
Abstract
Background:
Management of radial head fractures around the elbow with open techniques can predispose to edema, postoperative pain, and adhesions. The resultant limitation in elbow range of motion negatively affects functional outcomes. Rehabilitation is then rendered a challenge in a joint with proneness to stiffness.
Hypothesis:
Arthroscopic percutaneous fixation of Mason type 2 radial head fractures would provide satisfactory radiological and clinical outcomes.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 24 patients diagnosed with isolated Mason type 2 radial head fractures at a single institution between February 1, 2021, and December 31, 2021, received arthroscopic percutaneous fixation by headless screws. Functional evaluation included Mayo Elbow Performance Score and postoperative elbow range of motion measurements. Radiological evaluation was performed using elbow radiographs and computed tomography scans. Patients were evaluated for a minimum of 24 months.
Results:
This study included 12 male and 12 female participants with a mean age of 37.29 ± 11.93 years. At the end of the follow-up period (mean, 27.75 months; range, 24-32 months), the mean elbow flexion was 140.17° ± 8.21° and the extension deficit was 4.17° ± 3.81°. The Mayo Elbow Performance Score revealed 21 patients with excellent results and 3 patients with good results. All patients returned to preinjury activities at a mean time of 3.1 months (range, 2-6 months) postoperatively. Union was reached in all patients at a mean time of 7.63 weeks (range, 6-10 weeks). No neurological complications or reoperations were reported at the end of the follow-up period.
Conclusion:
Arthroscopic fixation was demonstrated to be a valid and valuable technique for managing isolated Mason type 2 radial head fractures. It allowed for accurate reduction without the need for soft tissue dissection, resulting in excellent clinical outcomes.
Radial head fractures constitute around 33% of fractures around the elbow and up to 5% of all fractures.20,29 Injury patterns can include sole fractures in addition to those associated with complex elbow fractures or dislocation. 20 Appropriate management of these fractures is crucial owing to the role played by the radial head in elbow stability. 28 The most commonly utilized classification is the Mason classification, 19 which was later modified by Hotchkiss to outline treatment options for each fracture pattern. 17 Type 1 fractures include those with displacement <2 mm, type 2 fractures are those with >2 mm of displacement with or without mechanical block, and type 3 fractures are highly comminuted fractures that are nonreconstructable.17,19 Type 1 fractures are generally treated nonoperatively,34,35 and type 3 fractures require radial head replacement since acute excision has been deemed obsolete. 12 Management of type 2 fractures, however, has not been as clear-cut in comparison.12,41 Debates exist in the treatment of type 2 fractures in addition to the indications for open reduction and internal fixation (ORIF). 30 Good midterm results were reported with nonoperative management in patients presenting with no mechanical block. 13 Satisfactory outcomes have been described by some authors after conservatively managing fractures with 5 mm of displacement, no comminution, or block to motion.3,15 However, a 12% rate of delayed radial head excision was reported.3,15 After long-term follow-up, radiocapitellar arthritis was found in patients managed nonsurgically, even in the absence of block. 3 Consequently, other authors have recommended fixation of type 2 fractures regardless of the presence of mechanical block to avoid these delayed complications.6,22
Elbow arthroscopy has developed greatly and is currently considered a standard technique to evaluate and treat elbow pathologies. Indications of elbow arthroscopy have been consistently expanding to include acute fracture fixation. 18 In the setting of a radial head fracture, arthroscopy allows direct visualization of the articular surfaces. Concomitant injuries to the capitellum and coronoid can also be assessed without extensive soft tissue dissection. 14 The aim of this study was to evaluate the radiological and functional results after arthroscopic percutaneous fixation of Mason type 2 radial head fractures. Our hypothesis was that the arthroscopic percutaneous fixation technique would provide satisfactory radiological and early clinical outcomes.
Methods
Patient Selection
Research ethics committee approval was obtained for this study, and written informed consent was obtained from all included patients. Patients with isolated Mason type 2 radial head fractures who were admitted to our hospital between February 1 and December 31, 2021, were considered for this study. Inclusion criteria included isolated Mason type 2 fractures with an injury onset not exceeding 2 weeks in a skeletally mature patient. Exclusion criteria were open fractures, concomitant elbow dislocation, ligamentous injury, and associated neurological injury.
After considering the study inclusion and exclusion criteria, 24 consecutive patients with a minimum follow-up of 24 months were included in this case series. Power analysis using G*Power (3.1.9.7 Heinrich-Heine-Universität Düsseldorf) indicated that a minimum sample size of 15 patients was needed at a 95% level of significance, P value of <.05, and power of 0.95. Sample size calculation was based on the response rates of a study of arthroscopic radial head fracture management by Michels et al. 27
Surgical Technique
All study patients were treated by arthroscopic percutaneous fixation of radial head fractures performed by the same senior surgeon (A.E.S.), with expertise in arthroscopy. Patients received general anesthesia and were placed in a lateral decubitus position. Bony prominences were adequately padded. The shoulder was positioned at approximately 90° of abduction with the elbow flexed to 90° to allow clearance of elbow flexion. The arm was supported via an arm holder in such fashion as to permit free suspension of the elbow and forearm (Figure 1).
