
Abstract
Background:
Treatment strategies for meniscal tears range from nonoperative management to surgical intervention. However, national trends in cost-related outcomes and patient factors related to the failure of nonoperative management remain poorly understood.
Purpose:
To describe the costs associated with nonoperative versus operative management of meniscal tears in the 2 years after diagnosis and examine the relationship between patient characteristics and timing of surgery.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This study was conducted using the MarketScan databases. Patients diagnosed with a meniscal tear without concomitant knee osteoarthritis between January 1 and December 31, 2017, were included. The primary outcome was the total cost of meniscal tear-related procedures—including insurance deductibles, coinsurance, and net insurance payments—in the 2 years after diagnosis. Procedures included were as follows: (1) surgery—including meniscectomy or meniscal repair; (2) physical therapy; (3) medication—including nonsteroidal anti-inflammatories, opioids, and acetaminophen; (4) intra-articular injections—including professional fee, hyaluronic acid, and corticosteroids; (5) imaging; and (6) clinic visits to orthopaedic specialists. Patients were grouped as having undergone early surgery (ES) (≤3 months of diagnosis), late surgery (LS) (>3 months after diagnosis), or no surgery (NS). Multivariate logistic regression was performed to determine the likelihood of undergoing surgery early and failing nonoperative treatment.
Results:
The study population included 29,924 patients with a mean age of 43.9 ± 12.9 years (ES: n = 9507 (31.8%); LS: n = 2021 (6.8%); NS: n = 18,396 (61.5%)). Complex (36.6%) and medial (58.8%) meniscal tears were the most common type and location of injuries, respectively. The mean cost of management per patient was $3835 ± $4795. Costs were lower in the NS group ($1905 ± $3175) compared with the ES group ($6759 ± $5155), while the highest costs were observed in the LS group ($7649 ± $5913) (P < .001). Patients who were men, >40 years, and with a bucket-handle or lateral meniscal tear were more likely to undergo surgery early. Patients who were men, <30 years, and with a complex tear or tear to the lateral meniscus were more likely to fail nonoperative management.
Conclusion:
Nonoperative management had the lowest cost burden and should be recommended for patients with appropriate indications. However, if surgery is necessary, it should be performed earlier.
Meniscal injuries of the knee are common, and the incidence of tears to the meniscus has been estimated to be 60 per 100,000 individuals. 4 Treatment strategies may range from conservative management to surgical procedures, such as meniscectomies or meniscal repairs. The costs associated with these procedures are high, with varying levels of treatment efficacy.8,15 As we transition toward a value-based health care system, it is important to reduce disease burden by utilizing an evidence-based decision-making framework to manage patients with meniscal tears.
The risk factors of meniscal tears have been widely studied, including age,6,17 obesity, 6 and sports participation.1,2 The common approach to the treatment of meniscal tears has been to adopt a conservative approach for degenerative injuries, while surgical interventions are often recommended for traumatic tears. 12 However, identifying patient characteristics associated with failure of nonoperative management of meniscal tears remains poorly understood because of the lack of studies conducted. 16 Much less is known about factors related to traumatic meniscal tears and the prevalence of these factors related to surgery.
This study aimed to describe the costs associated with nonoperative versus operative management of meniscal tears in the 2-year period after diagnosis and examine the relationship between patient characteristics and timing of surgery.
Methods
Data Source
Ethical approval for this study was obtained from our institution. This study was conducted using the MarketScan Commercial Claims and Encounters and MarketScan Medicare Supplemental and Coordination of Benefits databases (Merative). The Commercial Claims and Encounters database comprises medical and drug data from employers and health plans in the United States for more than 203 million people annually, encompassing employees, their spouses, and dependents covered by employer-sponsored private health insurance in the United States. The Medicare Supplemental and Coordination of Benefits database consists of the Medicare-covered portion of the payment (represented as Coordination of Benefits Amount), the employer-paid portion, and any out-of-pocket patient expenses. 9
Inclusion and Exclusion Criteria
Patients aged 18 to 65 years who were diagnosed with a meniscal tear between January 1 and December 31, 2017, were included in the study. Patients with a concurrent knee osteoarthritis diagnosis were excluded. Patients who had switched insurance providers in the 2 years after diagnosis were also excluded from the analysis.
