
Abstract
Background:
The effect of prior rotator cuff repair (RCR) on clinical outcomes after total shoulder arthroplasty (TSA) is unclear.
Purpose:
To systematically review the literature to compare the outcomes of TSA in patients with and without prior RCR.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was performed using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines by searching the PubMed, Cochrane Library, and Embase databases to identify studies comparing outcomes of TSA with and without prior RCR. The inclusion criteria were full-text studies that directly compared outcomes between patients undergoing anatomic or reverse TSA with and without prior RCR. A quality assessment was performed using the Modified Coleman Methodology Score (MCMS), and risk of bias assessment was performed using the Risk Of Bias In Non-randomized Studies–of Interventions (ROBINS-I) tool. A total of 1542 articles were identified for review based on initial database queries. Weighted means of quantifiable demographics and patient-reported outcomes were calculated for all included studies and compiled, in addition to the MCMS and ROBINS-I tool.
Results:
Twelve studies (10 level 3, 2 level 4) met inclusion criteria, including a total of 885 patients who underwent RCR before TSA (mean age, 68.2 years) and 2275 patients with no prior RCR (mean age, 70.0 years). Of all outcomes evaluated, patients with reverse TSA showed superior results in the no prior RCR group. Three reverse TSA studies found the no prior RCR group to have significantly higher postoperative American Shoulder and Elbow Surgeons scores when compared with the prior RCR group (P < .05). Multiple reverse TSA studies found the no prior RCR group to have significantly higher postoperative Simple Shoulder Test scores (P < .05) and significantly improved forward elevation (P < .05) when compared with the prior RCR group. Of all outcomes in anatomic TSA studies, only complication rate was different between groups, with 1 study finding a significantly lower complication rate in the no prior RCR group (P = .01).
Conclusion:
Patients undergoing reverse TSA without prior RCR can be expected to experience statistically better outcomes when compared with patients with prior RCR, while patients undergoing anatomic TSA can be expected to have similar outcomes regardless of prior RCR status.
The prevalence of total shoulder arthroplasty (TSA), both anatomic and reverse, has increased significantly in the United States over the past 2 decades. 12 Both procedures have been shown to reliably reduce pain and improve function in many types of patients.30,42 Anatomic TSA is a successful treatment for patients with glenohumeral osteoarthritis with a functioning, intact rotator cuff, 20 whereas reverse TSA is indicated and has been found to be successful in patients with massive, irreparable rotator cuff tears with or without glenohumeral arthritis, 41 among others.
Despite the success of TSA, complications are still common. 20 Predictors of poor outcomes have been studied, with prior ipsilateral shoulder surgery being identified as a predictor of negative outcomes after TSA.13,24,43,45 More specifically, the impact of prior rotator cuff repair (RCR) on the outcome of TSA remains unclear. Multiple studies have reported worse outcomes in patients with prior RCR,6,23,31,36 while others have reported similar outcomes for patients who have and have not undergone prior RCR.10,11,27 The purpose of this study was to systematically review the literature to compare the efficacy of TSA for patients with and without previous RCR. The authors hypothesized that there would be no difference in outcomes between patients undergoing TSA with and without prior RCR.
Methods
This systematic review was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines using a PRISMA checklist. Two independent reviewers (J.C.H. and J.W.B.) searched the PubMed, Embase, and Cochrane Library databases up to December 22, 2021. The electronic search strategy used was shoulder arthroplasty AND rotator cuff repair, shoulder arthroplasty AND prior rotator cuff. A total of 1542 studies were reviewed by title and/or abstract to determine study eligibility based on inclusion criteria. In cases of disagreement, a third reviewer (J.T.B.) made the final decision.
The inclusion criteria were (1) human studies that directly compared clinical and functional outcomes of patients who underwent anatomic or reverse TSA with and without prior RCR, (2) studies that were published in English, and (3) full-text articles that were published in a peer-reviewed journal. Exclusion criteria included (1) abstract and technique articles, (2) studies without a control group, (3) studies without stratified analysis for prior RCR, and (4) studies of primarily patients with RA, patients undergoing concomitant procedures, or patients undergoing revision shoulder arthroplasty or arthroplasty for fracture repair. Data extraction from each study was performed independently (J.C.H.) and then reviewed by a second author (J.W.B). There was no need for funding or a third party to obtain any of the collected data.
Risk of bias was assessed according to the Risk Of Bias In Non-randomized Studies–of Interventions (ROBINS-I) tool, 39 which incorporates an assessment of bias due to confounding, selection of participants, deviations from intended interventions, completeness of outcome data, selection of outcomes reported, and other sources of bias.
