
Abstract
Background:
The ulnar collateral ligament (UCL) is the primary soft tissue stabilizer to valgus stress in the elbow and is placed under this valgus stress during the throwing motion. Although there are known risk factors for UCL injury, it is unknown whether the UCL undergoes adaptive changes in athletes from different climates.
Purpose:
To compare elbow stress ultrasound (SUS) findings between professional baseball pitchers from warm climates versus cold climates and assess significant differences in adaptive and morphologic changes in the UCL.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Dynamic SUS evaluations were performed over 18 years on the dominant and nondominant arms of 643 professional pitchers from warm and cold climates as determined by the player's country/state of origin. Studies were compared with respect to relative UCL thickness (dominant arm vs nondominant arm), relative glenohumeral joint laxity (joint space distance under stress vs joint space distance at rest), and the presence of morphologic changes such as tears or calcifications. In addition, a subgroup analysis was performed to compare the progression of SUS findings over 3 years in players with sequential yearly data.
Results:
Players from warmer climates had significantly greater relative UCL thicknesses than players from colder climates (1.75 vs 1.50 mm, respectively; P = .047). There were no differences between these 2 groups in terms of relative ulnohumeral joint laxity (P = .201), presence of morphologic changes (P = .433), 3-year progression of relative UCL thickness (P = .748), or relative joint laxity (P = .904).
Conclusion:
Professional pitchers from warm climates had a greater side-to-side difference in UCL thickness between the dominant and nondominant arms. This may be due to the potential for year-round throwing among baseball players from warm climates. There was no difference in laxity, thickness progression, laxity progression, or the presence of additional morphologic changes.
The ulnar collateral ligament (UCL) is the primary soft tissue stabilizer to valgus stress in the elbow. In overhead-throwing athletes, particularly baseball players, the medial elbow is susceptible to injury due to repetitive stress during throwing.1,3,8,10,23,39 For complete UCL tears or partial tears that have failed nonoperative treatment, patients may undergo surgical reconstruction or repair. Although the rate of return to play among professional baseball players ranges from 80% to 97% after UCL reconstruction (UCLR), the prolonged recovery keeps these athletes sidelined for up to 12 to 15 months,35,39 contributing to millions of dollars (average of US$1.9 million per pitcher in 2019) in economic impact to Major League Baseball (MLB) teams. 29 Approximately 25% of professional baseball pitchers have undergone at least 1 UCLR. 14 Preventative measures have been studied to avoid this career-interruptive injury.6,7,22,30
Much of the present research regarding UCL injuries in youth and professional baseball players has focused on identifying risk factors for developing elbow pain and the potential need for future elbow surgery.10,15,20,23,26-28,31,33 While originating from warm climates has been shown to be a risk factor for UCLR compared with originating from colder climates, 18 no study has specifically explored the adaptive changes that the UCL undergoes in players from different climates. As such, our understanding of what may put these players at risk of injuries is limited.
Although magnetic resonance imaging with or without intra-articular contrast enhancement remains the gold standard for diagnosing UCL injuries, dynamic stress ultrasound (SUS) has been shown to be a reliable tool for evaluating the structure of the UCL.5,11,13,17,21,32,37 Multiple studies have shown that the UCL in the dominant arm of professional baseball players and adolescents was thicker and had increased laxity to valgus stress.3,13,24,33 While SUS has been used to validate the risk of increased pitch count and pitch volume on the change in UCL morphology,3,9,17,24 to our knowledge, no study has investigated SUS findings of the UCL in professional baseball players from warm-weather locations compared with cold-weather locations.
This study aimed to compare SUS findings between pitchers from warm- and cold-climate locations and assess significant differences in adaptive and morphologic changes in the UCL. The hypothesis was that players from warmer climates would have thicker UCLs, with higher incidences of morphologic changes.
Methods
Inclusion/Exclusion Criteria
This study of professional baseball pitchers was conducted using prospectively collected preseason SUS measurements over 18 years (2002-2020). Dynamic SUSs were performed as part of routine spring training evaluations. However, players had the option to decline this evaluation. A total of 1153 SUSs were performed on the elbows of 650 unique, asymptomatic professional pitchers from various minor league divisions (Rookie, A–, A, AA, AAA) within a single MLB organization. An internet search of identified pitchers was performed to collect player demographic data—including country/state of origin and the round in which players were drafted. Geographic and demographic data for all MLB players were collected using publicly available information (https://www.baseball-almanac.com). 4 This study was determined to be exempt from institutional review board approval.
