
Abstract
Background:
The jackling position within rugby has not been previously described as a mechanism for proximal hamstring injuries.
Hypothesis:
Acute surgical repair of proximal hamstring avulsion injuries sustained from the jackling contact position enables a return to a previous level of sporting activity with low risk of recurrence.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study included 54 professional rugby players (mean age, 26 ± 4.8 years) who underwent acute primary surgical repair of complete, proximal hamstring avulsion injuries. The mean follow-up time was 17 months (range, 12-24 months). Mean isometric hamstring strength and function testing was performed at 3 months and 1 year after repair.
Results:
Of the 54 players, 51 (94.4%) returned to their preinjury level of sporting activity. The mean time from surgical repair to full sporting activity was 7 months (range, 4-12 months). No patients had recurrence of the primary injury. At 1 year postoperatively, patients had significantly restored mean isometric hamstring muscle strength when compared with the uninjured leg at 0° (98.4% ± 2.8%), 15° (95.9% ± 2.9%), and 45° (92.9% ± 4.1%); improved Lower Extremity Functional Score (78.0 ± 2.0); and improved Marx activity rating score (14.3 ± 1.5) (P < .001 for all).
Conclusion:
Acute surgical repair of proximal hamstring avulsion injuries caused by the contact jackling position produced a high return to preinjury level of sporting activity, increased muscle strength, and improved functional outcome scores, with a low risk of recurrence at short-term follow-up.
Hamstring muscle injuries are one of the most commonly seen injuries in sports such as rugby union, 8 Australian Rules football, 23 track and field, 1 and soccer. 15 Within elite-level rugby, Brooks et al 8 showed that 22% of professionals sustained a hamstring injury during the season. These injuries are associated with potentially career-threatening prognoses in elite athletes, with prolonged time for rehabilitation, delays in return to preinjury level of sporting activity, and a high risk of recurrence.2,28
The most common mechanism of hamstring injury seen is during the late swing phase of high-speed running. 12 The rapid knee extension with the hip flexed causes eccentric contraction of the hamstring muscle complex. The “slow-stretching” injury of the hamstrings with simultaneous extremes of hip flexion and knee extension has also been described in the literature. 2 Patients are usually evaluated with pain over the ischial tuberosity, reduced range of motion, hamstring weakness, and an inability to participate in sporting activity. 3 Direct-contact injuries have not been described in the literature to date, even though at our center, we have seen a significant number of rugby injuries caused by player contact. One example is the jackling position, seen after a rugby tackle when a defensive player attempts to win the ball from the attacking opposition on the ground (Figure 1).

(A) Jackling position seen during a professional rugby match. The red shirt team is attacking, and the black shirt team is defending. (B) The yellow outline highlights the player in the jackling position.
The jackling position occurs before a ruck can ensue over the tackled player on the ground. This leaves the defensive player susceptible to contact from the attacking opposition before a ruck ensues. This explosive contact between 2 players causes rapid knee extension while the hip is still flexed. Figure 2 shows this change in force through the muscle during contact. The hamstring complex is at maximal eccentric contraction with significant forces above and beyond the usual body weight of the athlete. This can cause significant injury and even complete proximal avulsion of the tendons.
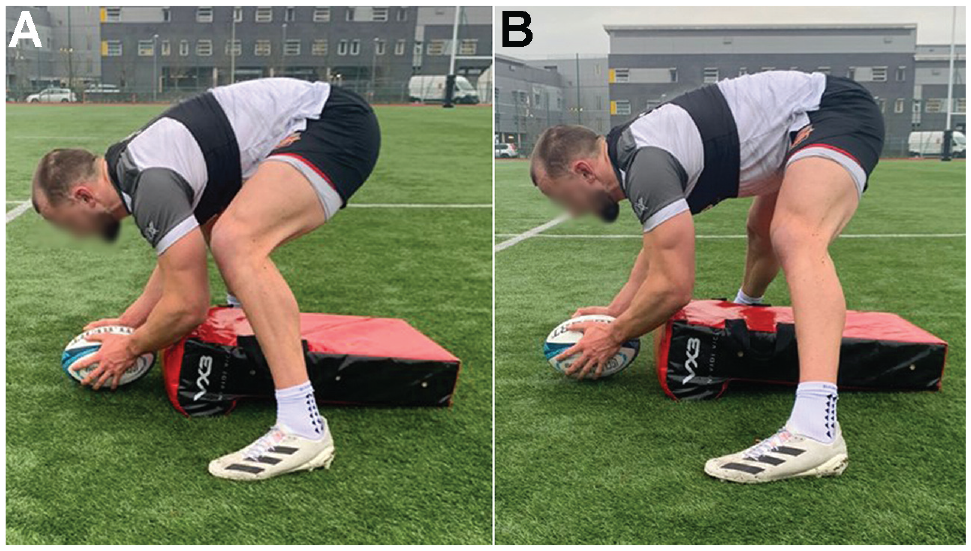
(A) The jackling position before contact with the opponent showing the knee flexed and hip flexed. (B) The knee extends on collision with the opposition player. Therefore, the hamstring muscle is placed under full tension and excessive load.