Reporting Outcomes
Outcomes assessed included patient-reported outcomes (PROs), postoperative functional evaluations, and complication rates. PROs included the American Shoulder and Elbow Surgeons (ASES) score, 29 Constant-Murley score, 5 Shoulder Pain And Disability Index (SPADI), 2 Simple Shoulder Test (SST) score, 19 and University of California Los Angeles (UCLA) score. 1 Postoperative functional evaluations included range of motion (ROM), complications, and revisions. Eight studies6,10,11,23,26,27,34,36 used the ASES score, 4 studies23,27,31,34 used the Constant-Murley Score, 3 studies23,27,34 used the SPADI score, 6 studies6,8,23,27,33,34 used the SST score, and 4 studies23,27,31,34 used the UCLA score. A total of 6 studies6,23,26,27,34,36 assessed ≥1 postoperative ROM metric, and 6 studies6,23,27,33,34,36 reported on complications and/or revisions for both groups.
All studies reported outcomes using 2 groups: patients with no prior RCR and patients with prior RCR. One reverse TSA study 23 further subcategorized patients into those undergoing shoulder arthroplasty for glenohumeral osteoarthritis and those undergoing shoulder arthroplasty for cuff tear arthropathy. Results were stratified based on whether patients underwent anatomic or reverse TSA.
Study Methodology Assessment
The Modified Coleman Methodology Score (MCMS) 4 was used to evaluate study methodologic quality. The MCMS has a scaled potential score ranging from 0 to 100. Scores of 85 to 100 were classified as excellent; 70 to 84, as good; 55 to 69, as fair; and <55, as poor.
Statistical Analysis
Weighted means were calculated for numerical demographics (age, follow-up, and sex percentage) and PROs (ASES, Constant-Murley, SPADI, SST, and UCLA scores).
Results
Twelve studies met the inclusion and exclusion criteria (Figure 1), ‡ including a total of 3160 patients (prior RCR, n = 885; no prior RCR, n = 2275). The mean patient age at time of surgery was 68.2 years (range, 52-88 years) and 70.0 years (range, 52-88 years) in the prior RCR and no prior RCR groups, respectively. The mean follow-up was 43.2 months in the prior RCR group and 40.3 months in the no prior RCR group. The overall percentage of men was 38.7% and 42.2% in the no prior RCR and prior RCR groups, respectively (Table 1). Patients underwent RCR at a mean of 35 months before reverse TSA (range, 3-120 months), and no anatomic TSA studies reported timing of prior RCR.

A flow diagram of the authors’ electronic search strategy after PRISMA guidelines. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RA, rheumatoid arthritis; RCR, rotator cuff repair.
Studies Included With Level of Evidence, Type of TSA, and Prior RCR or No Prior RCR a
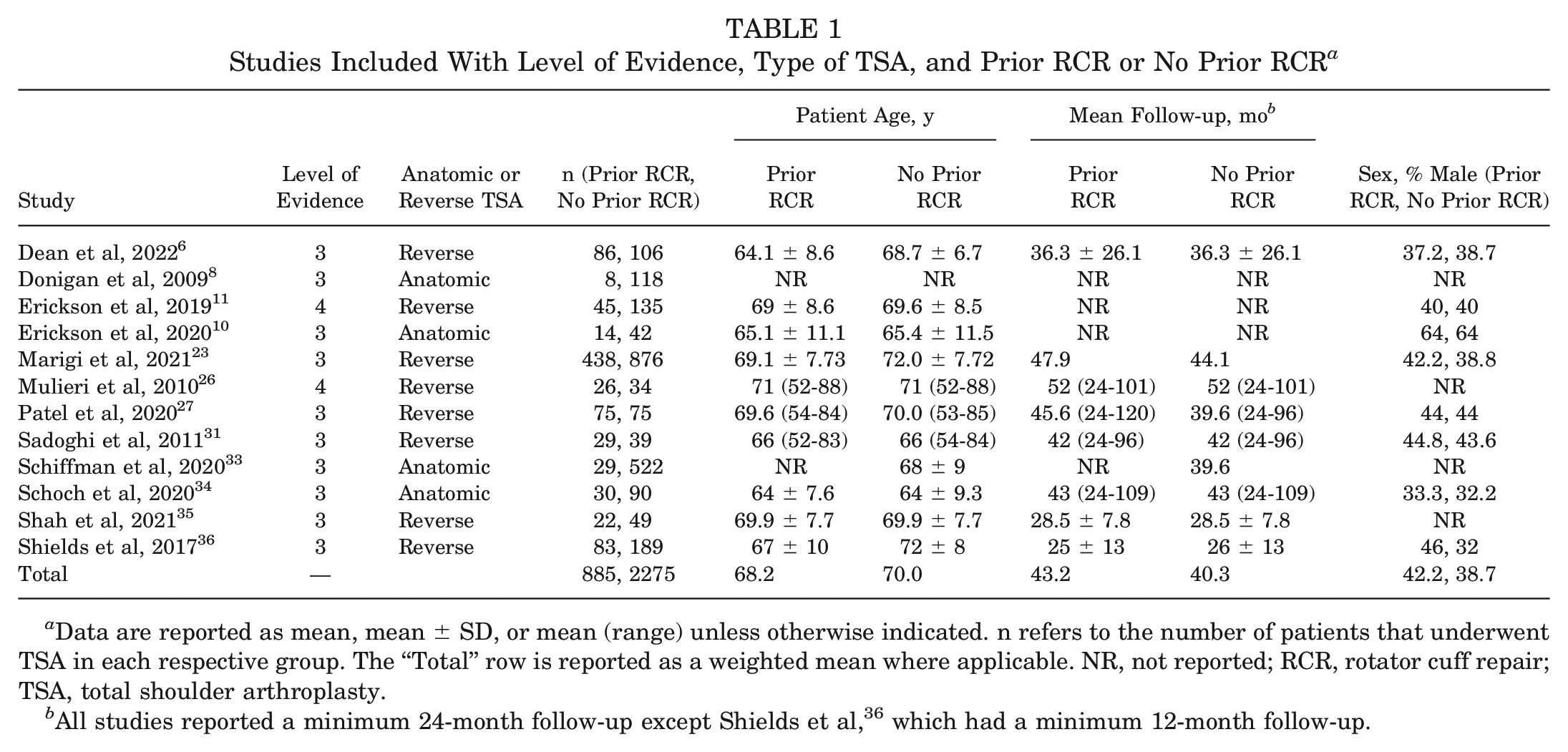
Data are reported as mean, mean ± SD, or mean (range) unless otherwise indicated. n refers to the number of patients that underwent TSA in each respective group. The “Total” row is reported as a weighted mean where applicable. NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
All studies reported a minimum 24-month follow-up except Shields et al, 36 which had a minimum 12-month follow-up.
Surgical Technique