Outcomes
The primary outcome was the cost of meniscal tear-related procedures in the 2 years after diagnosis. This included deductibles, coinsurance, and net insurance payments (inflation-adjusted to July 1, 2020, US dollars). 18 Current Procedural Terminology and International Classification of Diseases–10th Revision codes were used to identify procedures and diagnoses, respectively (Appendix Table A1). Procedures included were as follows: (1) surgery—including meniscectomy or meniscal repair; (2) physical therapy; (3) medication—including nonsteroidal anti-inflammatories, opioids, and acetaminophen; (4) intra-articular injections—including professional fees, hyaluronic acid, and corticosteroids; (5) imaging; and (6) clinic visits to orthopaedic specialists. Patients were grouped as either having early surgery (ES) (surgery <3 months of diagnosis), late surgery (LS) (>3 months after diagnosis), or undergone no surgery (NS) (Figure 1); we believe that both the LS and NS groups together represented patients who attempted nonoperative management, with the LS likely representing failed attempts and the NS representing successful nonoperative management. The cutoff period of 3 months was chosen because most patients (>80%) who underwent surgery did so within this period (Figure 2).

Flowchart of patient management timeline and rationale for selected multivariate logistic regression models. ES, early surgery; LS, late surgery; NS, no surgery.

Distribution of time to surgery after diagnosis.
Statistical Analysis
Descriptive analyses were performed to compare the aggregate costs of all procedures that took place in the 2-year postdiagnosis period, with differences compared using 1-way analyses of variance or chi-square tests. Multivariate logistic regression was performed to determine the likelihood of undergoing ES and the likelihood of undergoing eventual surgery in patients who had undergone at least 3 months of nonoperative management, adjusting for patient and injury characteristics. All statistical analyses were performed using STATA Version 17.0 (StataCorp), and P < .05 was considered statistically significant.
Results
A total of 29,924 patients (Northeast, 16.5%; Midwest, 21.3%; South, 47.7%; and West, 14.6%) were included in the analysis, with a mean age (±SD) of 43.9 ± 12.9 years, and 12,922 women (43.2%) (Table 1). Of the included patients, 61.5% (n = 18,396) did not undergo surgery, 31.8% (n = 9507) underwent surgery early, and 6.8% (n = 2021) underwent surgery late.
Demographic and Injury Characteristics of Patients With Meniscal Tears in 2017 a

Data are presented as mean ± SD or n (%). Dashes indicate areas not applicable. Bold P values indicate statistically significant differences between groups (P < .05). ACL, anterior cruciate ligament; COPD, chronic obstructive pulmonary disease; ES, early surgery; LS, late surgery; NS, no surgery.
Complex tears (36.6%) were the most common type of tear reported, and the medial meniscus (58.8%) was the most common tear location. The mean management cost per patient was $3835 ± $4795 (Table 2). Costs were significantly lower in the NS group ($1905 ± $3175) compared with the ES group ($6759 ± $5155), while the highest costs were observed in the LS group ($7649 ± $5913) (P < .001).
Two-Year Postdiagnosis Management Costs a
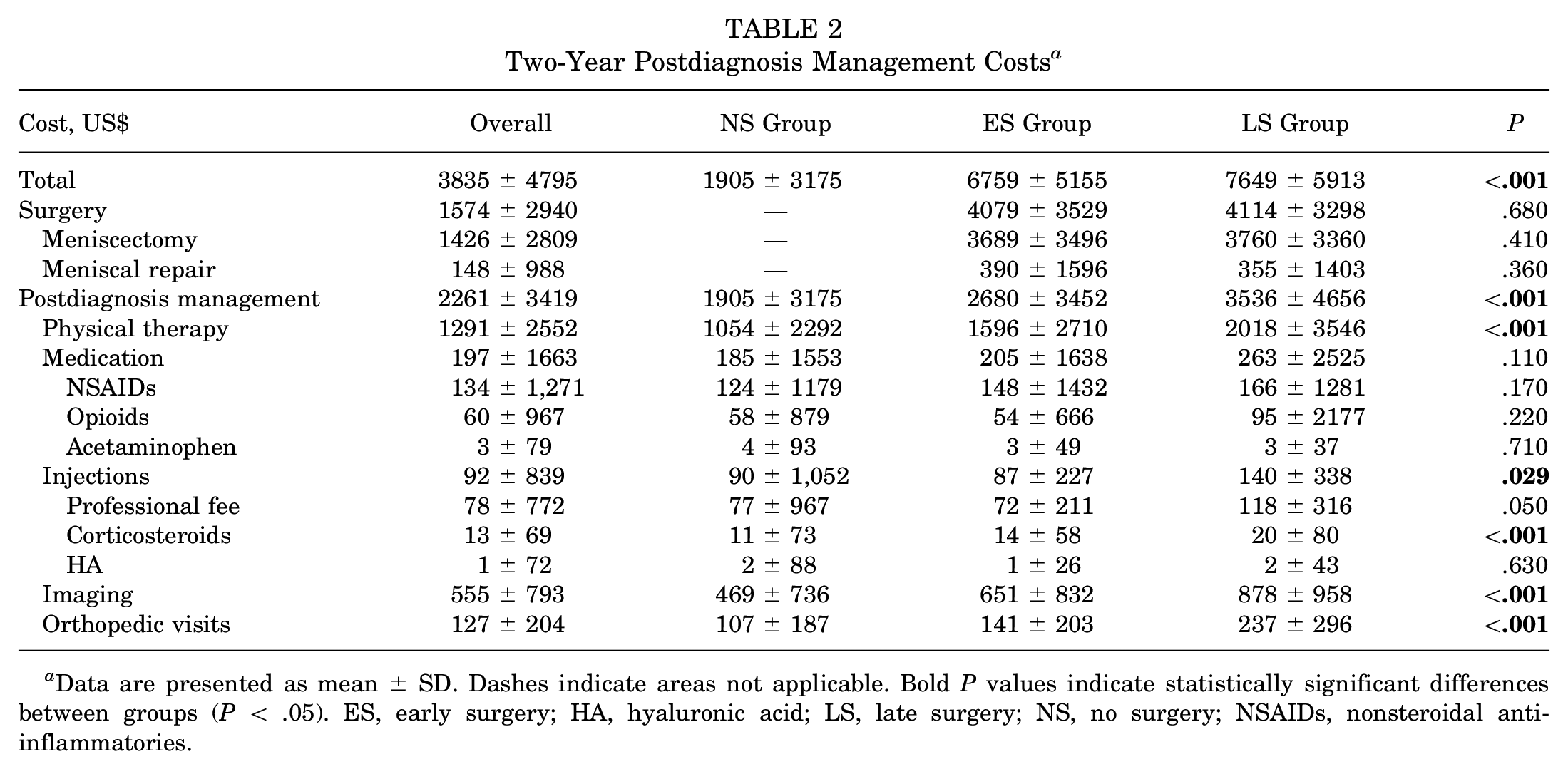
Data are presented as mean ± SD. Dashes indicate areas not applicable. Bold P values indicate statistically significant differences between groups (P < .05). ES, early surgery; HA, hyaluronic acid; LS, late surgery; NS, no surgery; NSAIDs, nonsteroidal anti-inflammatories.