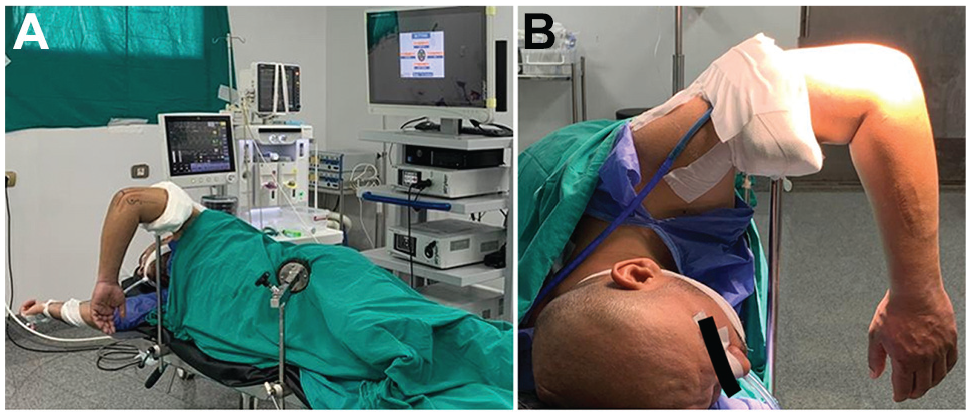
(A) Operating room setup and patient position. (B) Arm position to allow elbow flexion.
After tourniquet application, elbow motion was checked to ensure sufficient range of flexion up to 110°. The arm was then secured to a holder to prevent any alterations in position and subsequent loss of established portals during the procedure. Important anatomic landmarks (medial and lateral epicondyles, olecranon, triceps tendon, head radius, and ulnar nerve) were marked to guide portal placement (Figure 2).
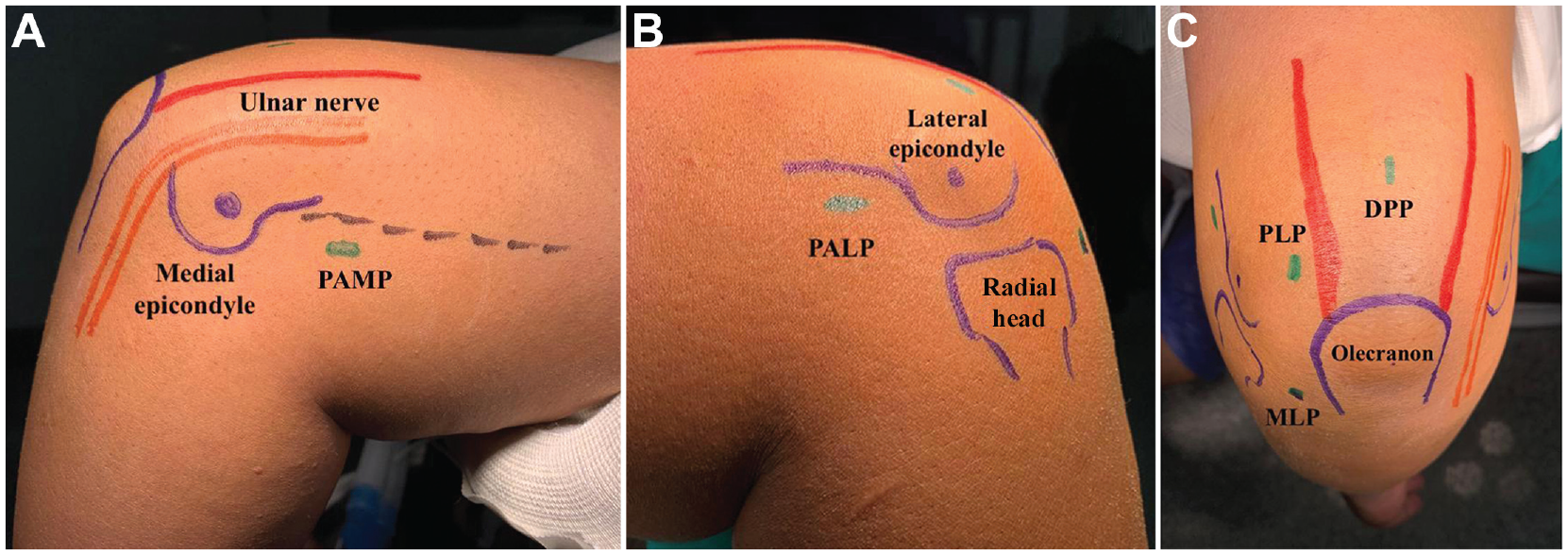
Portal markings. (A) Medial side of the left elbow showing the anteromedial portal (2 cm proximal to the medial epicondyle and 2 cm anterior to the intermuscular septum). (B) Lateral side of the left elbow demonstrating the anterolateral portal (2 cm proximal and anterior to the lateral epicondyle). (C) Posterior aspect of the left elbow showing posterior portals. DPP, direct posterior portal; MLP, midlateral or soft-spot portal; PALP, proximal anterolateral portal; PAMP, proximal anteromedial portal; PLP, posterolateral portal.
