
Abstract
Background:
There are limited data on the epidemiology of anterior cruciate ligament (ACL) ruptures in elite adult soccer players, especially in the Russian Premier League (RPL). There is an increased risk of injury due to a combination of additional risk factors such as playing in extremely high and low temperatures, frequent long flights, and regular play on natural and artificial surfaces.
Purpose:
To study the epidemiology of ACL ruptures and determine the patterns associated with their occurrence in RPL soccer players.
Study Design:
Descriptive epidemiology study.
Methods:
All ACL ruptures requiring surgery sustained by players competing in the RPL across 12 competitive seasons between 2010 and 2022 were analyzed. All required data were collected from media analysis and confirmed by club doctors.
Results:
A total of 85 players sustained 100 injuries during 12 competitive seasons. A total of 96.5% of players returned to competitive play. The injury incidence in RPL and during participation of RPL teams in European Cups were 0.4760 and 0.5622 per 1000 playing hours, respectively. When analyzing the outcomes of the primary ACL surgery (a total of 76 operations), the following data were obtained: in 11 cases (14.5%), there was a reinjury on the ipsilateral knee joint and in 4 cases (5.3%) on the contralateral knee joint. The mean return–to-play time after all operations was 284 ± 116 days. The time of return to play after primary reconstruction was 289 ± 136 days, 278 ± 91 days after reconstruction on the contralateral knee and 271 ± 51.5 days after the first ACL revision reconstruction on the ipsilateral knee joints.
Conclusion:
RPL ACL injury epidemiology is similar to that in the other leagues from around the world, although there are factors that can potentially influence the number of these injuries.
Regular injuries and subsequent operations of large joints such as the knee may have a negative impact on the general health of soccer players after their career.2,4,5,11,14,21,23,25,31 Anterior cruciate ligament (ACL) injuries are among the most severe injuries in professional soccer. Despite the efforts of practitioners and physicians, the prevalence of these injuries is still increasing. 30 Most of the time they require surgical treatment and prolonged rehabilitation and are accompanied by a large number of recurring injuries, the incidence of which can reach 16% to 25% during a 3-year follow-up period. 3 In soccer players, the incidence of recurring noncontact ACL injuries is significantly greater (42%) than that of contact injuries. 9 Notably, the incidence of secondary ACL injuries before return to play (RTP) at high-level competition is 6.7%. 39 Previous research indicates that the duration of RTP in professional soccer is shorter than in other sports such as American football, baseball, or basketball but is still considerable and has been reported to be 6.6 to 7.4 months in adult soccer players in European clubs.1,8,17,19,33,36
The incidence of ACL injuries can potentially be influenced by many factors. 6 The most significant of these include sex, neuromuscular control, hormonal constitution, and the intensity of physical activity.18,29,37 A study by Waldén et al 41 involving 25 teams also reported that the incidence of ACL injuries was lower in northern European teams (compared with southern Europe) with a statistically significant difference, especially for noncontact ACL rupture injuries.
In this context, it is of great practical interest to study the epidemiology of ACL injuries and possible patterns of their occurrence. However, despite this, there are somewhat limited data on the epidemiology of ACL ruptures in the top divisions of various soccer championships (Italy, Brazil, Germany, Sweden, Qatar, and the United States).12,16,20,28,32,34,35 Moreover, no conclusive data are available for elite Russian soccer players. The motivation to investigate injuries in this particular group is due to the fact that only in the Russian Premier League (RPL) is there a combination of possible risk factors such as playing in extremely high (>30°C in May-August) and low temperatures (<0°C in November, December, February, and March), frequent long flights (from 1 hour to 9 hours), and regular play on natural and artificial surfaces. For instance, between 2016 and 2021 alone, 67 matches started at -5°C and below, 111 matches at -4°C to 0°C, 161 matches at 1°C to 5°C, 186 matches at 6°C to 10°C, and a further 363 matches at 11°C to 20°C. Also, in each of the analyzed seasons, there was at least 1 team playing their home matches on an artificial turf. 26
Therefore, the aim of this study was to examine the epidemiology and return-to-play aspects of ACL ruptures and determine the patterns associated with their occurrence in a specific group of soccer players from the RPL over 12 consecutive seasons between 2010 and 2022. Our hypothesis was that there would be a higher incidence of ACL ruptures in the RPL compared with other top soccer leagues.