Baseline measurements were taken using players’ first available SUS. The exclusion criteria were (1) incomplete measurements and (2) missing and unobtainable demographic data. After appropriate exclusion, 643 professional pitchers and 646 baseline SUSs were included in this analysis (Figure 1A). In addition to baseline measurements, a 3-year progression on SUS was also analyzed when available (Figure 1B). If a player had multiple sets of SUSs separated by 3 years (ie, 2012-2015 and 2013-2016), the earliest available measurements were used for analysis. A total of 60 players and 120 SUSs (60 initial and 60 final) were included in this secondary analysis.
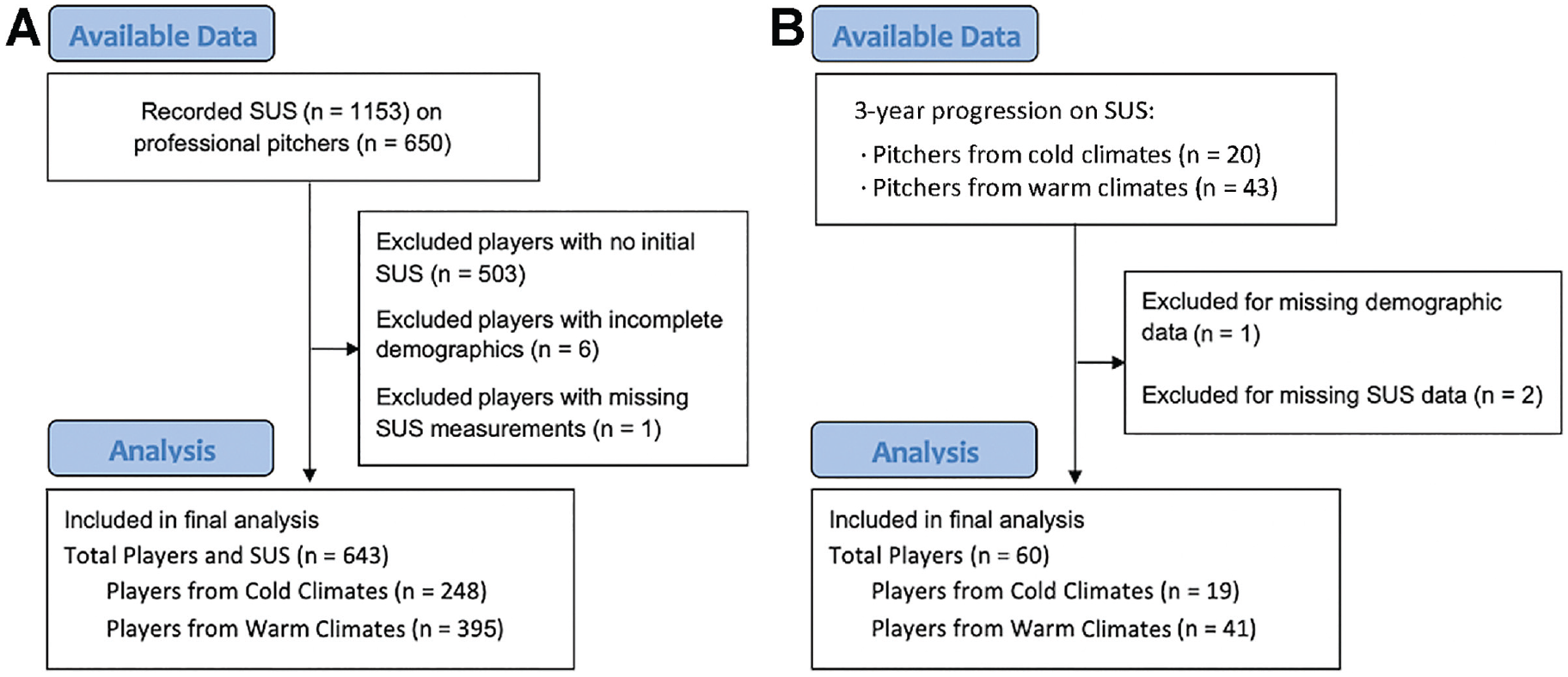
Flowchart of player inclusion in the (A) initial SUS analysis and (B) the 3-year progression SUS analysis. SUS, stress ultrasound.