Eight studies6,11,23,26,27,31,35,36 in this review used reverse TSA as the primary procedure, while 4 studies used anatomic TSA.8,10,33,34 When described, there was significant heterogeneity in surgical technique within any individual procedure, though a majority of the studies did not include a detailed description of surgical technique.
Postoperative Rehabilitation
Similarly, postoperative rehabilitation protocols were heterogeneous and poorly described. The most common protocol included 6 weeks of postoperative shoulder immobilization and passive ROM exercises,26,27,31,35 followed by 6 weeks of active-assisted ROM exercises with immobilization only when away from home.26,27 Return to full weightbearing activity was permitted after 12 weeks.26,27,31 At 6 months postoperatively, patients were allowed to participate in any activity based on comfort and confidence levels.
Modified Coleman Methodology Score
Table 2 shows the MCMSs from the 12 included studies. Nine studies6,8,11,23,26,31,34-36 received fair scores and 3 studies10,27,33 received poor scores.
Modified Coleman Methodology Score (MCMS)

Demographics
Two studies6,36 reported a significant difference in age between the no prior RCR and prior RCR study groups, with the prior RCR group being significantly younger in both (P < .001). One study 36 reported a significant difference in sex between the 2 groups, with the prior RCR group having significantly more men (P = .033). Multiple studies reported no difference in sex,6,10,11,23,27,31,34 body mass index,6,23,34,36 age,10,11,23,27,31,34 or height.23,31,34
Methodological Quality Assessment
The results of the methodologic quality assessment of the 12 nonrandomized studies using the ROBINS-I tool are presented in Figure 2. All 12 studies showed a moderate risk of bias due to confounding, as there were no prognostic variables that predicted baseline intervention and no patients who switched between interventions during the study period. No studies excluded eligible patients or used variable follow-up times based on intervention (low risk of bias), no studies deviated from the intended intervention (low risk of bias), and all studies clearly classified treatment type (low risk of bias). All 12 studies used nonblinded but identical postoperative protocols between groups (moderate risk of bias). Due to either the retrospective methodology or the nature of intervention, all 12 studies used physicians unblinded to treatment group (high risk of bias). No studies showed bias due to missing data (low risk of bias). Finally, no studies showed bias due to selective reporting (low risk of bias). A Cohen kappa score of 0.87 reflected a very good agreement between reviewers. 25

Bar graph presenting risk of bias as a percentage across all included studies (green, low risk; yellow, unclear; red, high risk).
Patient-Reported Outcomes
Three of the 6 reverse TSA studies (4 study groups)6,23,36 reporting on ASES scores found the no prior RCR group to have significantly higher postoperative scores when compared with the prior RCR group (P < .05) (Table 3). Two of the 3 reverse TSA studies (3 of the 4 study groups)23,36 that compared improvement in ASES scores found the no prior RCR group to have significantly higher improvement from preoperatively to postoperatively when compared with the prior RCR group (P < .05). No significant differences were observed between groups in the anatomic TSA studies.
