
Abstract
Background:
The posterior tibial slope (PTS) is an important feature in knee joint biomechanics and indicates anterior-posterior knee stability. Increased PTS is a known risk factor for both primary anterior cruciate ligament (ACL) rupture and postreconstruction rerupture.
Purpose:
To investigate the effect of long-term exposure to ACL deficiency on the PTS and the sagittal anatomy of the proximal tibia.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 44 patients (38 men, 6 women) with a history of knee injury and ACL rupture confirmed by magnetic resonance imaging and physical examination were included in this study. Patients were divided into those with chronic ACL deficiency (group 1: injured ≥5 years prior; n = 22) and acute ACL deficiency (group 2: injured <1 year prior; n = 22). The medial and lateral tibial plateau PTS and anterior tibial translation were measured on monopodal weightbearing knee radiographs at 20° of flexion. The mechanical tibiofemoral angle (MTFA) and the medial proximal tibial angle (MPTA) were measured using an orthoroentgenogram. The side-to-side difference between the affected and unaffected knees was also calculated for all measurements.
Results:
The mean duration of exposure to ACL deficiency was 7.6 years (range, 5-15 years) in group 1 and 4.4 months (range, 1-11 months) in group 2. Regarding the side-to-side differences in angular measurements, a higher medial PTS (affected vs unaffected: 12.4° vs 10.1°; P = .007), higher lateral PTS (11° vs 8.9°; P = .011), and increased varus alignment on both the MTFA (4.3° vs 2.4°; P = .036) and the MPTA (84.9° vs 86.3°; P = .033) were found in group 1, while no significant differences in angular measurements were found in group 2. Compared with group 2, patients in group 1 had a significantly higher side-to-side difference in the medial PTS (2.3° vs 0.1°; P = .0001), lateral PTS (2.1° vs 0.4°; P = .0001), and MPTA (1.4° vs 0.1°; P = .002).
Conclusion:
This study showed that the affected knees of patients with chronic ACL deficiency (≥5 years) had higher medial and lateral PTS compared with the unaffected contralateral knees. Therefore, when planning ACL reconstruction for patients with a history of long-term ACL deficiency, it is crucial to measure the preoperative PTS accurately.
Keywords
Failure after anterior cruciate ligament (ACL) reconstruction (ACLR) mostly develops due to various technical and anatomic risk factors.12,13,27,28 There is a great interest in the effect of anatomic factors. These include knee hyperextension, varus malalignment, and increased posterior tibial slope (PTS), particularly lateral PTS.4,5,18 Among these risk factors, increased PTS creates shear forces on the tibiofemoral surfaces that will force the tibia anteriorly, resulting in increased strain on the ACL graft. 25 The impact of high PTS on graft failure after ACLR is significant in the literature.6,10,14 The PTS has also been shown to be a risk factor for primary ACL rupture with a noncontact injury. Beynnon et al 2 found a 21.7% increased risk of ACL injury with every increase in the degree of the lateral PTS.
Although the literature has focused on the effect of the PTS on the risk of ACL rupture or rerupture, the opposite question, “What is the effect of long-term exposure to ACL deficiency on the sagittal anatomy of the proximal tibia?” has not yet been examined. It has been shown in the literature that long-term exposure to ACL deficiency may lead to varus deformity in the coronal plane; nonetheless, a similar change in the sagittal plane has not yet been demonstrated. 9
This study aimed to investigate whether the PTS and sagittal anatomy of the proximal tibia change over time in unoperated ACL-deficient knees. We hypothesized that long-term exposure to ACL deficiency would increase the PTS compared with the contralateral side.
Methods
After obtaining institutional review board approval, we included patients presenting to our outpatient clinics with an acute or chronic ACL injury without a ligament reconstruction between 2020 and 2022. The first group included patients who had sustained an ACL injury at least 5 years prior (chronic ACL deficiency group), and the second group included those who had sustained an ACL injury within the past year (acute ACL deficiency group). Patients with injury times between 1 and 5 years were not included. Orthoroentgenograms and radiographs of both the affected and contralateral sides were viewed. The ligamentous stability of both knees was assessed by physical examination.