The pump pressure was set to 35 mm Hg. After sterilization and draping, the tourniquet was inflated to 250 mm Hg. The elbow was then insufflated using 20 cm of saline through the soft spot. Elbow extension indicated successful intra-articular injection (Video Supplement 1). The first portal utilized was the proximal anteromedial portal. Sharp incision of the skin was done using a No. 15 blade, followed by blunt dissection.
The anterior elbow was then viewed using a 30°, 4.5-mm arthroscope (Figure 3) and examined for any concomitant intra-articular pathologies (Video Supplement 2). The proximal anterolateral portal was next established under vision as a working portal. A shaver was inserted to debride the synovium and hematoma to allow for radial head visualization. Supination and pronation of the forearm confirmed the position of the radial head and the fracture fragments.
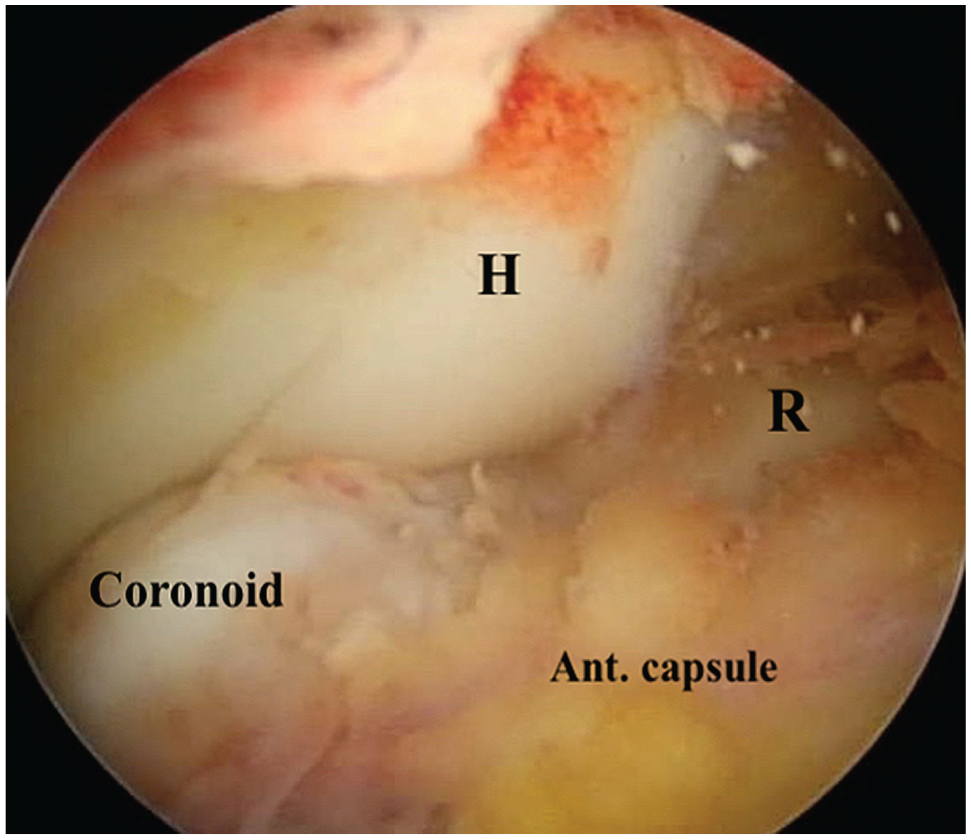
Anterior elbow anatomy identified via the proximal anteromedial portal. Ant., anterior; H, humerus; R, radial head.
Reduction of the fragment through the anterior or posterior portals was tailored according to fracture pattern, although fixation was performed through the posterior portals in all patients. The arthroscope was then shifted to the posterior elbow through the posterolateral portal. A switching stick was inserted through the anterior portals to preserve their position throughout the procedure. Through the posterolateral portal, the arthroscope was slid along the lateral edge of the olecranon to allow direct visualization of the posterior elbow and radiocapitellar joint (Figure 4). Removal of synovium folds along with any residual soft tissue impeding the view was performed through the soft spot (midlateral) portal. Gentle debridement of the proximal edge of annular ligament only at the site of screw insertion is crucial for accurate position in relation to the articular surface, avoiding intra-articular penetration (Video Supplement 3). Supination while the elbow was flexed at 90° was performed to bring the fragment into view. Manipulation of the mobile fragment was carried out via a blunt probe through the midlateral portal. Upon attaining adequate reduction, impaction of the fracture fragment was achieved by forearm rotation to maintain the reduced position (Video Supplement 4).

View from the posterolateral portal of the posterior elbow. Sigmoid notch and bare area of the olecranon articular surface can also be seen. C, capitellum; R, radial head; T, trochlea.