American Shoulder and Elbow Surgeons Scores a

Scores are reported as mean ± SD or mean (95% CI), with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
One of the reverse TSA studies (2 study groups) 23 reporting on Constant-Murley scores found the no prior RCR group to have significantly higher postoperative scores and significantly higher percentage improvement in scores from preoperatively to postoperatively when compared with the prior RCR group (P < .05) (Table 4). No significant differences were observed between groups in the single anatomic TSA study reporting on Constant-Murley score.
Constant-Murley Scores a

Scores are reported as mean ± SD or mean (range), with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
One of the 2 reverse TSA studies (2 of the 3 study groups) 23 reporting on SPADI scores found the no prior RCR group to have significantly higher postoperative scores and significantly higher percentage improvement in scores from preoperatively to postoperatively when compared with the prior RCR group (P < .05) (Table 5). No significant differences were observed between groups in the single anatomic TSA study reporting on SPADI score.
Shoulder Pain and Disability Index Scores a
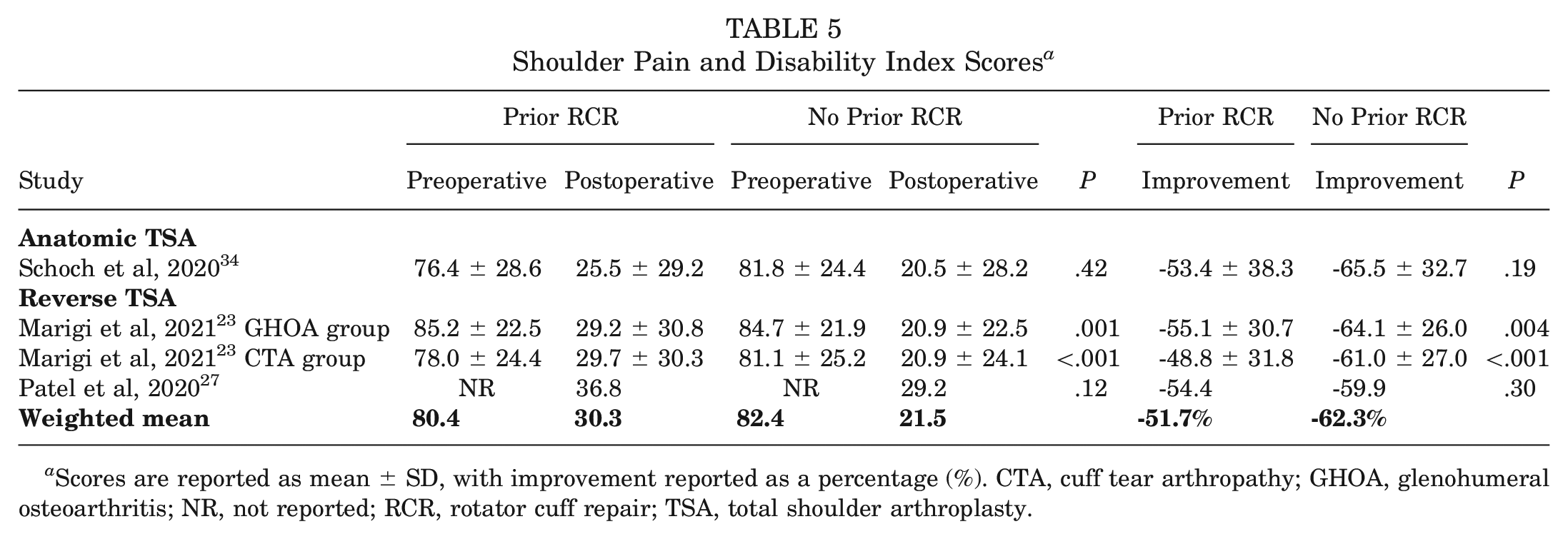
Scores are reported as mean ± SD, with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
Two of the 3 reverse TSA studies (3 of the 4 study groups)6,23 reporting on SST scores found the no prior RCR group to have significantly higher postoperative scores when compared with the prior RCR group (P < .05) (Table 6). One reverse TSA study (2 study groups) 23 also found the no prior RCR group to have significantly higher percentage improvement in SST score from preoperatively to postoperatively when compared with the prior RCR group (P < .001). No significant differences were observed between groups in the anatomic TSA studies.