The inclusion criteria were as follows: (1) age between 16 and 55 years; (2) a magnetic resonance imaging view confirming the rupture of the ACL at the time of the injury; and (3) properly viewed lateral radiographs (<6 mm of offset between the posterior halves of the medial and lateral femoral condyles).3,26 The exclusion criteria were as follows: (1) trauma or surgery history on the contralateral knee; (2) any noted sign of instability in the contralateral knee; and (3) a concomitant collateral ligament, posterolateral or posteromedial corner, or posterior cruciate ligament injury on the affected side. Initially, 67 patients from the chronic ACL deficiency group and 28 patients from the acute ACL deficiency group were identified; however, the final sample size was 22 for each group because of the inclusion and exclusion criteria (Figure 1).
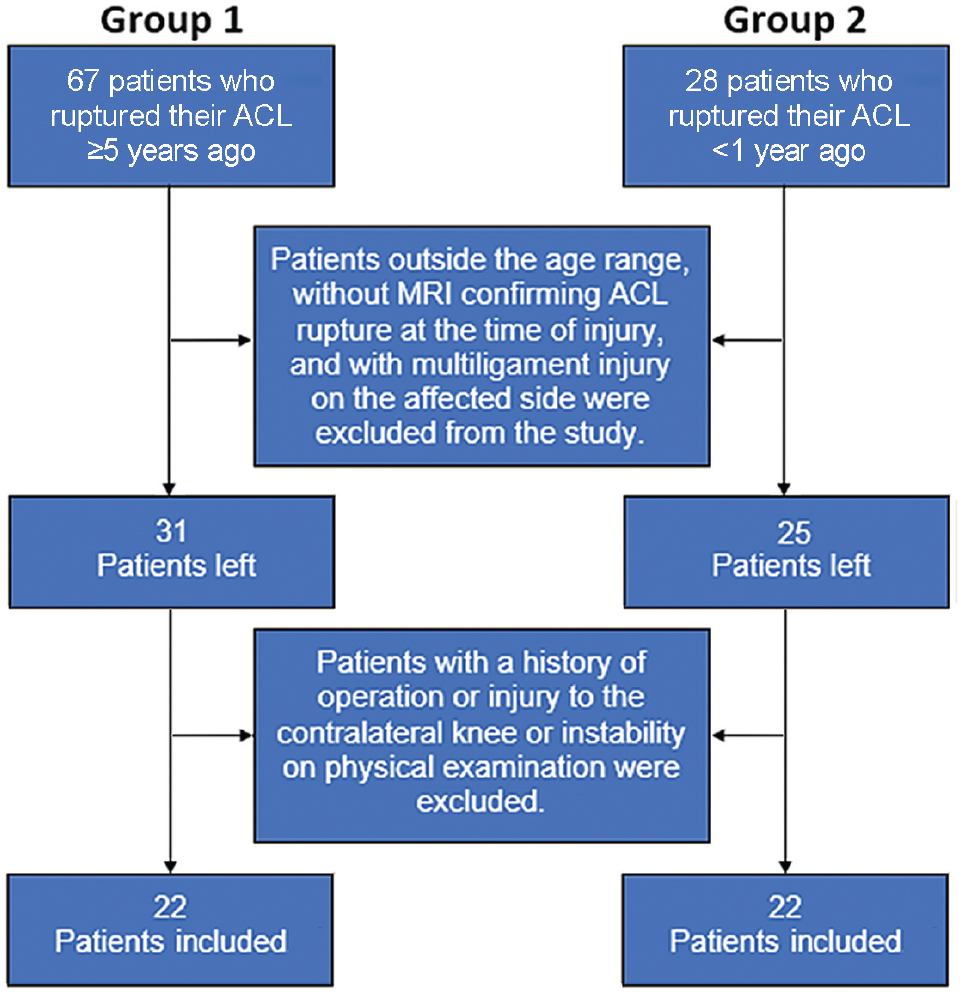
Flowchart of the enrollment process for the study groups. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
Radiographic Evaluation
The PTS of the lateral and medial tibial plateaus and the anterior tibial translation (ATT) were measured on monopodal weightbearing and 20° of flexion lateral radiographs. The PTS was measured separately for each tibial plateau and was calculated as the angle between the line formed by the anterior and posterior edges of each tibial plateau and the line perpendicular to the tibial axis (Figure 2). The tibial diaphyseal axis was formed by the union of the diaphyseal center points at 6 and 16 cm below the tibial plateau, as described by Dejour and Bonnin 8 and Faschingbauer et al. 11 The ATT, the distance between the 2 lines parallel to the posterior tibial cortex—the first of which is tangent to the posterior aspect of the medial proximal tibial plateau and the second of which is tangent to the posterior femoral condyles— was measured on the lateral monopodal weightbearing radiographs according to the method by Dejour and Bonnin 8 (Figure 3). In addition, to determine whether a deformity had developed in the coronal plane, the mechanical tibiofemoral angle (MTFA) and the medial proximal tibial angle (MPTA) were measured using an orthoroentgenogram (Figure 4). Finally, the side-to-side difference in the PTS, ATT, MTFA, and MPTA was calculated as the value of the unaffected knee subtracted from that of the affected knee.