Within the 2-year follow-up period, patients who were >40 years, men, obese, with a bucket handle tear, a lateral meniscal tear, or a concurrent anterior cruciate ligament tear were more likely to undergo surgery early (Table 3). Among patients who attempted nonoperative management for at least 3 months (ie, the NS and LS groups), those who were <30 years, men, obese, or had a complex tear or a tear to the lateral meniscus were more likely to fail and have surgery later, while higher utilization of physical therapy (>10 sessions) and pain medication (at least 1 prescription) were associated with a reduced risk of failure and delayed surgery (Table 4).
Likelihood of Undergoing Early Surgery Based on Patient and Injury Characteristics a

Dashes indicate areas not applicable. Bold P values indicate statistical significance (P < .05). COPD, chronic obstructive pulmonary disease; ACL, anterior cruciate ligament; OR, odds ratio.
Reference variable.
Likelihood of Eventual Surgery After 3 Months of Nonoperative Management Based on Patient and Injury Characteristics a

Results were assessed in patients who attempted nonoperative management for at least 3 months. Dashes indicate areas not applicable. Bold P values indicate statistical significance (P < .05). ACL, anterior cruciate ligament; COPD, chronic obstructive pulmonary disease; OR, odds ratio.
Reference variable.
Discussion
The findings of this study indicated that the costs associated with managing meniscal tears are substantial and could be attributed to a variety of procedures that patients undergo. Although several studies have found nonoperative treatment modalities such as physical therapy to be similar to, or better than, surgical treatment of degenerative meniscal tears,5,10,13 much less is known about treatment approaches in younger patients with meniscal injuries and without concomitant knee osteoarthritis. The main finding of this study was that the cost of health care utilization among patients who underwent nonoperative management was lower than those who underwent surgery. This suggests that nonoperative treatment strategies may be a reasonable first-line approach to managing meniscal tears in this population without resulting in an excessive cost burden. However, it is also possible that patients undergoing nonoperative treatments may have experienced less severe symptoms, as reflected by a reduced need for physical therapy or medication after diagnosis.
Although a small number of studies have found that nonoperative management is suitable for traumatic tears,3,7 it is likely that a conservative approach may only be suitable for patients with limited indications. Early surgical intervention should still be recommended for traumatic injuries with specific causes.12,14 Therefore, it is important for cost-related outcomes reported in this study to be interpreted in tandem with the results of investigations related to injury type and severity. This would strengthen guidelines based on cost-effectiveness for the treatment of meniscal tears.
Determining the need for surgery is typically surgeon-driven based on the assessment of injury location and severity. However, beyond these injury characteristics, there is poor consensus on other patient factors that may influence the decision-making process. While degenerative meniscal injuries may be more responsive to conservative treatment, traumatic meniscal tears may warrant ES to prevent subsequent degeneration. 20 In our study, we found that the decision for ES was associated with patients who were older, male, obese, and had a lateral tear or concomitant anterior cruciate ligament injury. Other patient factors that may influence the decision for ES could include patient occupation, patient desire to resume physical activity quickly, availability of social support, or simple patient preference for surgical intervention.