A K-wire was inserted percutaneously via a separate snip incision as an anti-rotatory wire or to aid reduction before screw placement if the fragment was unstable. In some instances, we utilized an intra-articular radiocapitellar reference K-wire to act as a guide to the fixating wire, ensuring its proper direction (Figure 5). A 1.2-mm wire was then drilled percutaneously through the fracture fragment via the midlateral portal. Correct positioning of the K-wire was then checked via the C-arm. If maximum supination was not sufficient for adequate fragment access, the guide wire was inserted retrograde in a posteroanterior fashion through radiographic guidance (Figure 6). The arthroscope was then switched back to the anterior elbow to ensure precise position of the guide wire. A 2-mm cannulated drill bit was then carefully placed. A 2.7-mm cannulated headless screw was then inserted through the guide wire (Video Supplement 5).

View from the posterolateral portal of the reference K-wire in the radiocapitellar joint with trajectory perpendicular to the fracture line. C, capitellum; R, radial head.

Intraoperative lateral view imaging of the elbow. (A) Reducing K-wire, with switching stick (blue asterisk) and arthroscope (red asterisk) in the anterior elbow. (B) After reduction and insertion of the guidewire.
Visualization of the radial head arthroscopically was performed to ensure fracture compression (Video Supplement 6). Screw position and length were then checked radiographically; the length ranged from 16 to 20 mm. Forearm rotation was carried out to confirm the absence of any blockage to range of motion. Portals were then closed via interrupted nonabsorbable sutures, then sterile dressing was applied.
Postoperatively, the elbow was placed in an arm sling for 2 weeks. Early active-assisted range of motion was encouraged on postoperative day 1 as tolerated and was continued for 2 weeks. Active and passive elbow range of motion exercises were then initiated gradually. Strengthening exercises were started after confirming fracture union and continued until preinjury activity was regained.
Evaluation
Clinical and radiological assessments were performed by 2 authors separately (M.R.K.I. and M.H.), then a mean was obtained. Clinical evaluation included postoperative active elbow flexion, extension, supination, and pronation. A goniometer was used to measure elbow range of motion. The Mayo Elbow Performance Score (MEPS), which includes parameters for pain, range of motion, stability, and function, was also utilized (Table 1). 24 MEPS grading is classified as excellent (90-100), good (75-89), fair (74-60), or poor (<60).
Mayo Elbow Performance Score a
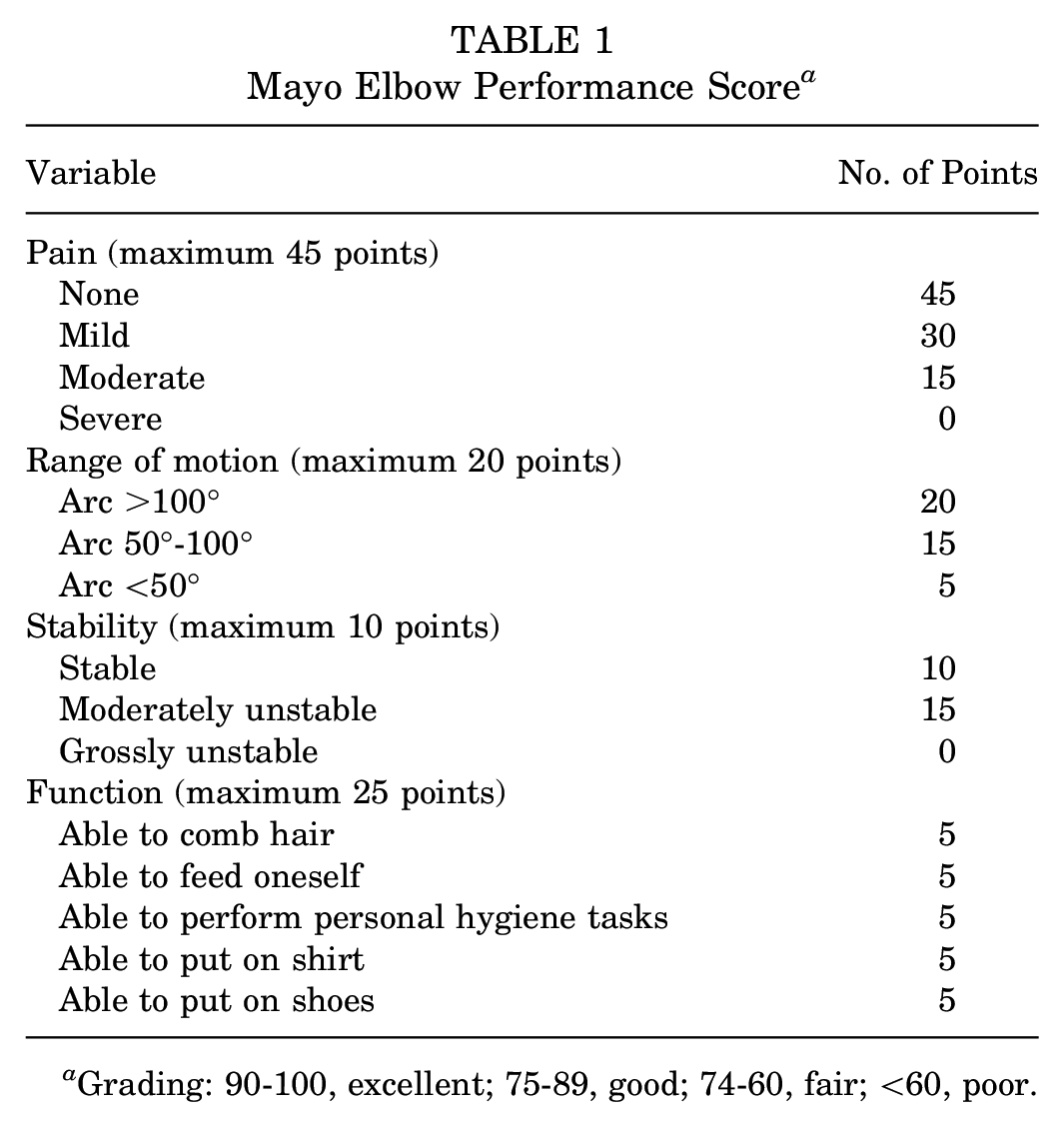
Grading: 90-100, excellent; 75-89, good; 74-60, fair; <60, poor.
