
Abstract
Background:
Little is known regarding the opinions of the general population on anterior cruciate ligament (ACL) graft options.
Purpose:
To evaluate the general population's perception of the use of allografts versus autografts in ACL reconstruction using a previously validated online marketplace platform.
Methods:
A prospective 34-question survey was distributed via the online marketplace. After collecting baseline demographics, participant preferences for ACL reconstruction with an allograft or autograft were established. All respondents completed a preeducation survey, reviewed an evidence-based education sheet, and completed a posteducation survey to assess their understanding. Upon completion, participants were asked which graft they would prefer. Participants were then asked if they would be willing to change their preference based on surgeon recommendation. Finally, participants were asked to rank the factors from the education sheet that were most influential.
Study Design:
Cross-sectional study.
Results:
There were 491 participants that completed the survey (mean age, 39.9 years [range, 19-72 years]; 244 male, 241 female, and 6 nonbinary/third-gender participants). Before reading the education sheet, 276 (56%) reported no graft preferences, 146 (30%) preferred autograft, and 69 (14%) preferred allograft. After reading the provided sheet, 226 (46%) participants preferred autograft, 185 (38%) preferred allograft, and 80 (16%) had no preference. The mean score on the preeducation test was 45%, and the mean score on the posteducation test was significantly greater (61%; P < .01). Overall, 345 participants (83.9%) stated they would change their preference for autograft or allograft if their surgeon recommended it. Surgeon preference (n = 330; 67%), educational information provided (n = 117; 24%), and previous knowledge (n = 44; 9%) were the most important factors for making graft selections. The mean ages of the participants selecting each graft type before and after education were as follows: allograft (37.8 ± 10.1 vs 40.6 ± 11.8 years; P = .05), autograft (38 ± 11.5 vs 39.5 ± 10.1 years; P = .21), and no preference (41.5 ± 11.2 vs 39.4 ± 11.8 years; P = .16).
Conclusion:
Education resulted in a greater number of individuals’ reporting a preference in graft type (either allograft or autograft) compared with preinformation questioning. In addition, 83.9% of the participants were willing to switch their graft choice if recommended by their surgeon.
Keywords
Anterior cruciate ligament (ACL) tears are one of the most common orthopaedic injuries with a reported annual incidence of 68.6 per 100,000 person-years. 23 The number of ACL reconstructions has increased significantly over the past 2 decades.1,4,16 Advancement in ACL research has helped surgeons develop a variety of reconstruction graft options, including both autograft and allograft options. 14
Autografts are those that come from the patient and are typically the preferred choice in the young, athletic patient due to lower rates of failure and risk of repeat rupture. 27 However, autografts are also associated with donor-site morbidities such as patellar fracture, anterior knee pain, graft mismatch, flexion weakness, and inability to utilize certain autografts in skeletally immature patients, among others.5,9,15 Allografts have the advantages of no donor-site morbidity, faster initial recovery, faster operative times, and size-specific matching. 12 Conversely, allograft availability, maximal tensile strength, and infection have all been identified as weaknesses in the use of allograft in ACL reconstruction.
While multiple comparative studies looking at patient outcomes after allograft and autograft ACL reconstruction have been performed, we are not aware of any studies that consider the opinions of the general population on ACL graft options. Amazon Mechanical Turk (MTurk; Amazon Web Services), an online crowdsourcing platform that allows businesses and researchers access to a broad population with a variety of backgrounds, has been utilized in the recent orthopaedic literature to gauge patient expectations and public perceptions.8,20,21 This tool has been shown to have strong internal consistencies and test-retest reliability compared with more conventional survey techniques. Additionally, it has been shown to provide accurate generalizability to the US population.6,8,18,22
In the current study, we used MTurk to evaluate the general population's perception of the use of allografts and autografts in ACL reconstruction. The null hypothesis was that there would be no difference in patient preference between allograft and autograft use in ACL reconstruction.