Simple Shoulder Test Scores a
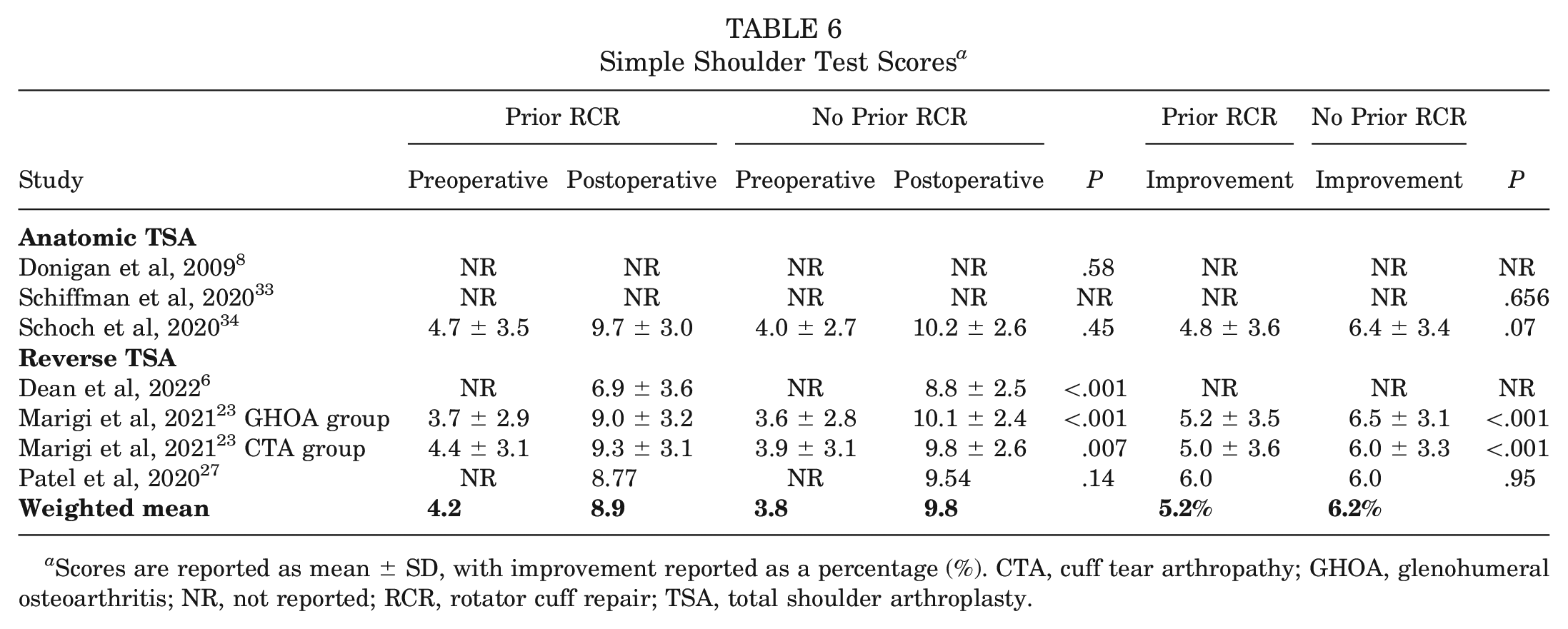
Scores are reported as mean ± SD, with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
One of the 3 reverse TSA studies (2 study groups) 23 reporting on UCLA scores found the no prior RCR group to have significantly higher postoperative scores and significantly higher percentage improvement in UCLA score when compared with the prior RCR group (P < .001) (Table 7). No significant differences were observed between groups in the single anatomic TSA study reporting on UCLA score.
UCLA Shoulder Scores a

Scores are reported as mean ± SD or mean (range), with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty; UCLA, University of California Los Angeles.
Functional Outcomes
Range of Motion
None of the anatomic or reverse TSA studies that reported on active abduction found a significant difference between the prior RCR and no prior RCR groups postoperatively. One reverse TSA study (2 study groups) 23 found a significantly greater improvement in active abduction in the no prior RCR group compared with the prior RCR group (P = .001) (Table 8).
Active Abduction a

Values are reported in degrees as mean ± SD, with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
Two reverse TSA studies (3 study groups)6,23 that reported on active forward elevation found the no prior RCR group to have significantly higher postoperative scores when compared with the prior RCR group (P < .05) (Table 9). Additionally, 2 reverse TSA studies (3 study groups)23,36 found a significantly greater improvement in active forward elevation in the no prior RCR group compared with the prior RCR group. No significant differences were noted in the single anatomic TSA study that reported on active forward elevation.
Active Forward Elevation a

Values are reported in degrees as mean ± SD or mean (95% CI), with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
None of the anatomic or reverse TSA studies that reported on active external rotation found a significant difference between the prior RCR and no prior RCR groups postoperatively. One reverse TSA study (2 study groups) 23 found a significantly greater improvement in active external rotation in the no prior RCR group (P≤ .001) (Table 10).