Imaging evaluation comprised conventional elbow radiographs as well as computed tomography (CT) scans with 3-dimensional reconstruction. Preoperative elbow radiographs and CT scans were performed routinely to judge fracture classification. Patients also underwent conventional radiographs immediately postoperatively and at 6, 8, and 10 weeks postoperatively depending on when union was reached. CT scans were performed to confirm signs of union. Radiological union was determined based on the findings of bridging trabeculae, nonvisible fracture line, and absence of lucency at the fracture site.
All complications and return to the operating room were recorded.
Statistical Analysis
Data were analyzed using IBM SPSS software package version 20.0 (IBM Corp). Qualitative data were described using number and percentage. Quantitative data were described using means with standard deviations and medians with ranges.
Results
There were 24 patients included in the analysis, with no patients lost to follow-up. The study population comprised an equal number of male and female participants. The mean age was 37.29 years (range, 19-63 years). A total of 13 patients had an injury of their right arm (54.2%) whereas the left arm was injured in 11 patients (45.8%). The dominant side was fractured in 15 patients (62.5%). The mean follow-up period was 27.75 months (range, 24-32 months). The characteristics of each included patient are detailed in Appendix Table A1 and are summarized in Table 2. Postoperative parameters are summarized in Table 3.
Summary of Patient Characteristics (n = 24) a

Data are reported as n (%) unless otherwise indicated.
Distribution of Patients According to Postoperative Parameters (N = 24) a
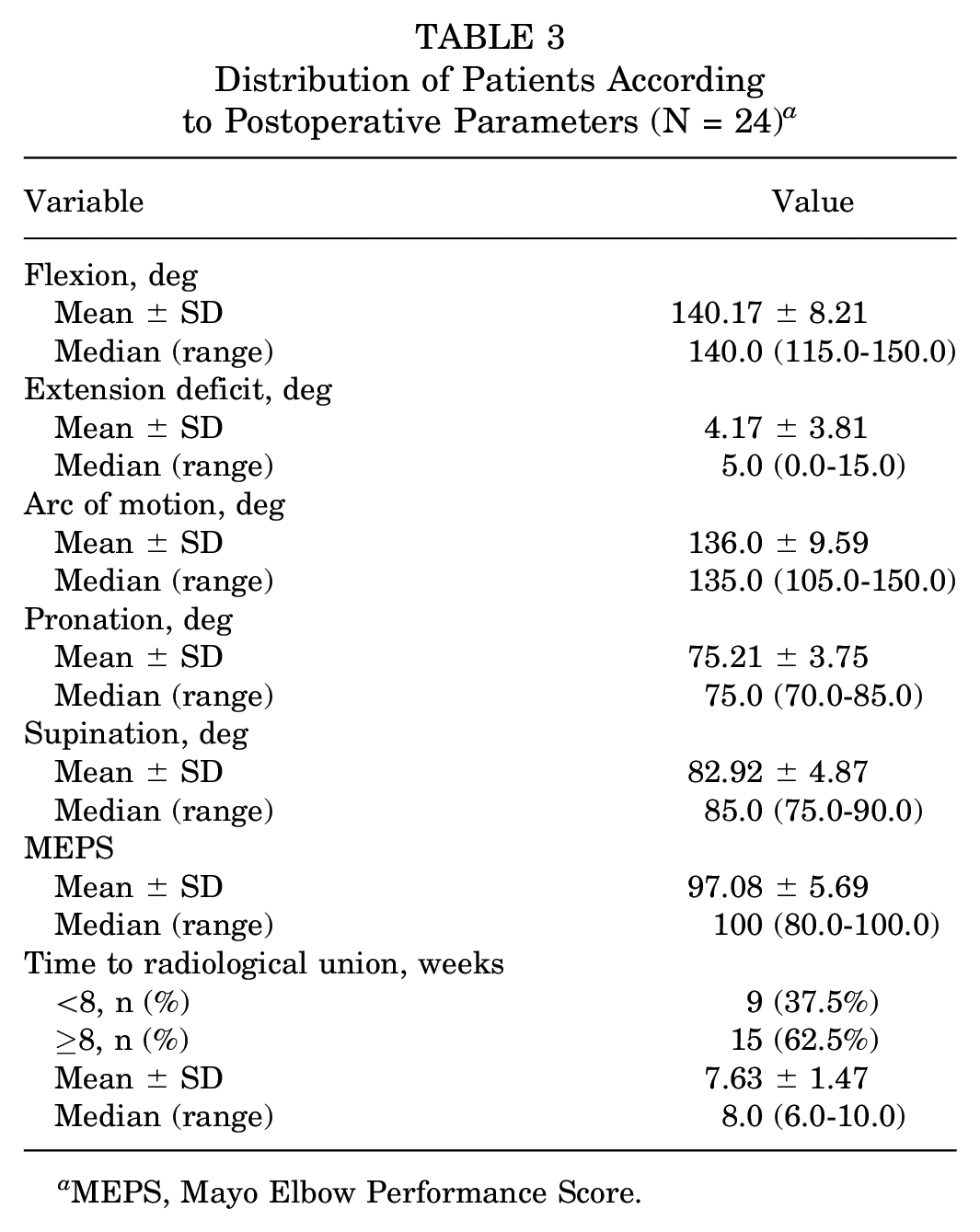
MEPS, Mayo Elbow Performance Score.
Range of Motion
At the end of the follow-up period, the mean elbow flexion was 140.17° (range, 115°-150°), whereas the mean extension deficit was 4.17° (range, 0°-15°). This resulted in a mean arc of motion of 136° (range, 105°-150°). Regarding forearm rotation, the mean pronation was 75.21° (range, 70°-85°), and the mean supination was 82.92° (range, 75°-90°) (Table 3).
Radiological Union
Union as evidenced by radiographs and CT scans was achieved in all of the included patients (Figure 7). The mean time to radiological union was 7.63 weeks (range, 6.0-10.0 weeks).