Methods
For this study, we crowdsourced the participation in our custom survey to registered users on the MTurk platform. Unique survey completion codes are generated through the platform once participants have finished a survey, allowing for verification of completion followed by compensation. This process ensures high-fidelity responses from the participants. We recruited adult participants ≥18 years of age and those residing in the United States. Respondents were paid $1.50 for completion. Incomplete surveys or those with a duplicate internet protocol address were omitted. Institutional review board approval was not sought, as this study was considered exempt from review.
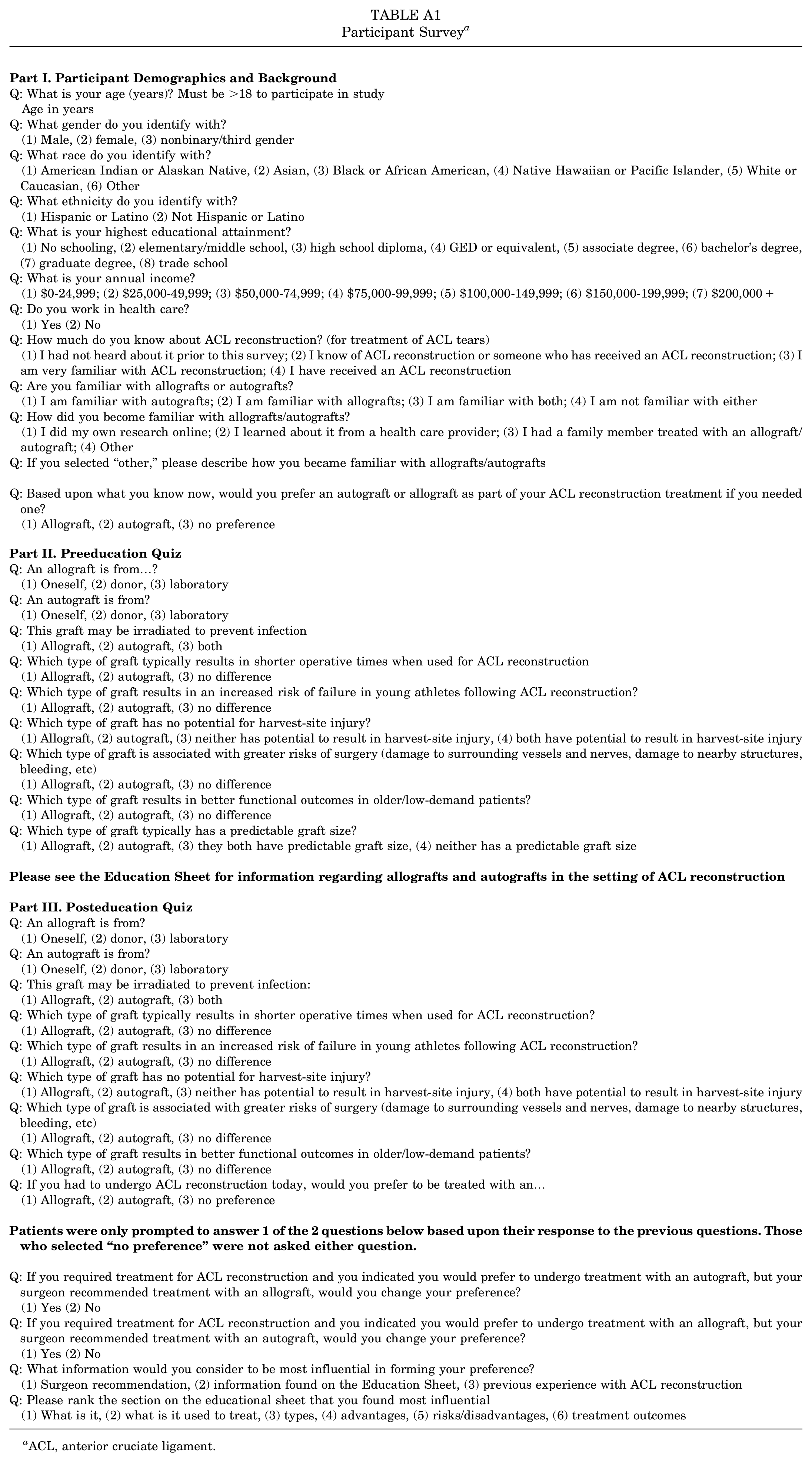
The survey included 34 questions designed to identify participant demographics, factors perceived to potentially influence their opinions, and baseline knowledge about ACL reconstruction (Appendix Table A1). Included was a preeducation section regarding knowledge of graft preferences. Participants were subsequently provided with an evidence-based education sheet highlighting some of the integral differences between autograft and allograft (Figure 1). The participants were then asked the same questions from the preeducation section in a posteducation section; the aim of this portion of the survey was to ensure that participants read/understood the information provided. Finally, participants were asked about their willingness to change their opinions and the factors that were most influential in their decision-making process.