Determination of Climate Differences
Determining whether a pitcher was from a cold or warm climate was done using the same method described by Erickson et al, 18 who used the country or state where each player pitched in high school as the basis of location. Before the onset of the study, warm-climate areas were defined as countries or US territories or states that are intersected by or closer to the equator than the northern or southern 33rd parallel. If a country or state was farther from the equator than the 33rd parallel, it was considered to have a cold climate. A total of 44 unique cold-climate locations and 24 unique warm-climate locations were included (Appendix Table A1).
Imaging Technique
All pitchers were evaluated using the same standard sonography imaging technique as previously described by Ciccotti et al. 13 All participants were imaged by a single, experienced, independent musculoskeletal radiologist who was a co-developer of the current technique utilizing a multifrequency 13-MHz linear-array transducer (SonoSite MicroMaxx or M-Turbo; SonoSite) and a standard acoustic coupling gel. During the evaluation, pitchers’ right elbows were placed at 30° of elbow flexion (measured with a digital goniometer and the longitudinal axis of the forearm and upper arm) in a standardized instrumented device (Telos). This angle was chosen because (1) the UCL has been demonstrated to be the primary restraint against valgus stress at 30° of elbow flexion and (2) appropriate stress using the standardized stress device can only be consistently applied at lower degrees of elbow flexion (the players’ elbows could not be appropriately positioned in the stress device at flexion angles >60°). In this position, the thickness of the UCL anterior band at its middle portion, at the joint line level, was measured. The ulnohumeral joint space at the anterior band was also measured first at rest, followed by when 150 N of valgus stress was applied. Images were evaluated for calcifications, tears, hypoechoic foci, and osteophytes. All described measurements were performed with a precision of 0.1 mm and were recorded in a computer spreadsheet for subsequent analysis. The same was done in the same order for the left arm.
Calculated Measurements
Side-to-side differences in SUS findings were calculated. The term “relative” was used to describe calculated side-to-side differences where nondominant side measurements were subtracted from dominant side measurements (UCL thickness, joint spaces). The primary outcomes of interest were relative UCL thickness and relative ulnohumeral joint space laxity (the ulnohumeral joint space distance at rest subtracted from the joint space distance under stress). A positive result was used for relative UCL thickness and joint space laxity to indicate that the dominant arm UCL was thicker or had greater laxity, respectively, than the nondominant arm UCL.
A 3-year progression analysis of SUS measurements was also performed to assess changes in UCL findings in professional pitchers. As with the comparison of the initial measurement, progressive changes in relative SUS findings were calculated so that a positive value for relative UCL thickness indicates a relative increase in UCL thickness in the dominant arm compared with the nondominant arm over 3 years. A similar analysis was performed regarding relative laxity progression; thus, positive results indicate a relative increase in dominant arm laxity over 3 years.
Statistical Analysis
After a power analysis, the effect size was 0.142 for the overall analysis of players from cold (n = 248) and warm climates (n = 395). The effect size was 0.095 for comparing progressive data for players from cold (n = 19) and warm climates (n = 41).
The Mann-Whitney U test or the t test was used to compare continuous data, and the chi-square test or the Fisher exact test was used to compare categorical data. A logistic regression using the presence of any morphologic changes as the dependent outcome was also created to assess its relationship with other variables. The threshold for statistical significance was set at P < .05. All statistical analyses were done using R Studio Version 3.6.3 (R Core Team).
Results
Initial Ultrasound Measurements
The demographic characteristics of the 643 professional pitchers included in the comparison of cold- and warm-climate players are found in Table 1. Players in the cold-climate group were significantly older than those in the warm-climate group (23.1 vs 21.6 years, respectively; P < .001). Moreover, members of the cold-climate group were drafted at a higher rate (77.8% vs 46.8%; P < .001), drafted from high school at a higher rate (27% vs 16.2%; P = .001), and drafted from college at a higher rate (59.3% vs 37.5%; P < .001).