Methods
All ACL ruptures sustained by players from the RPL and that required surgery between 2010 and 2022 were analyzed. The study period commenced at the start of the 2010 competitive season and concluded at the end of the 2021/2022 season. A total of 12 competition seasons were analyzed. In 2010, the competitive season started at the end of February and ended at the beginning of December (ie, spring-fall system). By decision of Executive Committee of Russian Football Union, from 2011 and subsequent years, the competitive seasons started in early-July and ended in mid-May (autumn-spring system). During the COVID-19 seasons (2020/2021 and 2021/2022), tournaments were played as usual although without a live audience. In each of the analyzed seasons, 16 teams participated in the RPL. According to Russian Football Union regulations, each team's squad comprised no more than 25 people. Players who had previously sustained an ACL injury before the period of the study were not included. Only injuries that occurred during a particular team's participation in the RPL were taken into account.
The inclusion criteria for the study were the following: player was registered with the club when the injury occurred and player participated in at least one first team championship or cup match during the study seasons or the season preceding the injury (to include injuries sustained during the off-season).
The following indicators were analyzed: total number of ACL injuries; mean player age at the time of injury; total number of primary ACL injuries; number of recurrent ACL injuries (ie, ipsilateral knee); number of ACL injuries on the contralateral knee joint after a primary ACL reconstruction; injury situation (ie, the event during which the injury occurred: official or friendly match, training, domestic activity); number of ACL ruptures in each of the analyzed seasons; number of ACL injuries sustained during players’ participation in RPL and European Cup matches; season period of the injury (preparatory or competitive period); distribution of ACL ruptures by month of the year; player position according to the grading proposed by Mallo et al 22 ; length of RTP after primary ACL reconstruction; length of RTP after recurrent ACL reconstruction; number of surgeries performed in clinics in different countries; number of ACL injuries in teams that most frequently played in the RPL during the study period; and match exposure in the RPL and European competitions.
All data were obtained from the website transfermarkt.de by 3 independent sports medicine experts (team physicians). Data were also confirmed by club doctors. In case of mismatching data, all information was validated by 1 of the experts personally with the players who sustained the ACL injury.
Relapse injury was defined as any ACL graft injury resulting in surgical treatment before participation in the first friendly or competitive match. Reinjury was defined as an ACL injury sustained at any time resulting in surgical treatment after resuming participation in matches. “Career end” was defined as no participation in friendly or competitive matches for 24 months after the primary surgery related to the ACL rupture. Duration of the RTP was defined as the period between the date of injury and the first participation in a competitive match. Injury incidence for 1000 playing hours was calculated according to the formula described by Phillips and in a consensus statement on injury definitions in football studies15,31:

The study was performed in accordance with the Declaration of Helsinki. The study was also approved by the local ethics committee of Sechenov University [N 22-21 dated December 9, 2021]. Informed consent was obtained from all individual participants included in the study.
Statistical Analysis
Statistical analysis was carried out using IBM SPSS (Version 23.0.) Descriptive statistic methods were used to describe the resulting dataset. The Shapiro-Wilk test was used to assess the normality of the RTP timing distribution. A further comparison of timing according to the type of injury (primary, secondary ipsilateral, secondary contralateral) was performed by analysis of variance. Pearson chi-square test was used to compare the frequency of injuries according to the season and incidence of injuries. Results were considered statistically significant at P < .05.
