
Abstract
Background:
Several studies have examined return to play (RTP) and outcomes following the Latarjet procedure in contact athletes.
Purpose:
To investigate clinical outcomes affecting RTP following the Latarjet procedure in contact athletes.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 67 contact athletes (72 shoulders) ≤35 years old who underwent Latarjet procedure for recurrent shoulder instability between January 1, 2018, and March 31, 2022, were retrospectively identified. Demographic information, medical history, surgical history, number of dislocations before surgery, and postoperative complications up to 6 months after surgery were reviewed. Outcomes evaluated included RTP, competition level, satisfaction, and patient-reported outcomes including visual analog scale for pain, American Shoulder and Elbow Surgeons (ASES) Score, and Disabilities of the Arm, Shoulder and Hand (DASH) scores.
Results:
There were a total of 67 patients (72 shoulders) included in the study with a mean age at surgery of 19.7 years for all shoulders. Of the total cohort, 46 patients (50 shoulders; [69.4%]) were available for follow-up by phone. Of the 46 patients contacted by phone, 22/46 were football players; 30/50 [60.0% of all shoulders]) were contact athletes and 19/46 [41.3%] limited contact athletes) were interviewed with a mean follow-up of 25.5 months (range, 10-49 months). Of 72 patients, 22 (30.6% of shoulders and 32.8% of patients) patients had prior shoulder surgery, most commonly arthroscopic stabilization. Only 1 patient experienced hardware failure, but this did not require reoperation. Sixteen of 46 (35%) athletes competed at the collegiate level, and 24/46 (52%) were high school athletes at the time of surgery; 34 of 46 patients (74%) returned to play, of which 30 of the 34 (88%) returned to playing at the same competition level; 15 of 22 (68%) football players returned to play. Only 4 of 51 (8%) reported subjective recurrent instability. Postoperative mean ASES score was 92.2, DASH score was 5.6, and visual analog scale for pain score was 4 (range, 0-50). A total of 43 of 46 (93%) patients reported improvement in quality of life after undergoing the Latarjet procedure for shoulder instability. Eight of 72 (11.1%) shoulders had unresolved pain or stiffness 6 months postoperatively, and 2 of 72 (2.8%) required revisions.
Conclusion:
Patient RTP, outcomes, and satisfaction were high following the Latarjet procedure in young contact athletes.
Shoulder instability is a prevalent pathology in the young, active population.2,19 Researchers have estimated the incidence to be as high as 3% in male athletes who play contact sports. 10 Additionally, the peak age of incidence was found to be between 14 and 19 years of age, which is when many individuals participate in contact sports. 19 Consequently, there has been significant research done to evaluate optimal treatment interventions in this patient population.
The Latarjet procedure uses the technique of removing and transferring a section of the coracoid process to the front of the glenoid to restore stability to the glenohumeral joint. Previous studies have investigated the ability of the Latarjet procedure to treat shoulder instability in young, active patients.4,15,18 The Latarjet procedure has been demonstrated to produce lower Rowe instability scores and to minimize losses in external rotation, but outcomes for the Latarjet procedure following a prior surgery for shoulder instability are mixed.1,4 Several studies to date have investigated return to play (RTP) in contact athletes following the Latarjet procedure.6,12 Previous studies have reported that >85% to 90% of contact athletes are able to return to play 3 to 6 months after undergoing the Latarjet procedure for shoulder instability.3,5 However, there is heterogeneity in the literature about postoperative outcomes in these patients.
The objective of this study was to report RTP in contact or limited contact sport athletes who underwent the Latarjet procedure for shoulder instability. We hypothesized that most patients would achieve significant returns in strength, motion, function, and stability to allow participation in contact sports following surgery.
Methods
After institutional review board approval was obtained, a retrospective review of all patients (n = 67) who underwent Latarjet procedure at a single university institution between January 1, 2018, and March 31, 2022, by 3 fellowship-trained shoulder surgeons (R.C.R., G.L.C., J.Y.B.) was conducted. Study inclusion criteria were patients who were ≤35 years old, playing a contact or limited contact sport before surgery, and English speaking. Contact sports were defined according to the American Academy of Pediatrics: ice hockey, football, basketball, skiing/snowboarding, soccer, wrestling, rugby, martial arts, lacrosse, ultimate frisbee, boxing, and diving; limited contact sports included volleyball, surfing, softball, baseball, floor hockey, and bicycling. 7 Exclusion criteria were patients who received an allograft bone block or had a history of seizure.