Active External Rotation a
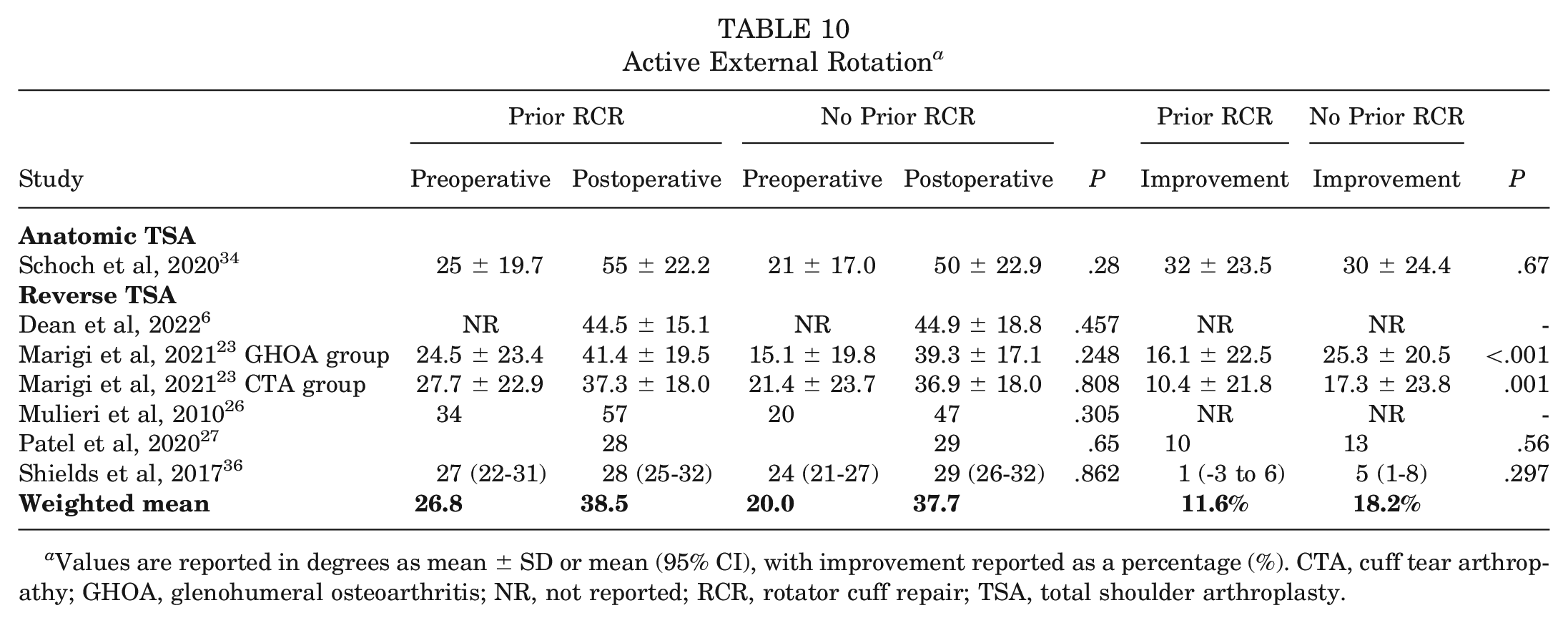
Values are reported in degrees as mean ± SD or mean (95% CI), with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
None of the anatomic or reverse TSA studies that reported on internal rotation scores found a significant difference between the prior RCR and no prior RCR groups postoperatively. One reverse TSA study (2 study groups) 23 found a significantly greater improvement in internal rotation score in the no prior RCR group (P < .001) (Table 11).
Internal Rotation Scores a
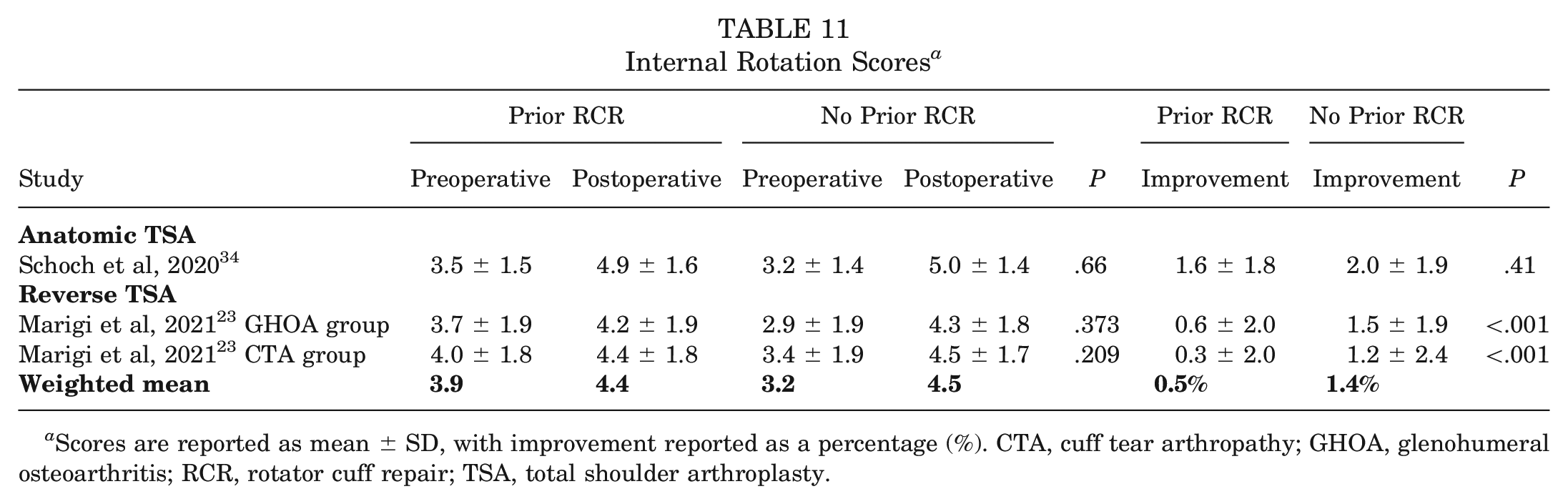
Scores are reported as mean ± SD, with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
One reverse TSA study (2 study groups) 23 found the no prior RCR group to have significantly higher postoperative strength and significantly higher percentage improvement in strength when compared with the prior RCR group (P < .05) (Table 12).