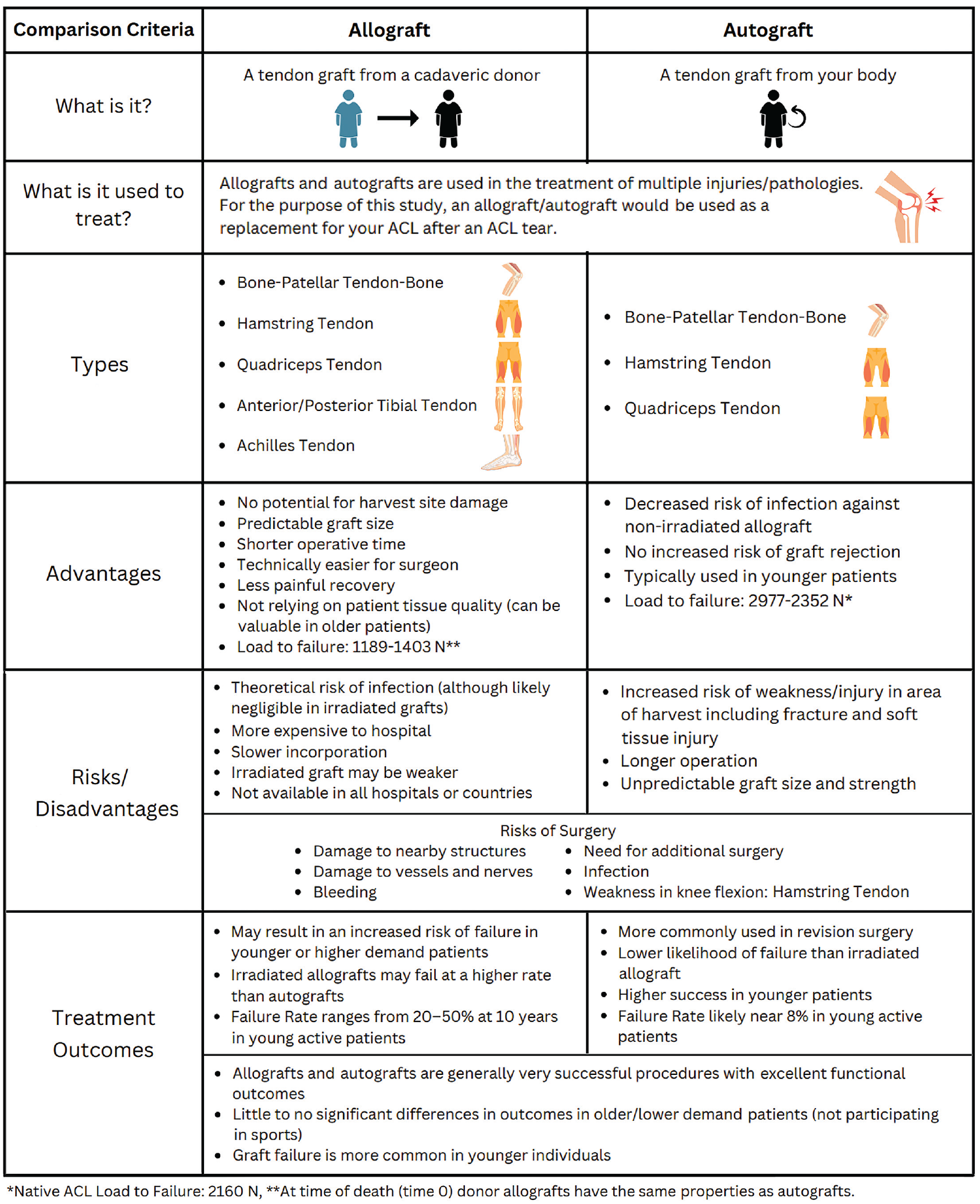
Evidence-based education sheet provided to the study participants between the preeducation and posteducation portions of the survey.