Results
A total of 100 ACL injuries occurred in 85 players (mean age at injury, 26.2 ± 3.5 years) from 21 teams during 12 competitive seasons between 2010 and 2022, with a mean age at primary injury of 25.3 ± 3.7 years. None of the participants were excluded. On average, there were 8.3 ACL injuries in each of the 12 competitive seasons, approximately 1 ACL injury per 2 teams. The most common injury situation was official match play and team training, with 58 and 29 injuries, respectively. Another 11 injuries occurred during friendly games, 1 injury during domestic activity, and 1 during rehabilitation training.
Only 3 players (3.5%) out of 85 ended their soccer career due to injury. Thus, 96.5% of players have returned to play. Out of 100 ACL injuries, 76 (76%) were primary, 6 (6%) were on the contralateral limb, and 18 (18%) were recurrent on the ipsilateral limb. In 3 cases (3%), the reinjury occurred before the player's participation in the match.
When analyzing the outcome of primary ACL reconstruction (total of 76 operations), the following data were obtained in relation to the number of reinjuries: in 11 cases (14.5%) the reinjury occurred on the ipsilateral knee joint, and in 4 cases (5.3%) the injury was on the contralateral knee joint. Thus, the total percentage of reinjuries after primary ACL surgery was 19.7%.
The mean time of RTP postsurgery was 284 ± 116 days. The duration of RTP postprimary reconstruction was 289 ± 136 days, and the duration of RTP after ACL revision reconstruction on the ipsilateral knee joint was 271 ± 51.5 days. The mean time of RTP post-ACL reconstruction on the contralateral joint was 278 ± 91 days. No statistically significant difference (P = .73) was found when comparing the time of RTP postprimary reconstruction on the contralateral with the postrevision reconstruction on the ipsilateral knee joints.
The mean number of days before reinjury on the ipsilateral limb was 738 ± 459 days (range, 254-1575 days) and on the contralateral limb was 1792 ± 1245 days (range, 200-3633 days).
Central and wide midfielders sustained the most injuries, at 25% and 22%, respectively, while goalkeepers were the least injured (6%). Central defenders and forwards had the smallest number of reinjury cases: 1 in each group. Four goalkeepers had 6 ACL injuries. Moreover, there were recurring injuries in all cases (2 goalkeepers had 3 ACL injuries, including 1 before 2010, and 2 goalkeepers had 2 ACL injuries).