Demographic data were collected from the patient medical record and included age at time of surgery, sex, primary sport played, prior shoulder surgery, subjective shoulder dislocations before surgery, surgical indication, and procedure. Postoperative complications occurring up to 6 months after surgery were recorded, including graft or hardware failure, vascular injury, nerve (musculocutaneous, axillary, or suprascapular) injury, recurrent instability, additional shoulder surgery, infection, reoperation, wound dehiscence, hematoma formation, complex regional pain syndrome, nonunion, and ulnar neuritis.
All eligible patients were contacted for a telephone interview by 2 researchers (M.S. and A.P.). A standardized script was used to explain the purpose and confidential nature of the study to each contacted patient. Patients who were willing to participate provided consent over the telephone; for patients aged <18 years, a parent or guardian was contacted and provided consent first. Only patients who completed the patient-reported outcomes (PROs) and novel RTP questionnaire (Supplemental Figure S1, available online) were included in the telephone cohort. A total of 46 patients (50/72 shoulders; 69.4%) were successfully interviewed with a mean follow-up of 25.5 months (range, 10-49 months).
The novel questionnaire assessed RTP, which was defined as whether patients returned to participating in sports. Data gathered by the questionnaire included the contact or limited contact sports played by the patient; preoperative competition level (high school, collegiate, semiprofessional, or professional); RTP; further instances of instability, subluxation, or dislocation; and quality of life after undergoing the Latarjet procedure. RTP was further delineated by whether the patient returned to his or her preoperative level of sport. Reasons for not returning to play or returning to play but not at the same level were assessed; answer choices provided to patients included restrictions placed by their surgeon, aging out, fear of further injury from the sport played, shoulder apprehension, recurrent dislocation, and any other reason not listed above. Patients were allowed to select multiple reasons as to why they did not RTP. The date of interview was compared with the date of surgery to determine follow-up. PROs including the American Shoulder and Elbow Surgeons (ASES) score, Disabilities of the Arm, Shoulder and Hand (DASH) score, visual analog scale (VAS) for pain (0-10), and Single Assessment Numeric Evaluation were also assessed over the telephone.
Descriptive statistics were generated for the entire cohort of eligible patients and the cohort of patients who participated in the telephone interview. RTP by competition level and whether Latarjet was a primary versus revision surgery were assessed. Preoperative glenoid bone loss (in mm) was compared between patients who returned to play and those who did not. Glenoid bone loss was measured using the perfect circle method on preoperative computed tomography scan. Hill-Sachs measurement is given as a width, as in the glenoid track measurement calculation. Selection bias was minimized by enrolling a consecutive series of eligible patients. Continuous variables were analyzed via t test, and categorical variables were analyzed via chi-square test. All statistical tests were 2-sided and considered significant at P < .05. Analyses were conducted using Stata/SE Version 17.0 (StataCorp).
Results
A total of 67 patients (72 discrete shoulders) were eligible as young contact athletes who underwent the Latarjet procedure in the study period. The mean age of the cohort was 19.7 years (range, 14-28 years). Of the 72 shoulders, 22 (30.6%) had ≥1 arthroscopic procedure with labral repair before undergoing the Latarjet procedure. Complications in the 6 months after surgery were relatively infrequent.
A total of 46 patients (50 shoulders) were interviewed over the telephone, yielding a follow-up rate of 68.7% with a mean follow-up of 25.5 months (range, 10-49 months). The majority, 52% (24/46 patients), of the interviewed cohort played at the high school level at the time of surgery (Table 1). Of the remaining patients, 35% (16 of 46) played at the collegiate level and 13% (6 of 46) recreationally. No professional athletes were interviewed. The most played sport was football, with 22 patients indicating that this was the primary sport they played at time of surgery. Five patients played ice hockey, 15 basketball, 1 skiing/snowboarding, 3 soccer, 4 lacrosse, 12 wrestling, and 19 (41.3%) played a limited contact sport. Of note, patients could choose multiple sports.
Descriptive Patient Data (N = 46) a

Mean follow-up was 25.5 months. Dashes indicate not applicable.
Multiple options could be chosen by interviewees.
