
Abstract
Background:
While prevention protocols have been implemented, skiing-related musculoskeletal injuries and concussions continue to present to emergency departments in the United States. Previous literature has suggested the pediatric population may constitute up to 40% of skiing-related injuries.
Purpose:
To assess injury trends and the underlying mechanisms of skiing injuries in pediatric patients seen at emergency departments in the United States.
Study Design:
Descriptive epidemiology study.
Methods:
The National Electronic Injury Surveillance System (NEISS) was queried for pediatric (age ≤18 years) skiing injuries between January 1, 2012, and December 31, 2022. Injury mechanism, location, disposition, and diagnosis were recorded, and the statistical sample weight assigned by NEISS by hospital was used to calculate national estimates (NEs). Injury trends were evaluated with linear regression analysis.
Results:
Overall, 2951 pediatric skiing injuries were included (NE = 123,386). The mean age of the patients was 12.4 ± 3.5 years, with 61.3% of the injuries occurring in male patients. Impact with the ground was the most common injury mechanism (NE = 87,407; 70.8%). Fractures were the most common diagnosis (NE = 38,527, 31.2%), followed by strains/sprains (NE = 22,562, 18.3%), contusions/abrasions (NE = 16,257, 13.2%), and concussions (NE = 12,449, 10.1%). The lower leg was the most common fracture site (NE = 9509, 24.7%), followed by the shoulder (NE = 7131, 18.5%) and lower arm (NE = 5876, 15.3%). Analysis of annual injuries revealed no significant trend between 2012 and 2022 (P = .17), with fluctuations apparent throughout the study period. Significant decreases were seen in strains/sprains (P < .01) and contusions/abrasions (P < .01), but not in concussions (P = .57) or fractures (P = .70).
Conclusion:
Impacts with the snow/ground made up 70.8% of all injuries. Fractures were the most common injury diagnosis, followed by strains/sprains, with the lower leg being most frequently fractured. While strains/sprains and contusions/abrasions showed a significant decline, there were no significant trends in fractures and concussions between 2012 and 2022.
Skiing is a popular winter sport, with an estimated 15 million participants in the United States and approximately 200 million worldwide.16,21 Participants across all age groups with varying levels of experience engage in the sport each year. 6 Although enjoyable, the sport presents an inherent injury risk given the complex biomechanical movements involved with navigating alpine slopes paired with high-speed falls and collisions.18,21
While skiing-related injuries were on the rise as the sport grew in the early 2000s, recent studies have pointed toward a decline in the past decade, especially given the rising popularity of snowboarding.6,21,31 While prevention protocols have been implemented,5,14,16 skiing-related musculoskeletal injuries and concussions continue to present to emergency departments (EDs) in the United States.10,15 Furthermore, while the pediatric population makes up approximately 20% of skiers, this demographic makes up a large proportion of injuries,3,15,21 with a study by Hurt et al 15 reporting approximately 40% of injuries being among youth skiers. Differences in anatomy, biomechanics, skill level, and coordination also result in distinctive injury patterns among pediatric skiers compared with adults.3,6,21
The purpose of this study was to assess injury trends and the primary mechanisms underlying skiing injuries in pediatric patients who visited US EDs between 2012 and 2022. Furthermore, we aimed to characterize injury trends and distribution by diagnosis type. The hypotheses were that (1) falls would contribute to a large portion of skiing-related injuries in this population, with fractures being the most common injury pattern and the lower extremities being a frequent fracture site; and (2) injuries would be decreasing due to the interventions implemented. These findings will be invaluable in guiding the assessment, treatment, and prevention of skiing-related injuries in pediatric patients, especially those that require an ED visit and work-up.
Methods
NEISS Database
We queried the National Electronic Injury Surveillance System (NEISS) database retrospectively for all skiing injuries (NEISS product code 3283) in the pediatric (≤18 years) population between 2012 and 2022. NEISS is a publicly available, de-identified national database operated by the US Consumer Product Safety Commission. ED visits are collected from a stratified probability sample of approximately 100 US hospitals with a minimum of 6 beds and a 24-hour operating ED. The NEISS dataset relies on a geographic sample of participating hospitals; thus, there is likely a large variation in the number of ski injuries based on location. The hospitals are grouped into 5 strata: 4 represent hospital EDs of various sizes and 1 represents EDs from children's hospitals. A statistical sample weight is assigned for each ED based on the inverse of the probability of selection, thus allowing for national estimates (NEs) of injuries to be calculated across the United States using the NEISS cases. Several epidemiological studies have utilized the NEISS database to characterize sports injuries,1,11,24,26,30,36 including those from snow sports.6,9,15,40 Institutional review board approval was not required for this study, as only publicly available data were included.