Statistical Analysis
Descriptive statistics were calculated for all included patients using the open-source R software (Version 2.14.1; The R Project for Statistical Computing). The distribution of data points was analyzed with the Shapiro-Wilks test. Student paired t tests were used to compare pre- and posteducation test scores. The chi-square test was used to analyze the significance of sex and graft selection. P values ≤.05 were deemed to be statistically significant.
Results
A total of 491 participants completed the survey. There were 244 (49.7%) male, 241 (49.1%) female, and 6 (1.2%) nonbinary/third-gender participants. The mean age of the respondents was 39.9 ± 11.3 years (range, 19-72 years). The most frequently reported races were 388 (79%) White or Caucasian, 54 (11.0%) Black or African American, and 33 (6.7%) Asian. Regarding level of education, 362 (73.7%) participants reported that they earned at least a bachelor's degree. Additionally, 362 (73.7%) participants reported that they did not work in health care.
In total, 272 participants reported not being familiar with either allografts or autografts before taking the survey. Of the participants who were familiar with either or both grafts before the survey, 20.5% (n = 45) learned about them independently, 41.1% (n = 90) learned about them from a health care provider, and 32.9% learned about them from a family member's treatment.
The mean score on the preeducation test was 45%, and the mean score on the posteducation test was significantly greater, at 61% (P < .01). Before reading the education sheet, 14.1% of the participants (n = 69) preferred an allograft, 29.7% (n = 146) preferred autograft, and 56.2% (n = 276) had no preference. After reading the education sheet, 46% of the respondents (n = 226) reported that they preferred autograft, 37.7% (n = 185) preferred allograft, and 16.3% (n = 80) had no preference. A significantly greater percentage of participants preferred autograft after education compared with the number who preferred autograft before education (P < .01). Similarly, a significantly greater percentage of participants preferred allograft after education (P < .01). Overall, more participants reported a preference for either allograft or autograft after education versus the number of participants who preferred either allograft or autograft before education (Table 1).
Patient Preferences for Graft Types Before and After Reading the Education Sheet a

Data are presented as n.
The respondent's sex did not appear to have any influence in graft selection choice. Of the 244 self-reported male participants, initially 65 (26.6%) preferred autograft, 37 (15.2%) preferred allograft while 142 (58.2%) had no preference. After education, 106 (43.4%) preferred autograft, 93 (38.1%) preferred allograft, and 45 (18.4%) still had no preference. Self-reported female participants followed a similar pattern of pre-/posteducation preferences. Of the 241 self-reported women, 79 (32.8%) preferred autograft, 32 (13.3%) preferred allograft, and 130 (54%) had no preference before reading the education sheet. After education, 116 (48%) preferred autograft, 91 (37.8%) preferred allograft, and 34 (14.1%) still had no preference. There were no significant differences between autograft or allograft preferences between male and female participants when preeducation (P = .33) and posteducation (P = .37) preferences were analyzed.
Among the 226 patients who preferred autograft after education, 80.5% (n = 182) reported that they would be willing to undergo treatment with an allograft if their surgeon recommended it. Similarly, among the 185 participants who reported a preference of allograft, 88.1% (n = 163) reported that they would undergo treatment with an autograft if their surgeon recommended it. In total, 345 patients (83.9%) stated they would change their preference for autograft or allograft if their surgeon recommended the other.