Of the total patients interviewed, 74% (34/46) returned to play, of which 88% (30/34) returned to playing at the same level; 47% (16/34) of patients who returned to play were still playing a contact sport at time of interview. Of those who did not RTP, 11 patients cited aging out of their preoperative competition level as a reason, 10 had fear of further shoulder injury, 3 had subjective shoulder apprehension, and 1 had recurrent dislocation preventing a return to play. Patients could choose multiple reasons for not returning to play. Patients returned to play at significantly higher rates following the index Latarjet procedure compared with revision Latarjet (P = .01) (Table 2). However, patients with index Latarjet procedure were likely to RTP at a the same competition level (P = .82) (Table 3). Rates at which athletes returned to play were not significant (P = .2) when analyzed by competition level, nor was whether patients returned to playing at the same or lower competition level (P = .39) (Tables 4 and 5).
Return to Play Based on Primary Latarjet Versus Revision Latarjet Surgery a
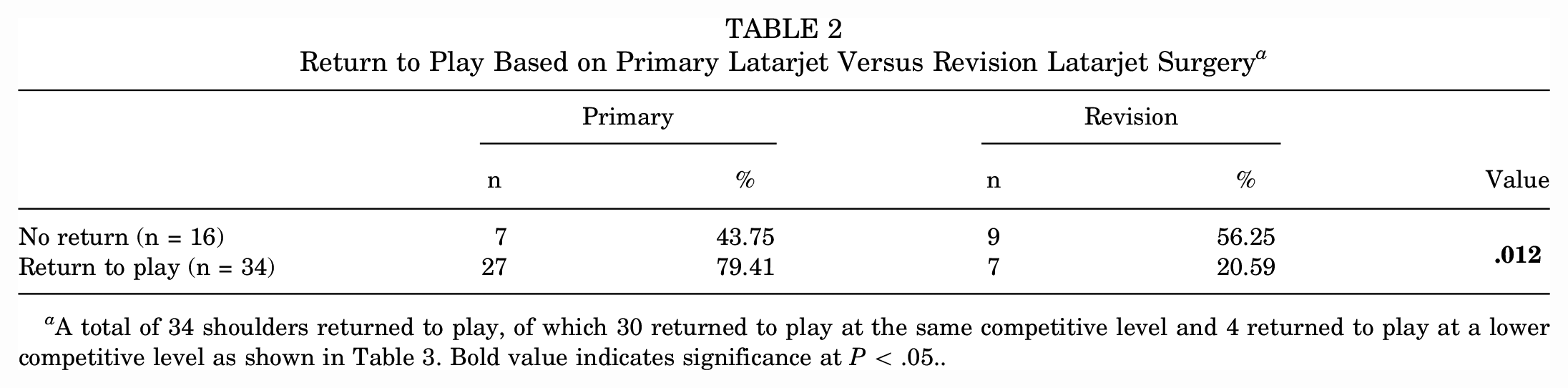
A total of 34 shoulders returned to play, of which 30 returned to play at the same competitive level and 4 returned to play at a lower competitive level as shown in Table 3. Bold value indicates significance at P < .05..
Level of Return to Play Based on Primary Latarjet Versus Revision Latarjet Surgery

Return to Play Based on Competition Level a

Reporting RTP based on total shoulders. 4 athletes had bilateral (total of 50 shoulders).
2 of the high school athletes had bilateral surgeries, accounting for 26 total shoulders.
2 of the college athletes had bilateral surgeries, accounting for 18 total shoulders.
Return to Play Based on Same or Lower Competition Level

There was no significant difference in the amount of preoperative glenoid bone loss between patients who returned to play and those who did not (P = .90) (Table 6). In the RTP cohort, the mean bone loss was 4.6 ± 2.1 mm (n = 14) and 4.7 ± 2.0 mm in the failure to RTP cohort (n = 28) (P = .90). There was no significant difference in preoperative glenoid bone loss when stratified by RTP at the same or lower level. The mean glenoid bone loss was 4.0 ± 2.3 mm in the RTP at the lower-level cohort and 4.7 ± 2.2 mm in the RTP at the same level cohort (P = .54). There were statistically significant differences in postoperative ASES and DASH scores when stratified by primary Latarjet or revision Latarjet following a failed prior arthroscopic stabilization, though these differences were below the minimal clinically important difference for the Latarjet procedure. The mean postoperative ASES score was 94.4 ± 9.4 in the primary Latarjet group and 87.7 ± 12.6 in the revision cohort (P = .04). The mean postoperative DASH score was 4.3 ± 4.7 in the primary Latarjet group and 8.3 ± 7.2 in the revision cohort (P = .02).