Data Extraction
There were 2991 cases of skiing-related injuries in pediatric patients between January 1, 2012, and December 31, 2022. For each injury case, the patient's demographic information (eg, age, sex, and race), date of visit, diagnosis, body area involved, and a visit narrative were available. Each narrative was reported by the health care provider to describe the injury and entered into the database by a trained coder. The narrative for each case was reviewed by 3 authors (A.Y., E.I.H., and K.K.O.), and the mechanism of injury and affected body parts were identified. The mechanism of injury was classified as impact with the snow/ground, impact with an object (tree, rock, etc), impact with another person, twisting motion, impact with ski poles, impact with skis, injured while getting on/off ski lift, other, or not specified in the narrative.
Exclusion Criteria
Injury cases were excluded if the patient was not a skier (eg, a snowboarder injured after colliding with skier), if the injury did not take place while skiing (eg, fall in the ski lodge, head injury from a falling ski boot), or if there was an injury mechanism or location that did not fit into the categories as above.
Statistical Analysis
The data were analyzed using IBM SPSS Statistics Version 28.0 (IBM Corp LLC). Descriptive statistics were performed and reported as NEISS cases and NEs (calculated using the statistical weights provided by the Consumer Product Safety Commission for each case). Linear regression analysis was used to analyze the relationship between the year and annual skiing-related pediatric injuries across the study period, with number of injuries as the dependent variable and year as the independent variable. The P value, regression coefficient (β), and 95% CI were reported when the data were statistically significant (P < .05).
Results
There were 2991 cases of pediatric (age ≤18 years) skiing injuries reported at US EDs between January 1, 2012, and December 31, 2022. Forty injuries that did not involve skiing (snowboarder injuries, injuries in ski lodge, or being hit by skis or ski boots not while skiing) were excluded, resulting in 2951 pediatric skiing injuries (NE = 123,386) that were included in the analysis. The mean age of the injured patients was 12.4 ± 3.5 years, with most injuries being among male (61.3%) and White (94.9%) patients (Table 1).
Characteristics of Skiing-Related Injuries in the Pediatric Population, 2012 to 2022 a
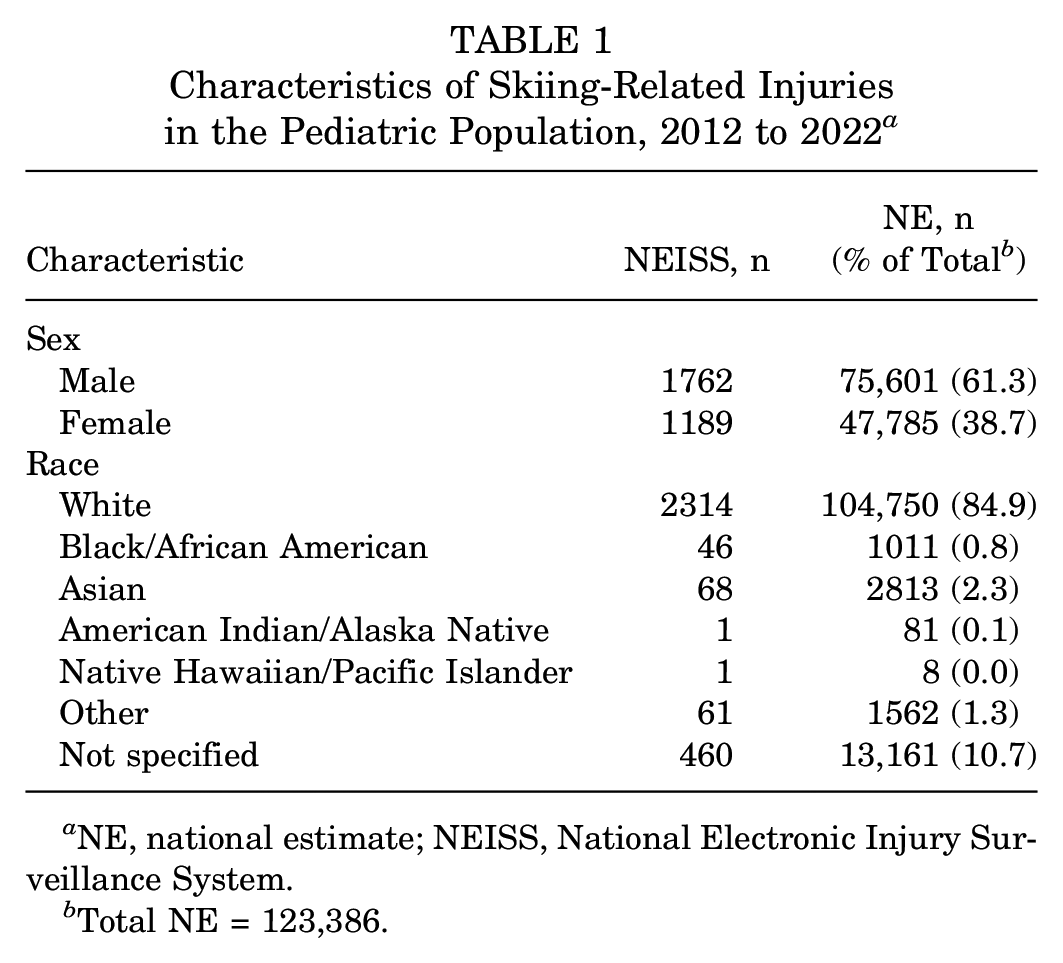
NE, national estimate; NEISS, National Electronic Injury Surveillance System.