A lateral monopodal weightbearing radiograph of a 39-year-old male patient who sustained an ACL tear 10 years prior. (A) The medial PTS angle is measured by the angle between the red line perpendicular to the tibial axis (yellow solid line) (defined as the line passing through two points, both equidistant from the anterior and posterior tibial cortex, 6 cm and 16 cm from the tibial plateau (yellow dashed lines respectively)) and the tangent to the anterior and posterior edges of the medial tibial plateau (blue line). (B) The lateral PTS was measured using the same method but tangent to the anterior and posterior edges of the lateral tibial plateau (orange line). ACL, anterior cruciate ligament; PTS, posterior tibial slope.

The ATT, the distance between the 2 lines parallel to the posterior tibial cortex—the first tangent to the posterior aspect of the medial proximal tibial plateau (red) and the second tangent to the posterior femoral condyles (yellow)—was measured on a lateral monopodal weightbearing radiograph. An ATT of 8 mm was measured in a 27-year-old male patient with a history of ACL deficiency for 9 years. ACL, anterior cruciate ligament; ATT, anterior tibial translation.

An orthoroentgenogram of a 27-year-old male patient with a history of left knee ACL injury for 5 years. The MTFA angles (between yellow lines in the left extremity and green lines in the right extremity), the MPTA angles (between lines parallel to the tibial plateau that are red on the left and yellow on the right side and tibial axis lines that are yellow on the left and green on the right side) were measured for both sides. More prominent varus alignment (MTFA: 5.20° vs 0.4°; MPTA: 84.92° vs 87.11°) was noted on the affected side. ACL, anterior cruciate ligament; MPTA, medial proximal tibial angle; MTFA, mechanical tibiofemoral angle.
All measurements were made by 2 observers, an orthopaedic surgeon and a radiologist (S.S.E.), and interobserver reliability was evaluated.
Statistical Analysis
The sample size power analysis was conducted based on a previous study by Macchiarola et al. 20 The sample size was determined based on the following parameters: a desired difference in a PTS of 2°, a desired power level of 0.95, and an alpha error of .05. The analysis results indicated that a sample size of 22 participants for each group would be sufficient to detect the specified difference.
Data were reported as mean ± standard deviation. The normal distribution of the side-to-side difference between the angular measurements was verified using the Kolmogorov-Smirnov test; however, the ATT measurement was found to have a nonparametric distribution. An independent samples t test was used to compare groups and sides regarding angular measurements, whereas the Mann-Whitney U test was used for demographic characteristics and ATT measurements. All statistical analyses were performed using SPSS 26.0 (IBM Corp). A Spearman correlation analysis was used to evaluate the relationship between side-to-side differences in PTS with patient age, patient weight, exposure time, and ATT.
The reliability of the measurements (PTS, ATT, MPTA, and MTFA) between the orthopaedic surgeon and the radiologist was calculated using the intraclass correlation coefficient (ICC) and an absolute agreement 2-way mixed-effects model.