Outcomes Stratified by Primary Versus Revision Latarjet and Return to Play Versus No Return to Play in Contact Athletes a

Bold values indicate significance at P < .05.. ASES, American Shoulder and Elbow Surgeons; DASH, Disabilities of the Arm, Shoulder and Hand.
A total of 8% of the shoulders (4 of 50) had subjective recurrent instability after undergoing Latarjet procedure; of these, 1 patient had frank instability and required revision surgery with distal tibial autograft 3.25 years after index surgery. None of these 4 patients returned to play. The 1 patient with frank instability did RTP after index surgery but not after revision surgery. Four percent (2 of 50 shoulders) required reoperation following Latarjet. Most significantly, 93% of patients (43 of 46) reported an improvement in quality of life after undergoing the Latarjet procedure. The mean ASES score was 92.2 (range, 65-100) and DASH score was 5.6 (range, 0-24.2). Mean VAS for pain score was 4 (range, 0-50).
Overall complication rate was 2.8% (2/72) in the first 6 months, and overall return to the operating room was 2.8% (2/72); there was 1 case of hardware failure, which did not require subsequent surgery; 2 patients required reoperation, with 1 hematoma evacuation in the initial 6-month period. Of the 50 shoulders in patients who participated in the telephone survey at a mean of 25.5 months after surgery, there was 1 revision Latarjet procedure (open reduction internal fixation) performed at another institution 3.25 years after the index Latarjet. The patient who underwent revision Latarjet surgery was able to return to play 9 months after the index Latarjet and was able to play contact sports for 2.5 years before the revision procedure. Eight shoulders (11%) had self-reported unresolved pain or stiffness 6 months following surgery.
Discussion
In this study, we used a survey to investigate factors affecting the ability of young athletes to return to play following the Latarjet procedure. There is conflicting literature to date regarding the efficacy of the Latarjet procedure in allowing contact athletes to resume their previous levels of activity. Previous investigations have reported that 70% to 90% of athletes return to contact sports within 6 to 9 months of this surgery.6,11,17 However, other studies have found that these patients are not able to resume contact sports due to persistent stiffness and loss of full strength and range of motion.9,11 The current study reinforced the previously reported high rate of RTP following the Latarjet procedure and further delineated whether RTP is affected by competition level, primary versus revision surgery, and bone loss.
Previous studies have reported on the ability of the Latarjet procedure to enable RTP in contact athletes. In a systematic review, Hurley et al 12 reported that 88.2% of collision athletes returned to sports with 69.5% returning to the same level as before by final follow-up. Similarly, Bohu et al 6 reported that 73% of 217 patients were able to return to play within 8 months of the Latarjet procedure. Ernat et al 8 found that 97% of 89 patients resumed sports, while 74% were able to return at the same level as or similar level to that before the injury. Our findings are in agreement with the prior literature. In this study, 76% of patients (35/46) returned to play, and of the patients to return to contact sports, 88% (30/34) of those returned to playing at the same level. It is important to note that 26% of patients did not RTP and that 35% of patients did not RTP at the same level. It is imperative to provide this information to patients preoperatively when counseling about the benefits and risks of the Latarjet procedure. Overall, this reinforces the previously well-demonstrated finding that the Latarjet procedure is an excellent option for contact athletes with glenohumeral instability. Additionally, we sought to investigate factors that inhibited athletes from returning to play, which we will discuss below.
In our patient population, roughly 24% (11/46) of patients did not return to playing contact sports following the Latarjet surgery. Several factors that may have contributed to this finding include high school students had graduated by the time they recovered from the Latarjet surgery, as well as fear of further shoulder injury and subjective shoulder apprehension, which was reported by 10 of 11 patients who did not RTP. While researchers have investigated reasons for failure to RTP, they have focused on reasons such as persistent stiffness, weakness, and inadequate range of motion following surgery. 9 In a similar study, Hurley et al 11 found that the most common reasons for not returning to play were persistent pain, graduating from their level of competition, and shoulder apprehension. Thus, our findings seem to follow what has been previously reported by Hurley et al. 11 The lack of RTP in our cohort can be divided into 2 categories: graduating from level of competition and shoulder-specific apprehension. The former category may consist of patients who could have returned to sports, while the latter group represents a true failure to return to play. Further research should be done in patients who graduated from their level of competition to see if they would be able to participate in contact sports following the Latarjet procedure.