Total NE = 123,386.
Linear regression analysis of annual injuries revealed no significant trend between 2012 and 2022 (P = .17) (Figure 1). Rather, injuries fluctuated during the study period. There was a slight increase from 2012 to 2013 and a slight decrease from 2013 to 2014, followed by larger decreases of 28.5% from 2014 to 2015 and 33.4% from 2015 to 2016. Injuries increased slightly in 2017, then increased by 51.8% from 2017 to 2018. Injuries then decreased in 2019 and 2020, followed by increases in 2021 and 2022. The 13,268 injuries reported at US EDs in 2022 was the highest in a single year nationally since 2014 and represented a 29.9% increase from 2021 (Figure 1).

National estimates for skiing-related pediatric injuries reported at US emergency departments between 2012 and 2022.
Injury Mechanism
The most common mechanism of injury was impact with the snow/ground, making up 70.8% (NE = 87,407) of injuries (Table 2). Impact with an inanimate object and injuries due to a twisting motion were the next most common, followed by injuries while getting on/off the ski chairlift. Collisions with other people made up 3.2% of injuries. Impact with ski poles, impact with skis, and other injuries made up a combined 3.2% of injuries.
Mechanism of Skiing-Related Injuries in the Pediatric Population, 2012 to 2022 a

NE, national estimate; NEISS, National Electronic Injury Surveillance System.
Total NE = 123,386.
Injury Diagnoses
Fractures were the most common primary injury diagnosis (NE = 38,527; 31.2%), followed by strains/sprains, contusions/abrasions, and concussions (Table 3). These 4 diagnoses made up over 70% of all national skiing injuries in the pediatric population. Among pediatric skiers aged ≤13 years, fractures made up 36.1% of all injuries, followed by strains/sprains making up 16.1%. In contrast, among the adolescent pediatric skiers (age, 14-18 years old), fractures made up 24.6% of all injuries, followed closely by strains/sprains at 21.3%.
Most Common Skiing-Related Injury Diagnoses in the Pediatric Population, 2012 to 2022 a

NE, national estimate.
Total NE = 123,386.
Linear regression analysis of annual trends of the 4 most common injury diagnoses between 2012 and 2022 revealed significant decreases in strains/sprains (P = .002; β = −270.76; 95% CI, −407.91 to −133.62) and contusions/abrasions (P = .007; β = −208.53; 95% CI, −354.14 to −71.92). However, no significant decreases in annual concussions (P = .57) or fractures (P = .70) were observed between 2012 and 2022, demonstrating that severe skiing-related head and musculoskeletal injuries remained prevalent and continued to be reported at US EDs (Figure 2).

National estimates for the 4 most common skiing-related pediatric injury diagnoses reported at US emergency departments between 2012 and 2022.
The lower leg was the body part fractured most commonly (NE = 9509; 24.7%), followed by the shoulder, lower arm, and wrist (Table 4).
Location of Skiing-Related Fractures in the Pediatric Population, 2012 to 2022 a

NE, national estimate; NEISS, National Electronic Injury Surveillance System.
Total NE for fractures = 38,527.
Only 4.5% (NE = 5562) of injuries reported at EDs required hospital admission, with 92% (NE = 113,515) being treated and released and 0.5% (NE = 615) leaving without treatment.
Discussion
The study findings indicated that skiing-related injuries in the pediatric population fluctuated between 2012 and 2022, with no significant linear trend. Furthermore, we found that impact with the ground was the most common mechanism of injury, with fractures being the most common injury diagnosis, frequently of the lower leg. Alarmingly, despite increased awareness and increased use of helmets and protective gear,12,20,33,41 there was no significant decline in concussion and fracture-type injuries between 2012 and 2022 according to study results.