Surgeon preference (n = 330; 67%) was found to be the most important factor in formulating participant preference, followed by the information provided on the education sheet (n = 117; 24%) and previous knowledge (n = 44; 9%). In terms of information from the education sheet that influenced their decision for graft type, the description of what the graft is (n = 127) was most frequently identified as being the most influential, followed by risks/advantages (n = 124), then treatment outcomes (n = 103). The mean ages of participants selecting each graft type before and after education were 37.8 ± 10.1 versus 40.6 ± 11.8 years for those selecting allograft (P = .05), 38 ± 11.5 versus 39.5 ± 10.1 years for autograft (P = .21), and 41.5 ± 11.2 versus 39.4 ± 11.8 years for those with no preference (P = .16).
Discussion
The primary findings of this study were that after providing an informational education sheet, the majority of participants formulated their own preferences with respect to allograft or autograft in ACL reconstruction. Furthermore, a vast majority of patients admitted that they would be willing to undergo surgery with the other graft option if their surgeon recommended it. This information is easily transferable to the general patient population of a knee surgeon, as these data were collected from a crowdsourced survey. Surgeons can use this information to understand the importance of providing details about graft types to patients before ACL reconstruction and appreciate that patients are able to formulate opinions based upon clinical and biomechanical data about different graft types.
Before reading the evidence-based education sheet (Figure 1), a majority of the participants reported no preference in graft type; however, after reading the education sheet, the number of participants with a preference (either autograft or allograft) increased significantly. In fact, the number of participants that preferred both autograft and allograft increased significantly. As patient activation becomes the emphasis in health care, it becomes more evident that patients are able and willing to make decisions when informed about a topic. 10 A 2010 study found that patients who derived a majority of their understanding of ACL graft types from the internet chose allografts at a significantly higher rate. 13 Understanding the inherent financial biases of publicly available sources toward allograft is essential in order to engage in productive dialogue with patients. Moreover, a recent study that surveyed young patients undergoing shoulder arthroscopy found that those that self-reported as athletes preferred patellar tendon autograft over allograft. 25 Clinicians should work to educate their patients in an unbiased, evidence-based manner about graft options as much as possible prior to engagement in discussions about what is best for their individual case. It is well known that patient expectations have an impact on patient satisfaction after ACL reconstruction.7,24 It is reasonable to assume that participating in shared decisionmaking and providing an unbiased and evidence-based education may assist surgeons in setting clear expectations for their patients.
An additional finding was that the majority of patients (84%) would be willing to switch their graft choice if recommended by their surgeon. A previous case-control study by Koh et al 13 on a cohort of patients undergoing ACL reconstruction found that surgeon explanation was the most important factor in affecting a patient's final decision about ACL graft type, while information derived through internet searches was the second most important factor. A 2005 study of 202 patients discussing invasive procedures found that the majority of patients reported that clinician opinion was the most influential factor. 17 This finding was further amplified in older patients. 17 The literature also demonstrates that clinicians’ graft choices are founded in evidence.3,19 Previous survey studies among surgeons have reported that patient age was the most important factor for surgeon preference, with patellar tendon and quadriceps tendon autografts being the preferred graft for younger athletes. 3 Fellowship training was also correlated with graft preferences. 27 These conclusions support the findings of the current study and emphasize the integral role that the surgeon has and the trust that patients place in allowing surgeons to guide ACL graft selection.
The current study found that the mean age of the participants who preferred an allograft was significantly older after education compared with the patients that preferred allograft before education. While we acknowledge that this difference may be due to information in the education sheet, such as “Not relying on patient tissue quality (can be valuable in older patients),” the sheet was formulated with evidence-based information.2,26 Additionally, this finding alludes to the fact that participants were able to engage with and interpret impactful information from the education sheet. This observation is further supported by the fact that posteducation quiz scores were significantly higher than preeducation quiz scores.