There were significant differences in RTP outcomes based on whether the Latarjet was an index or revision surgery following a failed arthroscopic stabilization. In our study, there was a significantly higher RTP rate in patients with index Latarjet (P = .01), but they were also likely to return at the same level of competition (P = .82). In a series of 73 patients, Privitera et al 16 also reported that patients with >2 prior arthroscopic stabilizations had lower rates of RTP following the Latarjet procedure and that preoperative glenoid bone loss had no bearing on RTP outcomes; both of these were consistent with the findings of the current study. In contrast, Kee et al 13 found that there was no significant difference in RTP outcomes when comparing patients with index (n = 14) versus revision (n = 42) Latarjet. However, Kee et al did not specify RTP by level of competition in their study. Our results support performing a definitive stabilization procedure and minimizing as much as possible the risk of needing a revision surgery. The risks of an unsuccessful arthroscopic procedure, which may necessitate a second surgery, include additional joint damage, requiring a second recovery period, downtime from sport, and additional scar tissue. It is notable that patients returned to the same competition level after a primary Latarjet procedure compared with a revision. We hypothesized that patients at the higher echelon of their competitive sport are more likely to RTP and also experience a recurrence in injury. Additionally, there are many factors outside of the actual surgery itself that can affect this, and further investigation is warranted before ascertaining clinical applicability.
PROs are a valuable metric in assessing shoulder function in patients with Latarjet. While some patients may not return to contact sports, the PROs provide information about shoulder utility. In a study specific to the Latarjet procedure, Menendez et al 14 found the Patient Acceptable Symptom State for ASES and VAS to be 86.0 and 2.5, respectively. In a midterm follow-up study, Belangero et al 4 reported that the mean ASES was 85 at 2 years and 83 at 5 years postoperatively. Similarly, our patients had a mean postoperative ASES score of 92.2 and mean VAS score of 4. Thus, our patients had a mean ASES score above the passable acceptable clinical state but their pain levels were slightly above the Patient Acceptable Symptom State value. This demonstrates that contact athletes may have excellent shoulder function despite residual pain following the Latarjet procedure.
This study has some limitations. Due to the retrospective nature of this study, there was some inherent selection bias built into the cohort. Additionally, we were only able to reach 68.7% of our eligible cohort, and it is possible that the remaining 30% may have skewed the results in a different direction. Additionally, about half of patients who did not RTP had graduated from high school, thus limiting our ability to investigate the true ability of the Latarjet procedure to allow patients to functionally return to contact sports. This study was also unable to assess RTP in professional athletes, who are a valuable demographic for the study of shoulder stabilization surgeries. We also included individuals who played limited contact sports, not just collision athletes. Future directions should include a prospective evaluation of a large population of young, contact-sport athletes undergoing the Latarjet procedure to further assess clinical factors that affect RTP at greater competition levels.
Conclusion
The Latarjet procedure is a safe and effective option for contact athletes with glenohumeral instability. In this study, 74% of our patients were able to return to contact play; furthermore, many reported no dislocations or subluxations following surgery. Most importantly, 93% of patients reported an improvement in quality of life after undergoing the Latarjet procedure. Thus, the Latarjet procedure should continue to be an excellent option for treating the high-impact contact athlete with shoulder instability.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241265029 – Supplemental material for Clinical Outcomes Affecting Return to Play Following Latarjet Procedure in Young Contact and Limited Contact Athletes
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241265029 for Clinical Outcomes Affecting Return to Play Following Latarjet Procedure in Young Contact and Limited Contact Athletes by Mathangi Sridharan, Akshar Patel, Erryk Katayama, Dane Swinehart, Ryan C. Rauck, Gregory L. Cvetanovich and Julie Y. Bishop in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted February 9, 2024; accepted February 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.S. has received education payments from Smith+ Nephew, Gemini Mountain Medical LLC, and CDC Medical LLC. R.C.R. has received compensation for services other than consulting from Arthrex and education payments from CDC Medical LLC. G.L.C. has received compensation for services other than consulting and travel payments from Smith+ Nephew and education payments from CDC Medical LLC. J.Y.B. has received consulting and travel payments from Stryker, consulting fees from Linvatec Corporation, and payments for services other than consulting from Smith+ Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Ohio State University (ref No. 2021H0367).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.