When analyzing the number of ACL injuries across competitive seasons, no difference in frequency between seasons was observed (P > .05) (Figure 1). When dividing 12 competitive seasons into 2 6-season periods, the number of injuries in 2010 to 2015/2016 compared with 2016/2017 to 2021/2022 was 53 and 47, respectively. However, this difference was not statistically significant.
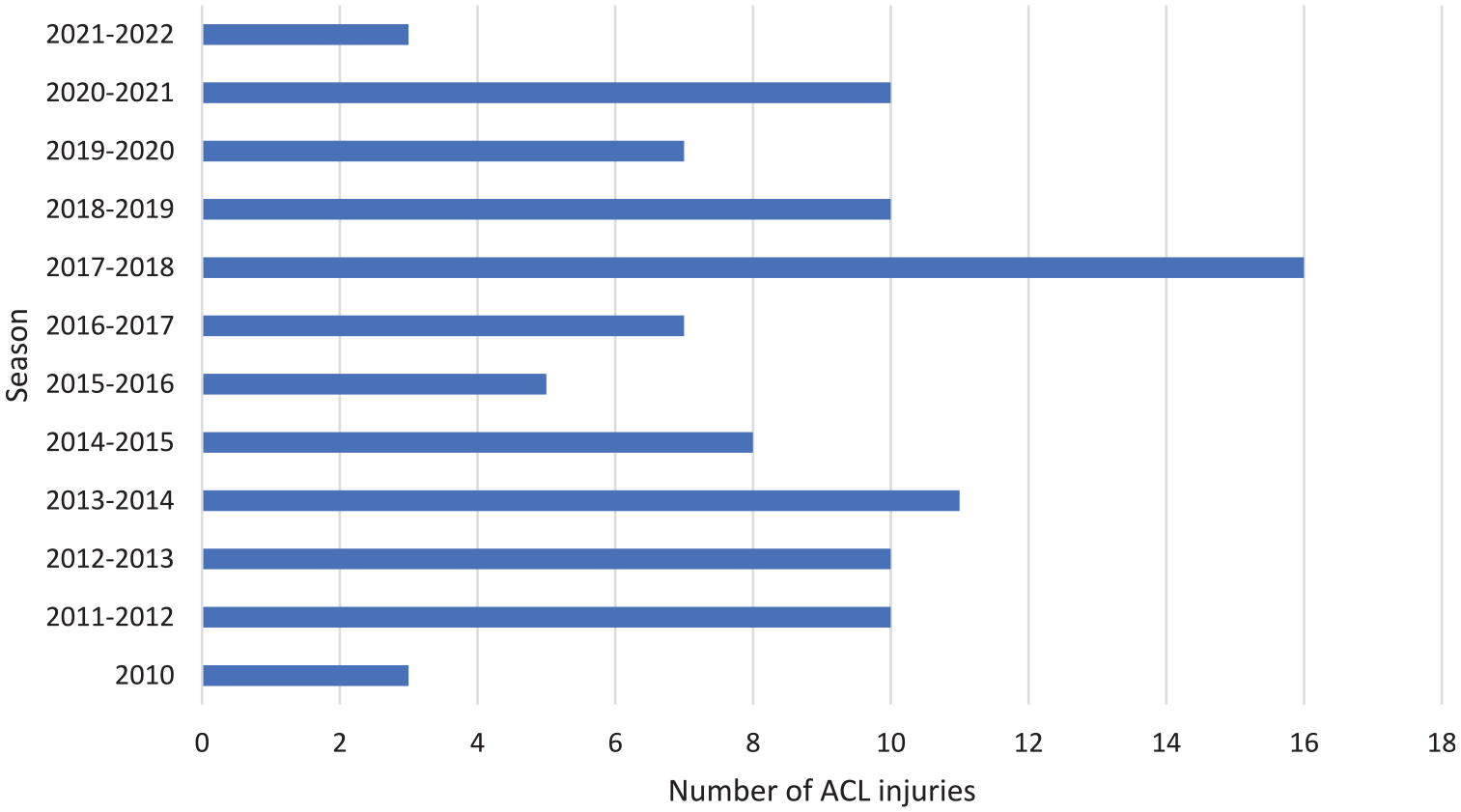
Distribution of ACL injuries in Russian Premier League players in each of the competitive seasons. ACL, anterior cruciate ligament.
A total of 79 injuries occurred during the competition period (from late-February to mid-May and from late-July to early-December) and 21 during the preparation period (from late-May to late-July and from mid-January to late-February). When analyzing the number of injuries by month, the highest incidence was in August and September—the first 2 months after the start of the championship and the participation of leading clubs in European Cup competitions (Figure 2).

Distribution of ACL injuries in Russian Premier League players during the calendar year. ACL, anterior cruciate ligament.
Incidence of ACL injuries during the RPL and European Cup matches was analyzed. During the study period, 31 teams played a total of 5984 and 539 matches in the RPL and European Cup, respectively. The number of sustained ACL ruptures during European Cup matches was 5. Therefore, the injury incidence in the RPL was 0.4760 per 1000 playing hours and in European Cup matches 0.5622 per 1000 playing hours. The difference in incidence was not statistically significant.
The analysis revealed that the largest number of ACL injuries was present in teams with the highest participation rate in European competitions (Figure 3).

Distribution of ACL injuries in teams that participated in at least 10 competitive seasons during the study period. ACL, anterior cruciate ligament.
The countries in which surgeries were performed were also analyzed. The most frequent countries in which operations were performed were Germany (44 cases), Italy (36 cases), and Spain (7 cases). In Germany, the operations were performed by several surgeons, while in Italy almost all operations were performed by a single surgeon (35 out of 36).