MTurk has been shown to be a valuable tool for crowdsourcing in the recent orthopaedic literature.8,21 Puzzitiello et al 21 used MTurk to report that surgeon professionalism/personality and quality of facilities were the most important factors in selecting a sports surgeon. Hafen et al 11 used MTurk to show that patients prefer navigation or robot-assisted total knee arthroplasty compared with manual or conventional total knee arthroplasty techniques. These studies allow clinicians and researchers access to a large number of people that accurately represent the general population as a whole. 18 Understanding consumer/patient preferences can help guide treatment plan discussions as well as marketing decisions in an ever-evolving world of cost-focused medicine.
Limitations
We acknowledge that this study was not without limitations. While the education sheet was based on objective data, it is not a complete resource. We felt that it was integral to make the sheet concise, which meant omitting certain data. It is important to note that the results proved that the provided sheet was successful at educating the participants, as was evidenced by the improved scores on the posteducation portion of the quiz. While we acknowledge that the mean score remained relatively low even after education (61%), we believe that this is likely a combination of the complexity of the topic and participants’ likely not understanding the information. Furthermore, the purpose of this study was not to validate a clinical decision tool. Rather, the purpose was to assess the general public's perspective on ACL reconstruction and better understand factors that influence such perspectives. Another potential concern that may be shared among orthopaedic surgeons is that health care decisions should not be made based on the whims of the patient alone. While this is a valid concern, it is well understood that expectations may influence outcomes. Providing a nonbiased education may not only build trust with patients but also set clear expectations. In addition, the results indicate that patients hold surgeon opinion in high regard and may be influenced based on surgeon recommendation. A final limitation is the selection bias incurred through the crowdsource study design. Our participants represent a general US population, which may not accurately represent the typical patient being evaluated at a sports medicine clinic with an ACL injury.
Conclusion
The informational education sheet was found to be successful at improving participant knowledge. Furthermore, education resulted in a greater number of individuals reporting a preference in graft type (either allograft or autograft) compared with preeducation questioning; however, the majority of individuals indicated they would alter their preference based on surgeon recommendation.
Footnotes
Appendix
Participant Survey a
|
|
| Q: What is your age (years)? Must be >18 to participate in study |
| Age in years |
| Q: What gender do you identify with? |
| (1) Male, (2) female, (3) nonbinary/third gender |
| Q: What race do you identify with? |
| (1) American Indian or Alaskan Native, (2) Asian, (3) Black or African American, (4) Native Hawaiian or Pacific Islander, (5) White or Caucasian, (6) Other |
| Q: What ethnicity do you identify with? |
| (1) Hispanic or Latino (2) Not Hispanic or Latino |
| Q: What is your highest educational attainment? |
| (1) No schooling, (2) elementary/middle school, (3) high school diploma, (4) GED or equivalent, (5) associate degree, (6) bachelor's degree, (7) graduate degree, (8) trade school |
| Q: What is your annual income? |
| (1) $0-24,999; (2) $25,000-49,999; (3) $50,000-74,999; (4) $75,000-99,999; (5) $100,000-149,999; (6) $150,000-199,999; (7) $200,000+ |
| Q: Do you work in health care? |
| (1) Yes (2) No |
| Q: How much do you know about ACL reconstruction? (for treatment of ACL tears) |
| (1) I had not heard about it prior to this survey; (2) I know of ACL reconstruction or someone who has received an ACL reconstruction; (3) I am very familiar with ACL reconstruction; (4) I have received an ACL reconstruction |
| Q: Are you familiar with allografts or autografts? |
| (1) I am familiar with autografts; (2) I am familiar with allografts; (3) I am familiar with both; (4) I am not familiar with either |
| Q: How did you become familiar with allografts/autografts? |
| (1) I did my own research online; (2) I learned about it from a health care provider; (3) I had a family member treated with an allograft/autograft; (4) Other |
| Q: If you selected “other,” please describe how you became familiar with allografts/autografts |