Nonoperative management of proximal intrasubstance hamstring injuries is still the mainstay of treatment, as seen in the study of Brooks et al 9 study on elite-level rugby, where no injuries during the entire season needed surgical repair. This study recorded injuries between 2002 and 2004, and since then, rules have significantly changed, allowing the jackling position to become a prominent part of the game. Data from 1 professional rugby club has shown that jackling attempts increased from 29 per game in 2017-2018 to 40 per game in 2020-2021. Therefore, we are now seeing the incidence of complete avulsion injuries from this unique position increase in rugby. Complete proximal avulsions have been shown to benefit from surgical repair, with improved outcomes for athletes including restoration of strength, shorter recovery periods, and less risk of reinjury.7,10,11,13,19,20,26,31
The aim of this study was to highlight the unique mechanism of hamstring injury in rugby players and present the outcomes from surgical repair. These findings may then be taken into consideration for rehabilitation timelines and expectations for recovery. This may help reduce reinjury rates from the jackling position in rugby.
Methods
Patient Selection
This prospective study included 54 professional level rugby players (international level, English Premiership, English Championship, and Pro12/Pro14) who underwent acute surgical repair for complete proximal hamstring avulsion injuries confirmed on magnetic resonance imaging (MRI). All operative procedures were performed by the senior author (F.S.H.) between February 2013 and February 2020. Characteristics and baseline data for all study patients are shown in Table 1.
Characteristics and Baseline Data of the Study Patients (N = 54)

Inclusion criteria included the following: (1) injury sustained in the jackling position during rugby confirmed through athlete history or film review, (2) operative intervention within 4 weeks of injury, and (3) preoperative MRI to confirm complete 3-tendon avulsion with at least 1 cm of retraction (British Athletics Muscle Injury Classification [BAMIC] grade 4 injury) 24 in the proximal tendons. Exclusion criteria were as follows: (1) nonjackling injuries, (2) incomplete avulsions, (3) injury sustained >4 weeks before surgical intervention, (4) BAMIC grade 1 to 3 proximal hamstring injuries, (5) recurrent injury after previous nonoperative treatment or surgical treatment at a different treatment center, and (6) nonprofessional-level players. Hospital review board ethics approval was obtained before commencement of the study, and written informed consent was obtained from all study patients.
Surgical Technique
All operative procedures were performed with the patient in the prone position under general anesthesia. The gluteal skin crease was marked, and a transverse incision of 5 to 10 cm was performed within the skin crease. The underlying subcutaneous tissue was divided using electrocautery until the gluteal fascia was exposed. The fascia was incised to expose the inferior border of the gluteus maximus. Care was taken to preserve the posterior cutaneous nerve of the thigh. The hamstring fascia was divided and any underlying hematoma evacuated. The hamstring muscles were traced proximally to their insertion into the ischial tuberosity. Intraoperative examination confirmed a complete avulsion of the tendons. The integrity of the adjacent sciatic nerve was inspected. The ischial tuberosity bony insertion was prepared using an osteotome to create a healthy bleeding bed for the anchors. One to 3 bone suture anchors (Healix 5.5-mm [DePuy Synthes] with double-loaded Orthocord sutures) were placed into the tuberosity, and the sutures attached were woven through the proximal tendon in a modified Kessler technique. The knee was held flexed at 30°, while the tendons were parachuted down to the tuberosity and secured with knots. The knee was fully extended to ensure satisfactory tension in the repair throughout the arc of motion. The wound was copiously irrigated with normal saline, and absorbable sutures were used to perform a layered closure of the overlying fascia, subcutaneous tissue, and skin. All patients were placed in a hinged knee brace for 4 weeks, limited to 60° to 120° of knee flexion for 0 to 2 weeks, and instructed to avoid hip flexion >70°, followed by incremental increases in range of motion from 2 to 4 weeks postoperatively.
