
Patient Characteristics Based on Age Group a

Data are reported as mean ± SD (range) or No. of patients. K-L, Kellgren-Lawrence.
Patient-Reported Outcomes
At final follow-up, IKDC, KOOS JR, and VR-12 Physical scores were significantly improved in both age groups when compared with preoperative values (Table 2). No significant difference in any outcome score at final follow-up was observed between the age groups (Table 3).
Preoperative and Postoperative Patient-Reported Outcome Scores Based on Age Group a

Data are reported as mean ± SD (range). IKDC, International Knee Documentation Committee; KOOS JR, Knee injury and Osteoarthritis Outcome Score for Joint Replacement; VR-12, Veterans RAND 12-Item Health Survey.
Patient-Reported Outcomes Based on Age Group a
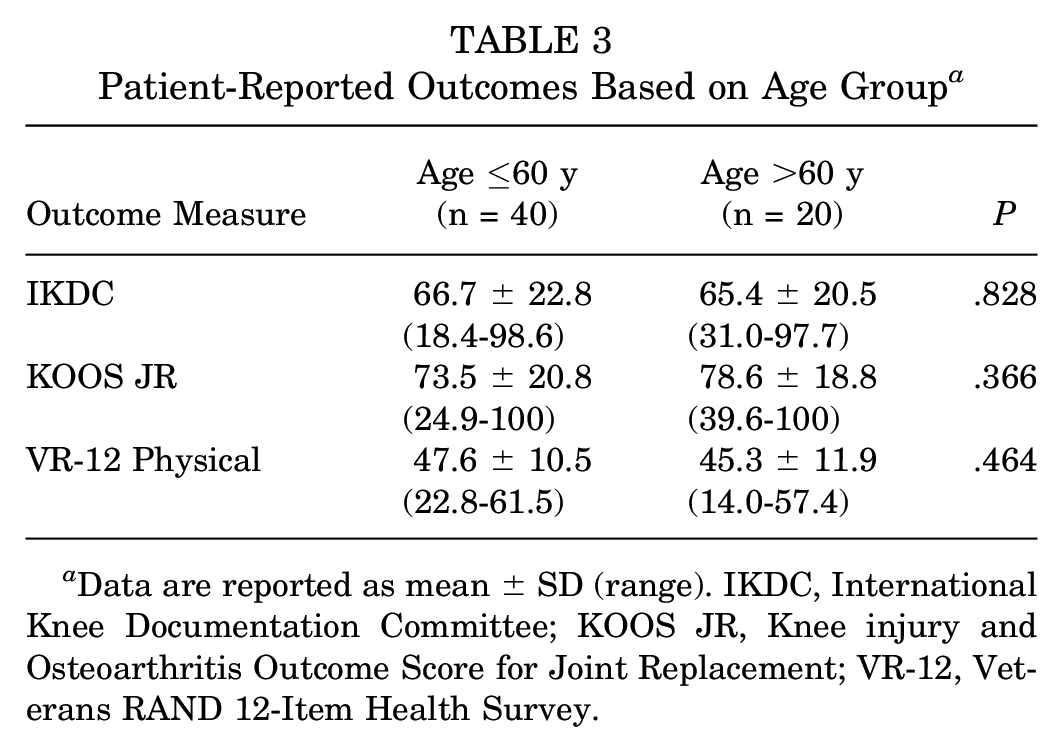
Data are reported as mean ± SD (range). IKDC, International Knee Documentation Committee; KOOS JR, Knee injury and Osteoarthritis Outcome Score for Joint Replacement; VR-12, Veterans RAND 12-Item Health Survey.
Revision Procedures
One patient in the ≤60-year age group (2.5%) required revision MMPR surgery. No revisions were documented in patients aged >60 years.
Discussion
The primary finding from this investigation was that patients aged >60 years who underwent isolated MMPR repair using either single or double transtibial tunnels reported significant improvements in IKDC, KOOS JR, and VR-12 Physical at minimum 2-year follow-up. No significant differences in outcome scores at final follow-up were appreciated when comparing patients aged >60 versus ≤60 years. No revision repairs were observed after MMPR repair in patients aged >60 years.