| Q: Based upon what you know now, would you prefer an autograft or allograft as part of your ACL reconstruction treatment if you needed one? |
| (1) Allograft, (2) autograft, (3) no preference |
|
|
| Q: An allograft is from…? |
| (1) Oneself, (2) donor, (3) laboratory |
| Q: An autograft is from? |
| (1) Oneself, (2) donor, (3) laboratory |
| Q: This graft may be irradiated to prevent infection |
| (1) Allograft, (2) autograft, (3) both |
| Q: Which type of graft typically results in shorter operative times when used for ACL reconstruction |
| (1) Allograft, (2) autograft, (3) no difference |
| Q: Which type of graft results in an increased risk of failure in young athletes following ACL reconstruction? |
| (1) Allograft, (2) autograft, (3) no difference |
| Q: Which type of graft has no potential for harvest-site injury? |
| (1) Allograft, (2) autograft, (3) neither has potential to result in harvest-site injury, (4) both have potential to result in harvest-site injury |
| Q: Which type of graft is associated with greater risks of surgery (damage to surrounding vessels and nerves, damage to nearby structures, bleeding, etc) |
| (1) Allograft, (2) autograft, (3) no difference |
| Q: Which type of graft results in better functional outcomes in older/low-demand patients? |
| (1) Allograft, (2) autograft, (3) no difference |
| Q: Which type of graft typically has a predictable graft size? |
| (1) Allograft, (2) autograft, (3) they both have predictable graft size, (4) neither has a predictable graft size |
|
|
|
|
| Q: An allograft is from? |
| (1) Oneself, (2) donor, (3) laboratory |
| Q: An autograft is from? |
| (1) Oneself, (2) donor, (3) laboratory |
| Q: This graft may be irradiated to prevent infection: |
| (1) Allograft, (2) autograft, (3) both |
| Q: Which type of graft typically results in shorter operative times when used for ACL reconstruction? |
| (1) Allograft, (2) autograft, (3) no difference |
| Q: Which type of graft results in an increased risk of failure in young athletes following ACL reconstruction? |
| (1) Allograft, (2) autograft, (3) no difference |
| Q: Which type of graft has no potential for harvest-site injury? |
| (1) Allograft, (2) autograft, (3) neither has potential to result in harvest-site injury, (4) both have potential to result in harvest-site injury |
| Q: Which type of graft is associated with greater risks of surgery (damage to surrounding vessels and nerves, damage to nearby structures, bleeding, etc) |
| (1) Allograft, (2) autograft, (3) no difference |
| Q: Which type of graft results in better functional outcomes in older/low-demand patients? |
| (1) Allograft, (2) autograft, (3) no difference |
| Q: If you had to undergo ACL reconstruction today, would you prefer to be treated with an… |
| (1) Allograft, (2) autograft, (3) no preference |
|
|
| Q: If you required treatment for ACL reconstruction and you indicated you would prefer to undergo treatment with an autograft, but your surgeon recommended treatment with an allograft, would you change your preference? |
| (1) Yes (2) No |
| Q: If you required treatment for ACL reconstruction and you indicated you would prefer to undergo treatment with an allograft, but your surgeon recommended treatment with an autograft, would you change your preference? |
| (1) Yes (2) No |
| Q: What information would you consider to be most influential in forming your preference? |
| (1) Surgeon recommendation, (2) information found on the Education Sheet, (3) previous experience with ACL reconstruction |
| Q: Please rank the section on the educational sheet that you found most influential |
| (1) What is it, (2) what is it used to treat, (3) types, (4) advantages, (5) risks/disadvantages, (6) treatment outcomes |
ACL, anterior cruciate ligament.
Final revision submitted December 19, 2023; accepted February 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.F. has received education payments from Pinnacle. R.F.L. has received education payments from Foundation Medical, consulting fees from Arthrex, nonconsulting fees from Smith+Nephew and Linvatec, and royalties from Arthrex and Smith+Nephew. J.H.G. has received education payments from Arthrex, consulting fees from Vericel and Smith+Nephew, nonconsulting fees from Smith+Nephew and Vericel, and honoraria from Vericel. J.B. has received education payments from Smith+Nephew and Arthrex, consulting fees from Smith+Nephew, nonconsulting fees from Arthrex and Smith+Nephew, honoraria from AcelRx Pharmaceuticals, and hospitality payments from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.