Case presentation. (A) Preoperative radiographs and CT scans showing the displaced fragment. (B) Postoperative radiographs after fixation with a headless screw. (C) CT scans showing fracture union. CT, computed tomography.
Functional Evaluation
The mean overall MEPS for the cohort was 97.08 (range, 80-100), with 21 excellent and 3 good results. All patients returned to preinjury activities (return to work, daily living and recreational activities) at a mean time of 3.1 months postoperatively (range, 2-6 months).
Concomitant Lesions
An associated capitellum cartilage injury that was not obvious on preoperative radiographs was diagnosed arthroscopically in 1 patient (Figure 8). Debridement of the lesion and removal of small loose cartilage fragments were performed. This patient presented with the lowest MEPS value in our study of 80 (good result) in addition to an arc of motion of 105°.

Arthroscopic view of an associated capitellum cartilage injury (blue asterisk). C, capitellum; R, radial head.
Complications
No patients required any additional procedures, and no neurovascular complications were encountered.
Discussion
The findings of this study confirm the effectiveness of arthroscopic fixation as a noninvasive technique for managing Mason type 2 radial head fractures over a minimum follow-up period of 24 months (range, 24-32 months). Union was achieved in all patients at a mean time of 7.63 weeks (range, 6-10 weeks) postoperatively. Satisfactory clinical and functional outcomes were obtained, with a mean elbow functional arc of motion of 136° as well as a return to preinjury activities after a mean of 3 months. There were 21 patients with excellent results on the MEPS and 3 patients with good results. In addition, no complications were reported.
The decision to surgically manage Mason type 2 fractures is still quite debatable. Yoon et al 41 reported no significant difference in clinical outcomes between ORIF and conservative management. However, they described a number of biases relating to different variables in both study groups. 41 Satisfactory results were reported by Akesson et al 3 in nonoperatively managed Mason type 2 fractures. Nonetheless, 82% of the elbows showed radiographic signs of degeneration. 3 In a retrospective study of the causes of surgical revision of conservatively managed radial head fractures, Nietschke et al 31 recommended fixation of type 2 injuries specifically in young patients owing to the risk of posttraumatic arthritis.