Significant improvements in IKDC, KOOS JR, and VR-12 Physical scores were reported at final follow-up in patients both >60 and ≤60 years of age after MMPR repair. These results are comparable with those reported by LaPrade et al 29 in their investigation evaluating outcomes after medial or lateral meniscus root repair in patients aged <50 years (n = 35) versus ≥50 years (n = 15). Specifically, in 45 patients who underwent posterior root repair (n = 15 lateral meniscus root tear, n = 35 medial meniscus root tear), no significant differences were found at a minimum 2-year follow-up when comparing postoperative Lysholm, Western Ontario and McMaster Universities Osteoarthritis, 12-Item Short Form Health Survey Physical Component Summary and Mental Component Summary, Tegner activity level, or patient satisfaction. 29 Revision surgery was performed in 6.7% (3 of 45) of the patients, with all failures occurring in patients aged <50 years with MMPR tears. As a result, LaPrade et al advocated that patients aged ≥50 years not be excluded from consideration for possible MMPR repair based on chronological age alone.
While not directly compared in this investigation, the performance of MMPR repair over meniscectomy in appropriately selected patients has been shown to lead to greater clinical improvement postoperatively. Husen et al 20 examined 32 patients aged ≥60 years (mean age, 64.5 ± 4.6 years), with a majority of tears (56.8%) involving the posterior root of the medial meniscus. When evaluating patients after MMPR repair versus meniscectomy matched by age, sex, and BMI as well as meniscal tear type, the authors noted significant improvement in IKDC, KOOS, and Lysholm scores (P < .001 for all) in patients at a mean of 42.2 months (range, 13-128 months) after repair. 20 Meanwhile, in their comparative cohort investigation, Chung et al 16 observed that in 37 patients (mean age, 55.5 ± 7.1 years) who underwent MMPR repair versus 20 patients treated with meniscectomy (mean age, 55.0 ± 14.0 years), patients in the repair group reported significant improvement in Lysholm (P = .002) and IKDC (P < .001) scores at minimum 5-year follow-up. Moreover, a significantly slowed progression of K-L grade (P = .005) and medial joint-space narrowing (P < .001) was observed after repair, while the rate of conversion to TKA was 0% after repair versus 35% in patients after meniscectomy. Similarly, when comparing patients aged ≥40 years who underwent meniscal repair (n = 35; mean age, 48.5 ± 7.0 years) versus meniscectomy (n = 131; mean age, 52.8 ± 7.1 years), Engler et al 17 reported no significant differences in median IKDC or Marx activity score at 5-year follow-up. As such, while additional studies examining long-term outcomes and knee longevity after repair versus debridement are warranted, additional factors beyond chronologic age should be considered during the decision-making process in the treatment of older patients with symptomatic MMPR tears.