Strength of Forward Elevation a

Values are reported in kg as mean ± SD or mean, with improvement reported as a percentage (%). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
Complications and Revisions
One of the 4 reverse TSA studies 6 and 1 of the 2 anatomic TSA studies 34 that reported on complication rates found the no prior RCR group to have significantly fewer complications when compared with the prior RCR group (P < .05) (Table 13). No study found a significant difference in revision rates between groups (P > .05).
Total Complications and Revisions in Anatomic and Reverse TSA Studies a

Complications are reported as number of complications (% of total number of patients). Revisions are reported as number of revisions (% of total number of patients). CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; NR, not reported; RCR, rotator cuff repair; TSA, total shoulder arthroplasty. Dashes indicate value not calculated.
Survivorship
Two reverse TSA studies26,31 (3 study groups) reported on survivorship. Mulieri et al 26 reported a mean survivorship of 91.8 months (95% CI, 86.1-97.5 months) in the no prior RCR group and 75.6 months (95% CI, 67.2-84.1 months) in the prior RCR group, with removal or revision of a component, radiographic loosening, or declining ASES score as end points. Sadoghi et al 31 reported a cumulative overall 5-year survival of 67.5% (95% CI, 30%-105%) with no significant difference in survival between the prior RCR and no prior RCR groups, with any complication, revision, or infection as end points.
Discussion
The results of this systematic review suggest that patients with no prior RCR undergoing reverse TSA experience statistically better outcomes and that patients with no prior RCR undergoing anatomic TSA experience statistically similar outcomes when compared with patients who have undergone prior RCR. Of the 12 studies in this review, 8 studies6,11,23,26,27,31,35,36 reported outcomes for patients with prior RCR after reverse TSA (n = 804) and 4 studies8,10,33,34 reported outcomes after anatomic TSA (n = 81). Of all patient outcomes assessed (ASES, Constant-Murley, SPADI, SST, UCLA, ROM, complications, revisions), none demonstrated superiority in the prior RCR group, whereas numerous reverse TSA outcomes demonstrated significantly better results in the no prior RCR group. Reverse TSA studies reported significantly better postoperative ASES scores (Table 3),6,23,36 Constant-Murley scores (Table 4), 23 SPADI scores (Table 5), 23 SST scores (Table 6),6,23 UCLA scores (Table 7), 23 active forward elevation (Table 9),6,23 strength of forward elevation (Table 12), 23 and lower complication rates (Table 13) 6 in the no prior RCR group (P < .05). Of all anatomic TSA outcomes assessed, only complication rate was different between groups, with 1 study reporting a significantly lower complication rate 34 (Table 13) in the no prior RCR group (P < .05).
With cuff retear rates varying significantly depending on RCR technique 18 and the demonstrated success of reverse TSA in patients with irreparable rotator cuff tears, 26 reverse TSA may achieve better outcomes in these patients. Additionally, there may be hesitancy to perform anatomic TSA in patients with prior rotator cuff pathology given the poor results of RCR after anatomic TSA should a cuff retear occur. 17 Regardless, the findings in this review suggesting no difference in reported outcomes for patients undergoing anatomic TSA with or without prior RCR and inferior outcomes for patients undergoing reverse TSA after previous RCR cannot be ignored.
Previous studies have demonstrated inferior outcomes of TSA in patients with prior ipsilateral shoulder surgery.13,24,37 Frank et al 13 found that numerous outcome scores after TSA were significantly worse in the prior surgery group, and these differences persisted in both the anatomic TSA and the reverse TSA subanalyses. Simmen et al 37 reported a significant reduction in probability of success after TSA in patients with previous operations, while Matsen et al 24 found that no previous shoulder surgery was associated with a significantly better outcome after TSA. These results are consistent with the conclusions of our review in that no subset of patients who underwent prior RCR had superior postoperative outcomes after TSA compared with those who did not.