The pediatric population may constitute 13% to 27% of the overall skiing population worldwide, yet some studies point to this demographic contributing to as much as 40% of skiing injuries seen in US EDs.15,28 The available literature also suggests that youth participants in snow sports in the US may face a higher risk of injury compared with adults. 40 Due to this notable injury burden among pediatric skiers, it is important for further research to determine which types of injuries are most common, their long-term impact, and ways to mitigate injury rates to maintain a healthy and active pediatric population moving forward. Furthermore, given that musculoskeletal immaturity of children and adolescents plays a key role in the burden of injury rates, identifying prevention strategies and protocols will be imperative to protecting pediatric skiers. 21 To our knowledge, this is the first study that has evaluated the epidemiology of injury patterns in this population.
A notable finding of this study was that skiing injuries in pediatric patients who visited US EDs showed no significant linear trend between 2012 and 2022. Rather, fluctuations in annual injuries were apparent over the study period. These fluctuations may be attributable to fluctuations in the popularity of skiing as well as variable weather conditions affecting snowfall and snow quality each season. The decrease seen between 2013 and 2016 may be a result of decreasing participation as well as increasing implementation of onsite clinics at ski resorts to address minor injuries that do not require a full ED work-up or visit.27,31,40 Furthermore, the use of injury prevention programs with safety training as well as emphasis of protective gear may have contributed to this decrease.4,20,22,31,40 The large increase in 2018 may be attributable to the 2018 ski season being the sixth busiest since 1978 despite decreasing participation in preceding years. 23 The drop in pediatric skiing injuries in 2020 likely was attributable to the COVID-19 pandemic cutting the 2020 ski season short, with many ski resorts closing during that period. The reopening of ski resorts in 2021 and 2022 and return to snow sports after the pandemic may have contributed to the increase in injuries in 2021 and 2022 compared with 2020.19,38,39
Some of the injuries experienced by the pediatric population could be explained by increased risk-taking behavior in this population. For example, some studies indicate that riskier skiers are actually more likely to wear helmets compared with those who are more cautious.12,34 This could explain the finding that while helmet usage and compliance has been increasing among the pediatric population, the rates of concussion have shown no significant downward trend over the study period despite helmets offering more protection if a skier were to fall.29,34 Furthermore, concussions have generally become a more prevalent ED complaint driven primarily by increasing youth sports participation and increasing concussion awareness.25,41
The mechanism of injury was also of interest in the current study. Impacts with the snow and ground were identified as the main mechanism of injury, making up 70% of the data. Fractures were the most common injury, making up 30% of the cases, and the lower extremity was the most common site of fracture (25% of fractures). This is in line with previous research showing that the lower limb, particularly the knee, was most at risk of injury in pediatric populations.8,28 Previous research has shown that, whereas adult injuries during skiing are more common than pediatric injuries, fractures of the lower leg specifically are more common in children than adults, which is supported by the data in this study. 8 Furthermore, we identified that one-third of injuries among pediatric skiers aged 13 years and younger were fractures, while only one-fourth of injuries among those aged 14 to 18 years were fractures. This heightened fracture risk among the younger pediatric population likely is attributable to less control, a higher center of gravity, and the role of open growth plates leading to weak points in the developing bones of growing children.17,32,35,37 Interestingly, there was a decreasing incidence of contusions/abrasions and strains/sprains. Previous studies have similarly shown that lower extremity sprains/strains and contusions/abrasions are decreasing and have also pointed out that upper extremity injuries are increasing. 16 This is thought to be due the development of better binding mechanisms between the ski and boot, which allow for better release of the foot and ankle before impact. 13 Minor injuries such as strains, sprains, contusions, and abrasions are likely able to be addressed at an onsite or outpatient clinic or with the use of protective gear, whereas more serious traumatic injuries such as fractures or concussions may be taken by ski patrol directly to the hospital for ED evaluation and additional imaging.20,27,31
Another area of particular interest in the data is that 5% of injuries occurred due to chairlifts. Chairlifts can be variable, from 2 seats to 6 seats or more per ride and can also include gondolas and other standing forms of transportation. Given that chairlifts are a method used frequently for accessing the top of the mountain, it is important that future research is focused on determining how to make this transportation safer, especially for pediatric populations. Some studies have shown that skiing in a larger group of friends or family can reduce risk of injury by around 50%, especially compared with skiing alone. 7 This shows possible risk mitigation for pediatric injury needs to fall onto parents and counselors chaperoning these trips to reduce rates of injury. Finally, ski resort chairlift models can have an impact on injury rates. One study at a particular ski resort found that chairlift injuries increased by 2-fold using only a 50% capacity increase to chairlift systems across the resort. 2 As winter sports become more popular and resorts increase lift capacities, such factors as traffic patterns, lift functioning, and overall snow accommodations will take further importance to prevent increases to injury rates.