However, the performance of meniscus root repair in older patients continues to be a source of debate among surgeons. 19 As the primary limiting factor to successful healing after root repair is tissue vascularity, 4 it is essential to consider the decrease in blood supply to the meniscus that occurs with increasing patient age. 38 As a result, higher failure rates may be expected in older patients undergoing MMPR tears when compared with younger patients.5,34 While not relying solely on chronologic age as a single determining factor when deciding between meniscectomy versus repair, a number of patient-specific variables should be considered. Chung et al 15 observed that at a minimum of 5-year follow-up after MMPR repair, in a predominately female cohort with a mean age of 56 years, the presence of chondral damage consistent with Outerbridge and International Cartilage Regeneration & Joint Preservation Society grade ≥3 as well as the presence of varus malalignment were independent risk factors for poor outcomes after both meniscal repair and meniscectomy. Krych et al27,28 further observed that the presence of K-L grade ≥2 was associated with a higher risk for conversion to TKA. Additional factors, including higher BMI 10 and the ability of patients to remain compliant with postoperative weightbearing restrictions, should also be considered during decision-making in older patients with MMPR tears. 33
Concern regarding repair integrity and durability after MMPR repairs in older patients is further warranted given the risk for arthritic progression after arthroscopic intervention. The presence of osteoarthritic changes in older patients with MMPR tears is high, with Choi et al 14 reporting concomitant arthritis in 42.5% of the 248 patients (mean age, 53.5 years) evaluated in their investigation. However, when compared with other management options, MMPR repair has been shown to effectively slow the progression of arthritic degeneration. Specifically, Bernard et al 6 observed that when comparing 45 patients with MMPR tears equally allocated and matched based on meniscal laterality, age, sex, and K-L grade to nonoperative (n = 15) versus meniscectomy (n = 15) versus root repair (n = 15), patients who underwent repair possessed significantly less arthritic progression based on changes in K-L grade at a mean follow-up of 74 months. A 2022 systematic review by Chang et al 12 evaluating 28 studies (n = 994 patients; mean age, 57.1 years) that assessed midterm outcomes after MMPR repair reported that 49% of patients had radiographic progression of ≥1 K-L grade at a mean follow-up of 4 years (n = 11 studies). This rate was noted to be substantially lower than the rate of arthritic progression reported in patients after meniscectomy in prior investigations, which ranged from 58% to 100% (mean, 76%).16,24,30 As a known risk factor for arthritis progression, 41 multiple investigations have demonstrated that the amount of meniscus resected has a substantial impact on the progression of radiographic arthritis.3,9,16 As such, while successful MMPR repair does not cease the progression of knee osteoarthritis, when compared with partial meniscectomy, arthritic progression may be decelerated.16,31
Limitations
This study is not without its limitations. Despite the prospective collection of data, the data were reviewed retrospectively, with a significant likelihood for potential selection bias. As a result of the indications inherent in performing MMPR repair in patients >60 years, our investigation was limited to a small sample size of patients meeting the appropriate inclusion criteria. This small sample size limited our ability to obtain adequate power to perform any meaningful statistical analyses between age groups. Patients were not graded by preoperative MRI for assessment of cartilage status, potentially confounding the results. No repeat MRI or second-look arthroscopy was performed to assess the rate and completeness of healing, prohibiting our ability to diagnose any subclinical repair failures that did not require revision surgery. Additionally, as all patients were treated at a specialized, tertiary care center, the results of this investigation may not be generalizable to the general population. While all included patients were undergoing transtibial anatomic repair of the MMPR, the decision to utilize a single- versus double-tunnel technique was made at the discretion of the operating surgeon, and the lack of surgical standardization limits the external validity of these findings for surgeons utilizing different techniques.
Conclusion
Anatomic transtibial pullout repair for isolated MMPR tears resulted in improvement in IKDC, KOOS JR, and VR-12 scores at minimum 2-year follow-up, with no significant differences in our cohorts of patients >60 versus ≤60 years of age.
Footnotes
Final revision submitted January 26, 2024; accepted February 29, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.M.K. has received grant support from Arthrex and Medical Device Business Services, education payments from Arthrex and Smith+Nephew, honoraria from Encore Medical, and hospitality payments from Stryker. O.A.O. has received education payments from Medwest Associates. J.R.M. has received education payments from Medwest Associates and hospitality payments from Medical Device Business Services. N.N.V. has received consulting fees from Arthrex and Stryker; nonconsulting fees from Arthrex; royalties from Arthrex, Smith+Nephew, and Graymont Professional Products; and hospitality payments from Spinal Simplicity and Relievant Medsystems. J.C. has received grant support from Arthrex; education payments from Arthrex and Smith+Nephew; consulting fees from RTI Surgical, Smith+ Nephew, Vericel, Arthrex, DePuy, and Linvatec; nonconsulting fees from Smith+Nephew, Arthrex, Medical Device Business Services, and Linvatec; and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center (ref No. 00000482).