Variable results have been reported on RCR as an independent predictor of poor outcomes after TSA. Shields et al 36 found that previous RCR was a significant independent predictor for lower postoperative ASES and Simple Shoulder Value scores; higher postoperative pain; and less improvement in ASES score, Simple Shoulder Value score, pain, and forward elevation ROM. Frank et al 13 reported similar outcomes irrespective of the prior surgery type, specifically noting no difference between prior RCR and other procedures. Shah et al 35 found that previous RCR was not an independent factor in lower postoperative patient satisfaction at 2-year follow-up.
One proposed mechanism for inferior functional and ROM outcome scores after TSA in patients with prior RCR is the presence of an altered deltoid muscle. Cho et al 3 demonstrated that deltoid atrophy and/or partial deltoid detachment may occur after open and arthroscopic RCR. Multiple studies have shown larger preoperative deltoid size44,46 to be a predictive factor of improved postoperative outcome scores after reverse TSA and deltoid atrophy15,44 to be a negative predictive factor of postoperative outcome scores after reverse TSA. This may partially explain the findings in this review.
Similarly, fatty infiltration and atrophy of the rotator cuff muscles may contribute to TSA outcomes. It is controversial whether these sequelae improve, stabilize, or persist after RCR7,16; however, they have been associated with poorer outcomes after RCR.14,21 In TSA, rotator cuff atrophy and fatty infiltration have been associated with postoperative strength and Constant-Murley score, 22 abduction strength, 32 and development of secondary rotator cuff dysfunction. 47 Other studies9,28 have not found any association between rotator cuff atrophy and fatty infiltration and TSA outcomes. This may be another contributing factor to the worse outcomes of TSA with prior RCR reported in this review; however, this would likely contribute more to worse outcomes in patients undergoing anatomic TSA given its reliance on an intact rotator cuff.
Another important consideration for the results in this study is the overall improvement in PROs in both the prior RCR and the no prior RCR groups, despite the significantly worse outcomes in the prior RCR group when compared with the no prior RCR group postoperatively. In a systematic review by Su et al, 40 minimal clinically important differences (MCIDs) in the reported outcome measures after TSA were 16.0 for ASES, 6.3 for Constant-Murley, and 2.9 for SST scores. Additionally, Simovitch et al 38 reported the MCIDs after TSA as 8.7 for UCLA and 20.6 for SPADI scores. Both studies used anchor-based methods to compile MCIDs and included both patients with reverse and anatomic TSA. All the MCIDs were met by both groups across all 5 of these outcome measures in this study. Therefore, the clinical relevance of the statistically better outcomes in the no prior RCR group for patients undergoing TSA is unclear.
Strengths and Limitations
The strengths of this study include a comprehensive systematic review performed by 2 independent reviewers. The limitations should also be noted. Of the 12 studies included in this review, none provided level 1 or level 2 evidence. Methodological assessment showed significant heterogeneity and fair to poor overall quality of the studies, which prohibited calculation of the I 2 statistic, completion of forest plots, and meta-analysis. Only 3 studies6,31,33 reported timing of prior shoulder surgery, with only 2 of these studies6,31 (both reverse TSA) reported the timing of prior RCR specifically. There were differences in surgical techniques and rehabilitation protocols between studies, and many studies did not describe either in detail. Follow-up times were highly variable, ranging from 12 to 120 months.
Conclusion
Patients undergoing reverse TSA without prior RCR can be expected to experience statistically better outcomes when compared with patients with prior RCR, while patients undergoing anatomic TSA can be expected to have similar outcomes regardless of prior RCR status.
Footnotes
Final revision submitted September 30, 2023; accepted November 13, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.K.M. has received hospitality payments from Stryker, Arthrosurface, and Medical Device Business Services and compensation for services other than consulting from Arthrosurface. R.M.F. has received consulting fees from Arthrex and compensation for services other than consulting from Arthrex; education payments from Arthrex, Gemini Mountain Medical LLC, and Pinnacle; and hospitality payments from Gemini Mountain Medical LLC, Joint Restoration Foundation, Smith+Nephew, Arthrex, and Stryker. A.J.S. has received consulting fees from Encore Medical and Medacta USA, honoraria from Encore Medical, and education payments from Arthrex. E.C.M. has received consulting fees from DePuy Synthes Products, Medical Device Business Services, Pacira Therapeutics, and Zimmer Biomet Holdings; royalty or license from Zimmer Biomet Holdings; education payments from Gemini Mountain Medical LLC; and compensation for services other than consulting from Arthrex. J.T.B. has received consulting fees from Encore Medical and Smith+Nephew, compensation for services other than consulting from Smith+Nephew, and education payments from Smith+Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.