Postoperative Rehabilitation
All patients received a standardized, milestone-based, rehabilitation program supervised by an experienced sports physical therapist. The rehabilitation program was divided into 4 distinct phases:
Phase 1: Rest, ice, compression, and elevation; mobilize partial weightbearing with crutches; aspirin 150 mg once daily; limit excessive combined hip flexion and knee extension; touch-toe weightbearing with progression to normalization of gait.
Phase 2: Regain pain-free range of motion, full weightbearing, concentric and eccentric training, core strengthening.
Phase 3: Aerobic conditioning with light jogging, cycling, and swimming; muscle strengthening with resistance exercises, double- and single-leg squats, quadriceps extension, and hamstring curls; sport-specific training.
Phase 4: Return to full sporting activity when full pain-free range of motion, isokinetic muscle strength 85% of uninjured limb (at 0°, 45°, and 90° of knee flexion), and no concerns with sport-specific training.
Outcome Measures
All study patients were reviewed by the operating surgeon in the outpatient clinic or virtually at regular intervals until return to play. Return to play was defined as playing within a competitive match (preseason/regular season). Study outcomes were recorded by a specialist nurse practitioner or club therapist at predefined intervals after surgery. All outcomes at 3 months and 1 year after surgery were collected.
Patient Satisfaction
Patient satisfaction was recorded at 3 months and 1 year after surgery using the Musculoskeletal Outcomes Data Evaluation and Management System, which scores patient satisfaction on a scale of 1 to 5 (1, very unsatisfied; 2, unsatisfied; 3, neutral; 4, satisfied; and 5, very satisfied). 16
Hamstring Muscle Strength
Isometric hamstring muscle strength was tested at 3 months and 1 year postoperatively. The patient was placed in prone and a handheld dynamometer (Hoggan Scientific) was positioned over the ipsilateral calcaneus. The maximum resisted knee flexion force (in newtons) was recorded at 0°, 15°, 45°, and 90°. This technique was repeated 3 times, and a mean flexion force at each of these angles in the injured limb was calculated. All values were compared with the contralateral uninjured limb to calculate the percentage of normal hamstring muscle strength.
Functional Assessment Scores
All study patients completed the Lower Extremity Functional Scale (LEFS) and the Marx activity rating score at 3 months and 1 year postoperatively. The LEFS is a validated and effective questionnaire for assessing specific lower limb function. It has an 80-point scale with 20 questions and 4 points allocated to each question, with a minimum clinical difference of 9 points. 6 The Marx score measures patient activity level and knee function independent of age, sex, and type of sporting activity. Scores of 0 to 4 are assigned to 4 activities: running, change direction, decelerating, and pivoting, with a total score of 16. 22 Time from surgical intervention to full return to sporting activity was collected in all study patients. All complications with their respective treatments and outcomes within 1 year of the primary surgery were recorded.
Statistical Analysis
Paired t tests were used to compare patient characteristics, and study outcomes were found to be normally distributed, while the Mann-Whitney U test was used for continuous outcomes found not to be normally distributed. Categorical outcomes were compared using the Fisher exact test. Statistical significance was set at a P value <.05 for all analyses, and all statistical analysis was performed using SPSS Version 24 (IBM).
Results
All 54 study patients completed follow-up. The mean follow-up time was 17 months (range, 12-24 months) from the date of surgery.
Return to Function and Recurrence
Of the 54 study patients, 51 (94.4%) returned to their preinjury levels of sporting activity. The mean time from surgical intervention to return to full sporting activity was 7 months (range, 4-12 months). No study patients sustained a recurrence of the primary injury.
Patient Satisfaction
Surgical repair of jackling injuries was associated with high patient satisfaction at 3 months and 1 year after surgery. In total, 95% of patients were either very satisfied or satisfied at 1 year after surgery.
Hamstring Strength
Surgical repair was associated with improved muscle strength between 3 months and 1 year after surgery. At 1 year, 94.4% of patients had restored strength to >90% of the uninjured side (Table 2).
Changes in Hamstring Strength (Compared With Uninjured Limb) Between 3 and 12 Months Postoperatively a

Data are reported as mean ± SD or mean (95% CI).