Results
The characteristics of the study groups are shown in Table 1. The patients in the chronic ACL deficiency group were significantly older than those in the acute ACL deficiency group (mean age, 40.1 vs 27.3 years, respectively; P = .002). A total of 18 patients in group 1 had sustained their ACL injuries while playing soccer. The mean exposure time from the ACL rupture episode to the measurement time was 7.6 years (range, 5-15 years) in the chronic ACL deficiency group, compared with 4.4 months (range, 1-11 months) in the acute ACL deficiency group. Table 2 shows the interobserver reliabilities of the radiographic measurements. All ICCs were above 0.85, suggesting excellent agreement between the 2 observers.
Characteristics of the Study Groups a

Data are reported as mean ± SD (range) or n. ACL, anterior cruciate ligament.
Interobserver Reliability of the Radiographic Measurements a

ATT, anterior tibial translation; ICC, intraclass correlation coefficient; MPTA, medial proximal tibial angle; PTS, posterior tibial slope; MTFA, mechanical tibiofemoral axis.
The radiographic measurements are summarized in Table 3. Patients in both groups had significant side-to-side differences in ATT (P = .0001 for both). Regarding the side-to-side difference in angular measurements, a higher medial PTS (12.4° vs 10.1°; P = .007), a higher lateral PTS (11° vs 8.9°; P = .011), and increased varus alignment on both the MTFA (4.3° vs 2.4°; P = .036) and the MPTA (84.9° vs 86.3°; P = .033) were found in the chronic ACL deficiency group. When comparing the side-to-side difference measurements between the groups, significant differences were found in medial PTS (2.3° vs 0.1°; P = .0001), lateral PTS (2.1° vs 0.4°; P = .0001), and MPTA (1.4° vs 0.1°; P = .002) (Table 3). In the context of the 2 groups, there was no significant disparity in the mean medial and lateral PTS observed in the affected knees; however, when comparing the unaffected knees, the mean medial and lateral PTS in the chronic ACL deficiency group were significantly lower compared with those in the acute ACL deficiency group (P = .012 and .029, respectively) (Table 3).
Radiographic Measurements According to Study Group a

Data are reported as mean ± SD. Bold P values indicate statistically significant differences (P < .05). ACL, anterior cruciate ligament; ATT, anterior tibial translation; MTFA, mechanical tibiofemoral axis; MPTA, medial proximal tibial angle; PTS, posterior tibial slope; SSD, side-to-side difference.
Osteophyte formation over the posteromedial border of the tibial plateau on the lateral radiograph was observed in almost all (19 of 22) affected knees in the chronic ACL deficiency group. In the acute ACL deficiency group, a similar osteophyte was seen in only 1 patient (Figure 5).
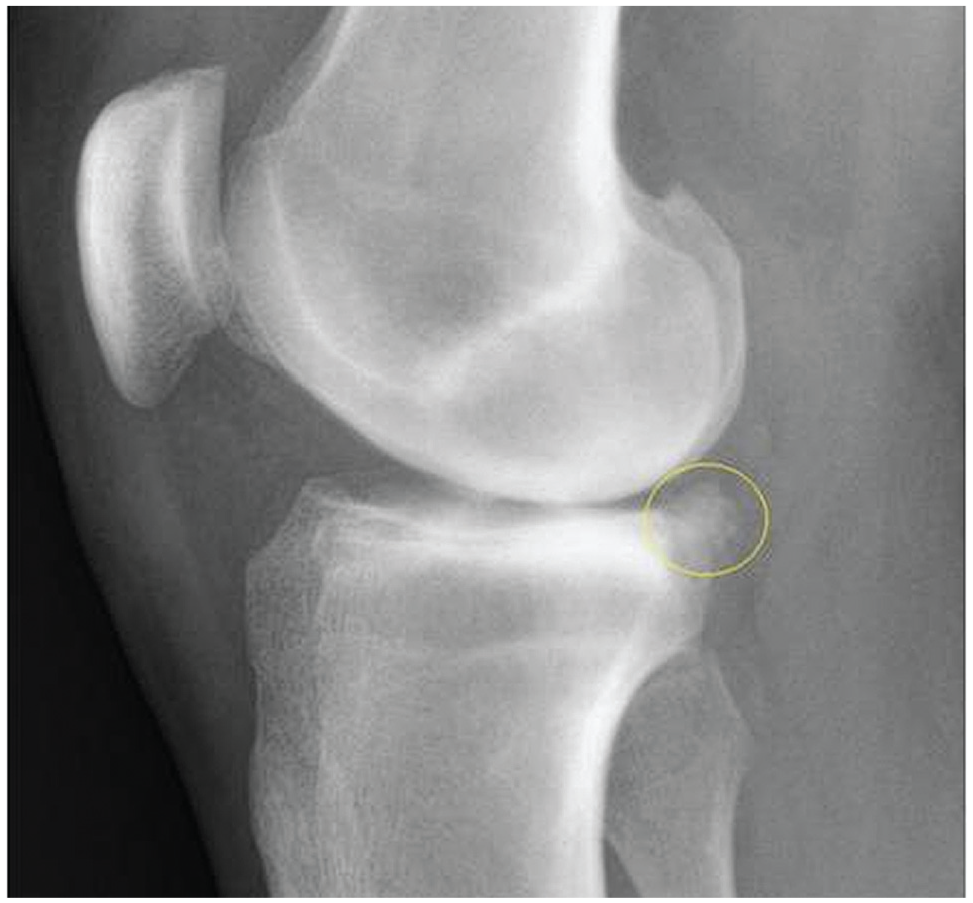