In a 2023 study, Hurt et al 15 identified a significant decrease in skiing, snowboarding, and snowmobiling injuries reporting at US EDs between 2009 and 2018, with fractures being the most common diagnosis and boys being injured more commonly. Warren et al 40 assessed pediatric ski and snowboarding injuries from 2010 to 2022 and reported fractures as the most common diagnosis, boys as being injured more frequently, and injuries as decreasing significantly between 2010 and 2020. Although they identified a significant decrease during the study period, they also noted that ski/snowboarding injuries reported at US EDs kept steady between 2017 and 2020. In our study, we similarly identified fractures as the most common diagnosis and found pediatric skiing injuries to be more common among boys. However, we demonstrated no significant trend in injuries between 2012 and 2022, which contrasts the decline previously reported. This discrepancy in injury trends may be due largely to the higher injury rate between 2018 and 2022 compared with 2016 and 2017. Importantly, our study further identified that, whereas fractures and concussions showed no significant trend, strains/sprains and contusions/abrasions significantly decreased. With 2022 representing the highest number of pediatric skiing injuries since 2014, these findings highlight the importance of continued injury prevention efforts and may aid in injury assessment and treatment by onsite ski clinics.
Given that this study relied on ED visits through the NEISS database, it likely underestimated the total number of skiing injuries in the pediatric population. Many pediatric skiing injuries are likely treated at ski clinics or may be evaluated at urgent care clinics, pediatric offices, or in orthopaedic offices. Thus, the NEISS dataset may consist primarily of injuries that require a timely evaluation and work-up, such as fractures. Importantly, while the use of protective equipment has increased over time, 5 this study shows that more serious injuries such as fractures and concussions continue to remain prevalent with no significant decline between 2012 and 2022. Thus, we recommend increased utilization of protective gear, including helmets, as well as implementation of safety lessons and concussion prevention protocols especially for pediatric skiers.
Limitations
As this was a retrospective study that relied on information provided by the NEISS dataset, limitations are inherent. The classification of injury mechanisms depended on the narrative reported by the ED clinician. There was variability in the detail provided in these narratives that might have resulted in misinterpretation of the contributing outcome. However, only 589 cases (0.48%) of pediatric skiing injuries in this study were classified as “not specified.” Another limitation of this study is that the location of injuries was not able to be considered. Thus, it was not known what prevention measures were in place at the ski resort, the helmet/protective gear usage rate, or the onsite ski clinics or ski patrol available for a given case. We attempted to mitigate such risks by using a large national database dataset to mitigate low sample size when assessing injury trends and distribution. However, NEISS NEs are extrapolated from 100 EDs that serve as a representative sample of all US EDs, and these estimates may be off from pediatric skiing injuries nationally. Another important limitation is that specific details regarding the injury/fracture patterns as well as findings from imaging are not known. Our analysis relied on NEISS coding for the injured body part and injury diagnosis, which may not always represent the true underlying injury. Finally, the exact number of total pediatric skiers each year in the United States over the study period is not known, and this may have affected annual trends and interpretation of preventive measures of safety initiatives.
Conclusion
Between 2012 and 2022, there was no significant trend in pediatric skiing injuries reported at EDs in the United States. Impact with the snow/ground was the most common injury mechanism, making up 70.8% of all injuries. Fractures were the most common injury diagnosis followed by strains/sprains, with the lower leg being fractured most frequently. While strains/sprains and contusions/abrasions reported at US EDs showed a significant decline, fractures and concussions showed no significant trend over the study period.
Footnotes
Final revision submitted November 19, 2023; accepted December 6, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.I.H. has received nonconsulting payments from Bioventus and hospitality payments from AbbVie, AstraZeneca Pharmaceuticals, and Aesculap. K.D.P. has received education payments from Gotham Surgical; nonconsulting fees from Bioventus and Linvatec; consulting fees from Anika Therapeutics, Flexion Therapeutics, Heron Therapeutics, and Smith+Nephew; and hospitality payments from Aesculap Biologics. D.P.T. has received grant support from Arthrex and education payments from Arthrex and Smith+Nephew. R.L.P. has received grant support and education payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.