The number of reports on arthroscopic fixation of radial head fractures is quite limited. To our knowledge, this study is the largest prospective case series on arthroscopic fixation of radial head fractures to date. The first report on the technique of arthroscopic fixation of radial head fractures was by Rolla et al 33 in 2006. It included 6 patients, half of whom presented with Mason type 2 fractures. Short-term results were satisfactory, with 50% excellent as well as 50% good MEPS scores. 33 Michels et al 27 described a retrospective series of 14 patients with Mason type 2 fractures managed arthroscopically. Functional evaluation using Broberg and Morrey score revealed 11 excellent and 3 good results. Flexion range was reported as a mean of 142.2° (range, 122°-150°), in addition to a mean extension deficit of 2.8° (range, 0°-10°). 27 In a retrospective series, Wang et al 38 described a technique of arthroscopically fixing Mason type 2 fractures using K-wires, with adequate clinical outcomes. The functional results of these studies are comparable with our findings.27,33,38
Ring et al 32 retrospectively reported the results of ORIF for radial head fractures. Of the included 56 patients, 30 had Mason type 2 injury, of which 16 were isolated. The mean arc of motion was found to be 119° (range, 75°-140°). The mean Broberg and Morrey score was 92 (11 excellent, 17 good, 1 fair, and 1 poor); however, the authors noted that the less satisfactory results were observed in patients with concomitant fractures and dislocation. 32 Lindenhovius et al 23 investigated the long-term follow-up results of ORIF for partial articular fractures in 16 patients and reported a mean MEPS of 89 (range, 55-100) and mean Broberg and Morrey score of 91 (range, 62-100). To our knowledge, a prospective cohort study comparing arthroscopic versus open reduction of radial head fractures has yet to be reported in the literature. Nevertheless, the results of our study, along with the previously reported series on arthroscopic fixation,27,33 demonstrated satisfactory functional outcomes.
Elbow arthroscopy has gained traction as a reliable intervention for the management of different elbow disorders. It is, however, a highly technical procedure that requires adequate knowledge of the neurovascular anatomy of the elbow joint. 18 In contrast to other large joint arthroscopy procedures, it demands a steeper learning curve. 16 Adherence to proper portal placement and appropriate indications can minimize complications,1,18,26 yet the rate of complications of elbow arthroscopy has not been as well established as that of routine arthroscopic procedures.10,11 Giving that it is a joint highly predisposed to developing posttraumatic stiffness, reducing soft tissue dissection, bleeding, and edema is crucial while managing fractures around the elbow. 25 Arthroscopic fixation of fractures can be a minimally invasive option leading to decreased scarring and risk of stiffness. In comparison with open surgery, arthroscopy holds the benefits of better rehabilitation, speedier return to preinjury activities, and reduced postoperative pain.5,16
We utilized the posterolateral portal as the viewing portal, the soft spot (midlateral) as the working portal, and a percutaneous snip for any additional antirotatory, reduction, or reference K-wires. The posterolateral portal provided adequate visualization of the radiocapitellar joint. The decision to fix all fractures via the midlateral portal was made to avoid the potential risk of neurological injury associated with anterior fixation. This all-posterior fixation approach can be quite challenging in some fracture patterns. However, radiographic guidance along with switching the view to the anterior elbow when needed to confirm guide wire location is an effective method to render the technique less demanding. Retrograde, radiographically guided arthroscopic fixation has been similarly described for the fixation of coronoid and capitellum fractures, with satisfactory results.9,36 We used an additional reference radiocapitellar wire in some fractures to help guide the trajectory of the fixating guide wire. This reference K-wire was described as an efficient technique in a cadaveric study by Camenzind et al. 7 The anterolateral portal was used as the working portal by Michels et al, 27 while Rolla et al 33 utilized both the anterolateral and midlateral portals.
All fractures were fixed using a single headless screw in this study. Stability was achieved without the need for adding additional fixation. In previous reports, solely a second screw insertion was required in a few selected cases.27,33 Contrary to the findings of Michels et al, 27 we did not encounter fragments that were deemed too small to withstand a single screw. Arthroscopic K-wire fixation of these fragments were described by Wang et al. 38 Their reported mean time to union (11 weeks), however, was longer than what we observed. Furthermore, because of their fixation choice, the elbow was immobilized in a 90° of flexion brace for 4 to 6 weeks, after which they initiated rehabilitation exercises. 38
The presence of associated capitellum injury with radial head fractures has been reported previously.37,39 We identified a small capitellum cartilage defect, which was debrided along with the excision of intra-articular loose bodies, in 1 patient (4%). Michels et al 27 reported a 14% rate of concomitant capitellum injuries. Comparable with our results, they similarly noted the poorer outcomes associated with these lesions. 27 The presence of concurrent interposed capitellum fragments and radial head fractures was described by Caputo et al 8 in 2006; similar to our patient, Caputo et al 8 did not diagnose this injury pattern initially on radiographic images, including CT scan. Haasters et al 14 further emphasized the diagnostic potentials of arthroscopy in the detection of intra-articular loose bodies associated with radial head fractures. In 60% of the cases, they found an increase in the number of loose bodies identified by arthroscopy compared with CT and magnetic resonance imaging. 14 These reports clearly highlight the advantages of directly visualizing articular surfaces, which is achieved by arthroscopy.