Functional Progress
Progressive improvements were observed in LEFS and Marx scores at 1 year compared with 3 months postoperatively (Table 3). At the 3-month follow-up, 6 patients (11.1%) had LEFS scores of 80 (of 80) and 35 patients (64.8%) had LEFS scores >75. Marx scores followed a similar trend to LEFS scores, with statistically significant improvement at each follow-up interval after surgery.
Changes in LEFS and Marx Scores From 3 Months to 1 Year Postoperatively a

Data are reported as mean ± SD or mean (95% CI). LEFS, Lower Extremity Function Score.
Complications
Only 1 patient (2%) had a postoperative complication. The patient had a bone anchor loosen that needed removal. Specifically, there were no episodes of venous thromboembolisms or neurological complications. There was no incidence of injury recurrence.
Return to Sport
Overall, 90.7% of athletes had returned to their previous level of sport at 1 year postoperatively. Three patients decided to retire due to the injury and therefore never achieved this milestone, although they were deemed to have healed satisfactorily and have not sustained any further hamstring problems. Two of the athletes retired because of their age (37 and 34 years, respectively), and 1 athlete (26 years) decided to retire because of their multiple injuries (non-hamstring related). Two other patients were excluded from analysis in return to sports because they had surgery on other injuries and were taking time out voluntarily. They had been cleared by the rehabilitation team to return to sports before these injuries or decisions. They returned at 16 and 18 months, respectively. Figure 3 highlights how many players returned to rugby in each month after surgery. Approximately 60% of players returned by 6 months, with a staggered return seen up to 12 months due to setbacks in rehabilitation and timing of injury within the season.

Prevalence of return to sports in months.
Discussion
In this study, we found that acute surgical repair of complete hamstring proximal avulsion injuries from the jackling contact position was associated with a high return to preinjury level of sport, increased muscle strength, and improved functional outcome scores, with a low risk of recurrence. To our knowledge, this is the first study to report on patients with hamstring injuries sustained through the jackling position and the outcomes of their surgical repair.
The most common mechanism of hamstring injury seen is during the late swing phase of running when the hip is flexed but the knee extends to cause eccentric contraction within the hamstring muscles. 7 Askling et al 2 first highlighted a different mechanism of injury from that most commonly seen during sprinting. They described slow stretching movements in athletes with extreme hip flexion and knee extension causing semimembranosus injury that resulted in longer recovery periods than more common mechanisms. A significant proportion of their study group (47%) decided to finish their sports careers. The study highlighted a unique mechanism of injury and the importance of diagnosing specific hamstring injury patterns acutely to prevent poor outcomes. Ayuob et al 4 showed that when semimembranosus injuries are surgically repaired, the return-to-sports rate is much higher at 95% compared with the 47% seen in the Askling et al 2 study.
The current study highlights the unique proximal hamstring avulsion injuries sustained in patients during the jackling contact position in rugby. Acute surgical repair enabled 94.4% of patients to return to their preinjury level of sport, with only 3 patients retiring from rugby. These findings highlight the importance of early diagnosis and consideration of surgical repair for these injuries. It was not possible to include a control group as all study patients were high-performance-level athletes who wanted operative management instead of nonoperative given the poor functional outcomes and high risk of recurrence associated with rehabilitation alone for these high-grade injuries.2,7,10,14,25,27
A recent meta-analysis of 795 proximal hamstring avulsion injuries reported significantly higher patient satisfaction (90.81% vs 52.94%) and hamstring strength (85.01% vs 63.95%) with operative compared with nonoperative management. 7 Buckwalter et al 10 showed improved return to sport in 262 patients with operative versus nonoperative treatment (94.5% vs 54.2%). The findings of the current study are comparable to those in these reviews in terms of hamstring muscle strength and return to sports after surgical repair. Barnett et al 5 had a much lower return-to-sport rate of 76% in 92 patients with operative treatment of proximal hamstring avulsion injuries. This may be explained by a significant proportion of patients (62.5%) having chronic injuries with surgery delayed >6 weeks. The current study may have had more favorable outcomes owing to the strict inclusion criteria of only acute (within 4 weeks) hamstring injuries sustained during contact in the jackling position of rugby.