A prominent osteophyte over the posteromedial border of the tibial plateau (circled) on a lateral radiograph of a 27-year-old male patient with ACL deficiency for 9 years. ACL, anterior cruciate ligament.
The results of the correlation analysis indicated no discernible association between the medial and lateral PTS with patient age, weight, exposure duration, or ATT (P > .05 for all) (see the Supplemental Material, available separately).
Discussion
The most important finding of this study was that exposure to ACL deficiency for ≥5 years was associated with an increase in both the medial and lateral PTS compared with the unaffected side. Body mass index, exposure time, and ATT on monopodal weightbearing radiographs did not correlate with the PTS change.
Decompensation in the sagittal plane and its consequences after an ACL injury have been discussed from different perspectives in the literature. 17 The association of increased ATT with the chronicity of ACL rupture was reported previously.20,22,29 In a 2022 study, Macchiarola et al 20 compared the ACL-deficient knees of their patients with the unaffected side and found that exposure for >4 years and the presence of meniscal injury were associated with a higher ATT on monopodal weightbearing lateral radiographs. A comparison of PTS measurement with the contralateral intact knee was also questioned, and the mean PTS was 0.6° higher in the ACL-deficient knee (10.2° vs 9.6°) without a significant difference. However, the duration of exposure was not considered while comparing those results. Our study suggests a potential association between long-term ACL deficiency and increased PTS compared with the contralateral side. However, it is important to clarify that our study design did not allow us to establish a definitive causal relationship between prolonged ACL deficiency and gradual changes in PTS. Further research with a different study design may provide deeper insights into these associations.
Increased ATT, due to chronic ACL deficiency, causes more load on the posterior tibial plateau during walking cycles.1,19 A posteriorly displaced contact surface of the femoral condyle over the tibial articular surface may increase mechanical stress over the posterior edge of the tibial plateau. Dejour et al 9 noticed that condylar impacts result in the development of the posterior osteophyte and the gradual transformation of the medial tibial plateau into a concave shape over time in their study on patients with osteoarthritis after ACLR. Considering our findings, this morphological change over the tibial plateau may result in a sagittal bone deformity that could lead to an increase in the PTS. However, it is important to acknowledge that our study did not conclusively demonstrate this change and further research is needed to confirm this hypothesis.