Discussion
This study examined the epidemiology of ACL ruptures in RPL soccer players during the 2010 to 2021/2022 competitive seasons. The main findings are comparable with results from previous studies in other professional leagues, namely the mean age at primary ACL injury, the number of primary and recurrent ACL ruptures, the percentage of players returning to competitive matches, and the distribution of these injuries across playing positions.
The mean age at primary ACL injury of players from leading European clubs and the top clubs from the Qatar and US leagues was in the range of 24.2 to 25.6 years, which is similar to our data obtained from the RPL (25.2 ± 3.7 years).7,12,27,32,40 The mean number of ACL ruptures during each of the analyzed seasons was 8.3 per 16 teams (0.52 injuries per team per season) with no statistically significant differences during the observation period. Similar results were obtained in studies involving Series A, Bundesliga, and Qatar Star League players. In these leagues, the mean number of ACL ruptures was 0.6, 0.53, and 0.51 per team in each season, respectively, across a minimum of 5 years of observation.16,32,35 It should also be noted that the number of ACL injuries in the RPL was larger during matches compared with training. However, the rate of such injuries during training was also high, with almost 30% of ACL injuries in RPL players sustained during training. Although this rate is lower than that of Series A (40%) and Qatar Star League players (40%), it can still be considered high and suggests the need for measures to improve training safety.16,32
Our results are also similar to those of studies that looked at the number and location of recurrent ACL ruptures in adult professional athletes. In RPL soccer players with primary ACL ruptures, repetitive lesions occurred in 19.7% of cases and were localized most frequently in the ipsilateral knee joint, which is consistent with earlier findings in soccer players and representatives of other sports. In previous studies, the incidence of recurrent injuries was estimated to be between 10% and 24%, and they were localized most frequently in the ipsilateral knee joint.13,42
The vast majority of players (97%) from the RPL were able to return to competitive play. This return rate can be described as very high and similar to that reported in other studies involving adult soccer players in which the RTP rate was over 93%.3,20 However, a number of studies examining elite soccer players from Europe and the United States have reported much lower return rates of 80% and 77%, respectively.9,12 Thus, it can be assumed that soccer players have one of the highest return rates to regular training activity across different sports.
The estimated duration of RTP after primary ACL reconstruction in RPL players was 289 days, which was longer than in previous studies on players of leading European clubs and the Qatar Star League, where the duration was approximately 225 days. 39 This difference may be due to a variation in the RTP definition. For example, in the study by Rekik et al, 32 RTP was calculated from the date of injury to the date of return to full participation (player being medically discharged and fully ready for unrestricted training and match play), while in our study the RTP was defined as the time from the injury to the first officially recorded participation in any match (including friendly matches).
When looking at match exposure of ACL ruptures during matches in the RPL, our results were comparable with those of the Italian Series A, the Qatar Stars League and the top division of the Brazilian championship. In the RPL, the injury incidence was 0.4760 per 1000 playing hours compared with the abovementioned leagues that were in the range of 0.41 to 0.61 per 1000 hours of matches.16,20,35 Furthermore, a study investigating 25 European and Bundesliga clubs found ACL ruptures to be 0.36 and 0.34 per 1000 hours of matches, respectively. 38 The most frequent injuries were in most successful teams (at the time of the study), most frequently ranked first in their championship, and participating regularly in the European competitions. These findings are consistent with the results obtained from the Italian Series A. 16
Notably, our study showed that goalkeepers have the lowest risk of ACL injury. These findings are consistent with those of other studies involving players of leading European teams, including those from the Italian and German championships. 10 One possible explanation for this may be the peculiarities of this playing position. Most often there are 3 goalkeepers in the squad, yet only 1 goalkeeper performs consistently in most competitive matches. The remaining 2 goalkeepers only train and thus the risk of ACL injuries is much lower. It should also be noted that, in this study, 4 goalkeepers had 6 ACL injuries; there were recurring injuries in all cases (2 goalkeepers had 3 ACL injuries, including 1 before 2010, and 2 goalkeepers had 2 ACL injuries). Although the sample is very small, it can be concluded that practitioners need to pay attention to this specific injury pattern in goalkeepers.