Delayed surgical treatment of proximal hamstring avulsion injuries has shown inferior patient-reported outcomes, increased nerve symptoms, and longer recovery periods before return to sports.26,30 Subbu et al 30 found quicker return to sports (16 vs 25 weeks) and fewer complications, such as local nerve irritation (2.5% vs 29%) if the operation occurred before 6 weeks. It is therefore recommended that patients with avulsion injuries undergo acute surgical repair to reduce the aforementioned complications. The current study found that the mean time for return to sports was 7 months, which is longer than the rates of Subbu et al 30 and Lempainen et al, 21 who reported a mean time for return to sports of 4 months. However, these studies included partial injuries, which are not as high-energy as the jackling contact injury and take less healing time than complete avulsions, and the definition of return to sport was not clarified. It takes significant force to avulse a young athlete's hamstring tendons, and this is certainly the case in the jackling position, whereby an opponent's whole-body weight at speed will collide with the patient. We would therefore assume longer recovery times with this amount of initial trauma when compared with partial hamstring tears. This area will need further research to assess whether higher-energy injuries need surgical intervention and longer recovery periods.
Hamstring isometric strength was restored to within 90% of the uninjured limb in 94.4% of patients at 1 year after surgery. Two athletes took >1 year to return to sports because of additional injuries unrelated to their hamstring requiring surgery. Both athletes achieved 90% hamstring isometric strength restoration compared with the uninjured limb at 1 year after surgery, although alternative surgery (non-hamstring related) and rehabilitation inhibited return to sport within 1 year. These results are superior to those reported in the literature with nonoperative management of these injuries, such as the study by Hoffman et al, 17 who found that nonoperative management of hamstring avulsion injuries restored only 62% of hamstring muscle strength compared with the uninjured side. Operative repair enables the tension in the avulsed tendon to be restored and reduces the reliance on scar tissue during muscle loading. All patients in the current study were competitive- or elite-level athletes, so they may have had better rehabilitation potential and reduced comorbidities compared with the cohort of patients in the study by Hoffman et al, 17 which had a mean age of 59 years. Bodendorfer et al 7 reported a hamstring strength of 85% in 376 patients in their systematic review of surgical repairs, which is consistent with the findings of the current study at 1 year after surgery.
One of the main reasons for operative repair versus nonoperative treatment is the high recurrence of hamstring injury on return to sports.14,25 This is because the scar tissue that developed in the tendon, and the muscle is weaker and more likely to retear.18,29 With the sporting community unaware of this jackling-type avulsion injury, many athletes will be misdiagnosed or mistreated. Pollock et al 25 have shown with MRI scans that more severe hamstring injuries have higher rates of reinjury, even rising to 63% in proximal avulsions treated nonoperatively. Highlighting this mechanism of injury will hopefully reduce the rates of rerupture from misdiagnosis and nonoperative treatment.
Dating back to the previous Rugby World Cup in 2019, there has been speculation regarding World Rugby's proposal to change rules at the breakdown, specifically highlighting the risk of jackling. Despite proposals, 4 years in the future at the next Rugby World Cup, no specific law change had been made to prevent the defending player from jackling. However, with the increased refereeing vigilance regarding the reduced height of approaching the ruck or tackle, players are theoretically less likely to explosively contact the jackling player; thus, we may see a decrease in the incidence of jackling-associated injuries.
Strengths and Limitations
The main strengths of this study are that it describes a new mechanism of injury and its associated surgical repair, which will facilitate medical professionals managing patients with these rare hamstring injuries in the future. Furthermore, the surgical repair undertaken used a standardized technique by a single surgeon with a predefined postoperative rehabilitation protocol, and a range of validated study outcomes were recorded at regular intervals after surgery. Among the limitations of the study is that no control group of patients undergoing nonoperative treatment was included. This was not possible as the patient group included all high-performance athletes who did not want to be randomized to nonoperative treatment. This is a single-surgeon series, and therefore, replication of results may be difficult. Very few surgeons have experience and high volume in this procedure to allow multicenter analysis. The sample size is also limited as we restricted this analysis to professional players.
Conclusion
The acute proximal hamstring injury sustained from the rugby jackling position is a unique mechanism of injury that has not been previously reported in the literature. It is important to highlight this mechanism of injury to aid in diagnosis and prevent delays to treatment. Acute surgical repair of this injury is associated with high patient satisfaction, increased hamstring muscle strength, improved functional outcome scores, and high return to preinjury level of sport with low risk of reinjury.
Footnotes
Final revision submitted January 25, 2024; accepted February 12, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Princess Grace Hospital.