Moreover, an increase in PTS also triggers an increase in ATT. 20 We do not know what ended this progression, but the aforementioned osteophyte, named the “cupola sign,” formed on the posteromedial tibial plateau, is thought to be an adaptive response to limit the increase of ATT. We noticed osteophytes in almost all patients in the chronic ACL deficiency group. 7
Our study reported a varus deformity originating from the proximal tibia in patients exposed to ACL deficiency for ≥5 years. While we detected a significant difference in both MPTA and MTFA measurements compared with those of the unaffected knee, we did not detect a similar difference in patients with acute (<1 year) ACL injury. Although an increase in varus angulation with exposure to ACL deficiency has been previously reported in the literature, 15 it is still controversial whether varus causes ACL rupture or ACL rupture causes progression of the varus.16,24 There is also a mechanism complicated by varus alignment and osteoarthritis due to the gradual stretching of the posterolateral structures over the years under ACL deficiency, as suggested by Dejour et al. 9
No significant relationship was detected between exposure duration and ATT with an increase in PTS in the chronic ACL deficiency group. While a suggestive association with ATT was observed, it did not reach statistical significance based on the Spearman correlation analysis. The validation of this relationship may necessitate a future study employing a larger sample size for robust statistical analysis. The reason for the lack of correlation with exposure duration might be that the structural change in the bone may have developed in a shorter period than 5 years, the increase in the PTS may have limited itself, and no further change may have occurred after the 5 years of exposure. Therefore, conducting this study with a larger sample size and a wider exposure time interval may help find meaningful results in terms of correlation.
The PTS measurement technique is another topic that needs to be considered. Most of our readings fell between 10° and 12°. These numbers were a little bit higher than what they ought to be according to the analysis by Matsuda et al. 21 We think that the reason for this was that we performed the measurements on the plane perpendicular to the midline points that we determined at 6 and 16 cm distal to the joint line. Faschingbauer et al 11 showed a difference between the measurements made over the whole tibia sagittal axis and the measurements made over the proximal axis of the tibia and found that higher slope values could be obtained in the measurements made from the proximal axis. Since we did all the measurements using the same method, this will not negatively reflect on the study results.
No significant group difference was observed when comparing the medial and lateral PTS of the affected sides, but the chronic ACL deficiency group exhibited significantly lower PTS on the unaffected side compared with the acute ACL deficiency group (medial: 10.1° vs 12.1° [P = .012]; lateral: 8.9° vs 10.5° [P = .029]). This finding aligns with the observation of Medda et al 23 that the PTS varies widely among individuals. 23 The fact that we found significant differences in the PTS between unaffected and affected sides in the chronic ACL deficiency group but not in the acute ACL deficiency group was sufficient to confirm our hypothesis that long-term exposure to ACL deficiency would increase the PTS on the affected side compared with the contralateral side.
Limitations
There are several limitations to the present study. First, it is important to note that patients in the chronic ACL deficiency who were significantly older than those in the acute ACL deficiency group exhibited a diverse range of time intervals since their injuries. For that reason, it remains challenging to understand how PTS is affected over time in this population. Second, the limited sample size was a notable constraint because finding patients with chronic ACL deficiency was difficult. While we did achieve the sample size predicted in the power analysis for comparing the PTS angle difference between cohorts, power analysis was not performed for other variables and correlations. Third, we did not consider the instability caused by meniscal tears, especially lateral meniscus posterior horn or root and medial meniscus ramp lesions. These tears or lesions may further affect the change in the PTS. Last, it is essential to emphasize that we did not evaluate patients over time, making it challenging to draw definitive conclusions about whether the changes in angulation were progressive over time.
Conclusion
The findings of this study showed that the affected knees of patients with chronic ACL deficiency had higher medial and lateral PTS when compared with the unaffected contralateral knees. Therefore, when planning ACLR in patients with long-term exposure to ACL deficiency, it is important to accurately measure the PTS preoperatively because additional slope-correcting osteotomies may be required in these patients.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241247524 – Supplemental material for Comparison of Side-to-Side Difference in Posterior Tibial Slope in Knees With Acute Versus Chronic Anterior Cruciate Ligament Deficiency
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241247524 for Comparison of Side-to-Side Difference in Posterior Tibial Slope in Knees With Acute Versus Chronic Anterior Cruciate Ligament Deficiency by Ömer Faruk Sevim, Selim Ergün, Suna Şahin Ediz, Engin Eceviz and Mustafa Karahan in The Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted October 23, 2023; accepted October 29, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kartal Dr Lütfi Kırdar City Hospital (ref No. 2021/514/204/4).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.