The analysis of ACL rupture incidence in the RPL during the calendar year revealed a bimodal peak, with the largest number of ACL ruptures in August and September and in February and March. This pattern may be related partially to the start of the competitive season and the top teams competing in European Cups in August and September as well as the start of preparation period in January. The resumption of the RPL in February, after a winter break, on surfaces of poor quality may also be a contributing factor. This distribution may also indicate that ambient temperature is not an important risk factor for ACL injuries. A study by Sandon et al 34 showed that the largest number of ACL injuries in players from the Swedish championship occurred in March and April, in the first 2 months after the start of the competitive season. Similar data were obtained in German professional soccer players. This distribution of injuries may be due to the accumulated workload during preseason training and the significant difference between the workload during friendly and official matches, which generally affects starting players. This may also lead to a higher risk of overexertion during matches and to worse recovery between the matches. However, in another study assessing players from the Italian Series A, the distribution of ACL injuries during the calendar year was somewhat different. The study by Grassi et al 16 found a bimodal peak of ACL injuries, but the distribution of these injuries was highest in October and March. The authors further explained this distribution by the negative impact of the physical preparation phase combined with the start of official fixtures for the first peak of injuries in October.
Our study also compared the RTP time after primary ACL reconstruction, contralateral reconstruction and the first revision reconstruction on both the ipsilateral and contralateral knee joints. The difference in RTP time was not statistically significant in all cases. These data are inconsistent with the results of a previous study, according to which the duration of rehabilitation after revision ACL reconstruction is significantly longer compared with rehabilitation after the primary injury. 24 A possible explanation for the similar RTP timing after primary and revision reconstructions of the ACL in RPL players may be related to the reinjuries occurring on average ≥2 years after primary reconstruction as well as the players being previously in good functional condition. Furthermore, the reoperations were always performed by experienced surgeons in leading German, Italian, and Spanish clinics on players with previous experience of recovering from primary ACL reconstruction, which could have had a positive influence on the recovery process. The data obtained on the location of the clinics where the operations were conducted may also be of interest. Almost all of the players injured during the study period did not receive surgery in Russia. This fact may be an indication that, at least in Russia, the club doctor's choice of surgeon is based not on convenient logistics and the cost of surgery but on the experience of a particular surgeon in performing similar operations on professional soccer players.
Limitations
There are several limitations of the study. Given its retrospective nature, accurate information about the timing of regular training activity resumption after ACL surgery could not be obtained and the duration of rehabilitation was assessed by participation in the first official match. Thus, it was not possible to examine the presence and nature of concomitant injuries of the knee joint. This, in turn, could have had an effect on the duration of rehabilitation, despite the fact that the ACL rupture is most often the pathology responsible for its duration. The lack of information about weather conditions and playing surface is another limitation. In addition, the study did not assess the sporting success of soccer players several years after surgery, which could be a subject for future research.
Conclusion
The epidemiology of RPL ACL injuries is similar to that in other leagues from around the world, although there are factors that can potentially influence the number of these injuries. Almost all players were able to return to competitive activity after ACL reconstruction. The estimated duration of RTP after primary ACL reconstruction in RPL players was longer than in previous studies in players of other top leagues; however, this difference may be due to a variation in the RTP definition. The difference in RTP time after primary ACL reconstruction and the first revision reconstruction on both the ipsilateral and contralateral knee joints was found to be not statistically significant. The most frequent ACL ruptures occurred in the first 2 months after resumption of competitive matches and were most frequent in players of the most successful teams.
Footnotes
Final revision submitted January 15, 2024; accepted February 12, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from First Moscow State Medical University (22-21).