In addition to factors associated with ES, we also identified factors that are associated with failure of nonoperative management. Patients who were younger, male, obese, or had a lateral meniscal injury were more likely to end up undergoing surgery within 2 years of diagnosis. We also found that postdiagnosis costs were approximately 30% more in patients who failed attempted nonoperative management compared with patients with early surgical intervention.
Other interesting findings were noted in this study. Patients who underwent more physical therapy sessions in the 3 months after diagnosis were less likely to fail nonoperative treatment. This supports the results of prior studies that physical therapy alone may be as effective as surgical intervention for some patients.11,19 A similar finding was also found in patients who received more prescriptions of pain medication. Further prospective studies should be conducted to determine the relationship between patient factors and response to specific nonoperative treatments. As the health care system transitions toward a value-based model, our findings of risk factors for failed nonoperative management, if implemented into clinical decision-making, could translate into substantial savings (as much as 30%) for the care of these patients.
Strengths and Limitations
The strength of this study lies in the utilization of a large national database that includes information from different hospitals and providers. This allows tracking of patients across institutions and provides information about patient history that single-institution studies may lack. The large study sample and extended length of follow-up of 2 years more accurately reflect national utilization trends and help to assimilate the results of prior single-institutional studies. This study utilized a nationwide database to identify potential risk factors for the failure of nonoperative management. In addition, it analyzed cost-related outcomes of meniscal tears and provided valuable information about 1 of the most common knee injuries reported in the United States.
A limitation of this study is the inability to document treatments with over-the-counter availability. Therefore, it is possible that the actual utilization of some procedures (eg, bracing and nonsteroidal anti-inflammatories) has been underestimated because of the patients’ willingness to pay out-of-pocket without insurance coverage. In addition, patient groups could not be matched for injury severity because of the absence of granular data. In the present study, laterality codes could not be confidently used to attribute all procedures identified to the ipsilateral knee. However, because of the proximity of the procedures performed to the time of diagnosis, it is likely that for most patients, the procedure performed was for the ipsilateral knee. Furthermore, the database is dependent on accurate coding by providers. Therefore, future investigations with available data could strengthen the results of this study by controlling for injury severity.
Conclusion
Nonoperative management of meniscal tears has the lowest cost burden and should be recommended for patients with appropriate indications. However, if surgery is required, it should be performed earlier. Clinicians could consider utilizing a decision-making framework based on patient and injury characteristics to determine the necessity and timing of surgery. Further investigation into validating similar decision-making frameworks through prospective studies is warranted.
Footnotes
Appendix
ICD-10 and CPT Codes for Identifying Diagnoses and Procedures a

| Variable | ICD-10 or CPT Code |
|---|---|
| Diagnosis | |
| Meniscal tear | S83.2− |
| Knee osteoarthritis | M17− |
| Procedure | |
| Meniscectomy | 29880, 29881 |
| Meniscal repair | 29882, 29883 |
| Physical therapy | 97110, 97140, 97010, 97014, 97112, 97001, 97530, 97035, 97032, 97116, 97012, 97016, 97535, 97113, 97124, 97033, 97150, 97026, 29530, 97750, 95831 |
| Injection fee | 20610, 20611, 77002, 76942 |
| IA-HA | Q4083, J7319, J7321, J7322, J7323, J7324, J7325, J7326 |
| IA-CS | J0702, J0704, J1020, J1030, J1040, J1094, J1100, J1700, J1710, J1720, J2650, J2920, J2930, J3300, J3301, J3302, J3303 |
| Imaging | 73560, 73562, 73564, 73565, 73700, 73701, 73721, 73722, 73723 |
| Clinic visits (orthopaedics) | 99211, 99212, 99213, 99214, 99215 |
ICD-10 codes were used to identify diagnoses; CPT codes were used to identify procedures. − indicates that subsequent alphanumeric characters are included. CPT, Current Procedural Terminology; IA-CS, intra-articular corticosteroid injection; IA-HA, intra-articular hyaluronate injection; ICD-10, International Classification of Diseases–10th Revision.
Final revision submitted November 14, 2023; accepted December 5, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.P. has received grant support from Arthrex; education payments from Arthrex, Smith+Nephew, and Legacy Ortho; and hospitality payments from Stryker. S.S.S. has received education payments from Arthrex and Smith+Nephew; consulting fees from DePuy Synthes and Exactech; and hospitality payments from Encore Medical. A.J.R. has received education payments from Arthrex. E.G.M. has received education payments and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from New England Baptist Hospital (ref No. 2022-25).