Complications of elbow arthroscopy include elbow stiffness, nerve injury, infection, and heterotopic ossification. 11 The incidence of these complications is not sufficiently well defined in the previous literature.11,21 A recent systematic review and meta-analysis by Ahmed et al 2 reported that elbow stiffness is the most common complication, followed by the need for reoperation after arthroscopy (regardless of indication), then neurological injury. Neurological injury is perhaps one of the most serious complications after elbow arthroscopy. 10 The limited joint space, in addition to the close relation of the capsule to the neurovascular structures, puts all the nerves passing around the elbow, along with their various branches, at risk.10,11,18 Batko et al 4 described precautions to follow for a safer elbow arthroscopy procedure. They reported that proper examination and history taking, in addition to identifying proper indications for arthroscopy, are crucial to prevent complications. Their study emphasized the importance of accurate portal placement, utilizing suitable instruments, and correctly marking anatomic landmarks. 4 Identifying possible risk factors for developing complications after arthroscopy is essential for patient selection.4,11 We did not encounter any neurological complications in this study; however, we excluded 2 patients with a body mass index >30, even though they matched the inclusion criteria. The anatomic landmarks were not easily palpated for safe portal placement; thus, open surgery was considered the safer option. Werner et al 40 reported on the postoperative complication rates of elbow arthroscopy in the obese population, confirming a significant increased risk of all complications, including nerve injury, when compared with nonobese patients.
Limitations
Our study has limitations. The relatively short follow-up period (24-32 months) did not enable us to assess rates of delayed sequelae including radiocapitellar arthritis. Thus, longer follow-up is needed. In addition, this was a single-center prospective case series with no control group for assessing the difference in outcomes compared with ORIF. Further prospective cohort studies with larger sample sizes are required to compare arthroscopic fixation with open surgery.
Conclusion
This study demonstrated that arthroscopic fixation is a valid and valuable technique for managing isolated Mason type 2 radial head fractures. It allowed for accurate reduction without the need for soft tissue dissection, resulting in excellent clinical outcomes.
Footnotes
Appendix
Detailed Patient Data a

| Patient | Age, years | Sex | Side Affected | Arm Dominance | Flexion, deg | Extension Deficit, deg | Arc of Motion, deg | Pronation, deg | Supination, deg | MEPS | Follow-up, months | Time to Radiological Union, weeks |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 29 | M | Right | D | 150 | 0 | 150 | 75 | 85 | 100 | 30 | 6 |
| 2 | 35 | F | Right | D | 145 | 0 | 145 | 75 | 90 | 100 | 29 | 6 |
| 3 | 25 | M | Right | D | 135 | 5 | 130 | 75 | 85 | 100 | 27 | 8 |
| 4 | 52 | M | Left | ND | 140 | 5 | 135 | 80 | 85 | 100 | 28 | 6 |
| 5 | 22 | F | Left | ND | 146 | 0 | 146 | 75 | 85 | 100 | 26 | 6 |
| 6 | 53 | F | Right | D | 145 | 5 | 140 | 70 | 80 | 100 | 24 | 8 |
| 7 | 50 | F | Left | ND | 130 | 0 | 130 | 85 | 90 | 100 | 24 | 8 |
| 8 | 40 | F | Left | ND | 140 | 5 | 135 | 75 | 85 | 100 | 24 | 10 |
| 9 | 53 | F | Left | D | 148 | 5 | 143 | 75 | 85 | 100 | 31 | 8 |
| 10 | 34 | F | Right | D | 145 | 15 | 130 | 75 | 80 | 85 | 26 | 8 |
| 11 | 47 | F | Left | ND | 136 | 5 | 131 | 75 | 85 | 85 | 28 | 6 |
| 12 | 28 | M | Left | ND | 150 | 5 | 145 | 75 | 80 | 100 | 24 | 8 |
| 13 | 38 | F | Right | D | 145 | 10 | 135 | 75 | 80 | 100 | 25 | 10 |
| 14 | 45 | F | Left | D | 140 | 5 | 135 | 70 | 75 | 95 | 32 | 9 |
| 15 | 21 | M | Right | D | 140 | 0 | 140 | 75 | 80 | 100 | 29 | 8 |
| 16 | 19 | M | Right | D | 132 | 5 | 127 | 75 | 75 | 95 | 27 | 6 |
| 17 | 25 | F | Right | D | 135 | 0 | 135 | 70 | 85 | 100 | 30 | 8 |
| 18 | 44 | M | Right | D | 130 | 5 | 125 | 80 | 90 | 100 | 28 | 6 |
| 19 | 31 | F | Left | ND | 135 | 5 | 130 | 70 | 75 | 95 | 32 | 10 |
| 20 | 43 | M | Left | ND | 140 | 0 | 140 | 75 | 85 | 100 | 25 | 10 |
| 21 | 25 | M | Right | D | 149 | 5 | 144 | 80 | 90 | 100 | 29 | 6 |
| 22 | 36 | M | Right | D | 145 | 5 | 140 | 75 | 80 | 100 | 30 | 6 |
| 23 | 37 | M | Left | ND | 148 | 0 | 148 | 80 | 85 | 95 | 27 | 8 |
| 24 | 63 | M | Right | D | 115 | 10 | 105 | 70 | 75 | 80 | 31 | 8 |
D, dominant; F, female; M, male; MEPS, Mayo Elbow Performance Score; ND, nondominant.
Final revision submitted March 26, 2024; accepted April 26, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Alexandria University (reference number 0201625).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.