Demographic Characteristics of All Included Pitchers (N = 643) a

Data are reported as mean ± SD, median [IQR], or n (%). Bold P values indicate a statistically significant difference between groups (P < .05). IQR, interquartile range; US, United States.
Players born in the United States composed 67.3% of the total study participants (90.7% of the cold-climate cohort, 52.6% of the warm-climate cohort). These players represented a majority (95.8%) of those included in the final analysis and drafted. Because of the eligibility rules for inclusion in the professional baseball draft, high-quality non–US-born players may not be drafted in rounds that otherwise correlate with their pitching ability. A subanalysis was performed to highlight the US-born players’ demographic characteristics (Table 2). Findings indicated that players from warm climates were drafted at higher rates than players from cold climates (P = .013).
Demographic Characteristics of the US-Born Pitchers (n = 433) a

Data are reported as n (%). Bold P values indicate a statistically significant difference between climate groups (P < .05). US, United States.
The initial SUS measurements of the 248 cold-climate and 395 warm-climate players allowed for the comparison of dominant and nondominant arm findings between cohorts. No difference in the overall rate of morphologic changes (calcifications, tears, hypoechoic foci, osteophytes) was found on SUS in the dominant arm in either group (42.3% vs 45.8%; P = .433). Similarly, no difference was found in the rate of specific morphologic changes such as calcifications (22.2% vs 22.3%; P≥ .999), tears (0.40% vs 2.28%; P = .098), hypoechoic foci (23.8% vs 25.8%; P = .627), and osteophytes (12.5% vs 12.7%; P≥ .999).
Table 3 shows the side-to-side differences in SUS measurements between the dominant and nondominant arms. Players in the warm-climate group had a greater relative dominant arm UCL thickness than those in the cold-climate group (1.75 ± 1.75 vs 1.50 ± 1.76 mm; P = .047). No difference was found between the groups in relative laxity (P = .201).
Comparison of Dominant and Nondominant Arms in Initial SUS Measurements a

Data are reported as mean ± SD. The bold P value indicates a statistically significant difference between climate groups (P < .05). SUS, stress ultrasound; UCL, ulnar collateral ligament.
Logistic regression utilizing the presence of any morphologic changes as the dependent outcome was created to assess the influence of other variables on this finding (Table 4). Increased side-to-side difference of UCL thickness was found to be significantly associated with the presence of morphologic changes on SUS (odds ratio, 1.53 [95% CI, 1.38-1.72]; P < .001). No correlation was found between age and UCL thickness.
Linear Regression Model of Variables Associated With Presence of Morphologic Changes on SUS a

The bold P value indicates statistical significance (P < .05). OR, odds ratio; SUS, stress ultrasound; UCL, ulnar collateral ligament.
Three-Year Progression of SUS Findings
Table 5 details the demographic characteristics of the 60 professional pitchers included in the analysis for the progression of SUS. All demographic characteristics were based on the first of 2 SUS records. Groups differed significantly in the percentage of players who had been drafted (89.5% of cold-climate cohort vs 46.3% of warm-climate cohort; P = .004) and the round in which the player was drafted (P = .002).
Demographic Characteristics of Pitchers in the 3-Year Analysis (n = 60) a

Data are reported as median [IQR] or n (%). Bold P values indicate a statistically significant difference between climate groups (P < .05). IQR, interquartile range; US, United States.
A 3-year longitudinal analysis was also performed. In the dominant arm, no difference was found in the rate at which players developed any morphologic changes—including calcifications (P = .412), hyperechoic foci (P = .084), or osteophytes (P = .892). If calcifications were present on the initial and final SUS, there was no significant difference in the size of these calcifications (P = .692), and no players in either cohort had tears present on either the initial or final SUS. A comparison of the change in side-to-side differences over 3 years is found in Table 6. No difference was found in the progression of relative UCL thickness (P = .748) or progression of joint laxity (P = .904) between arms of either cohort.
Comparison of Dominant and Nondominant Arm SUS Measurements Over 3 Years a

Data are reported as mean ± SD. SUS, stress ultrasound; UCL, ulnar collateral ligament.
A positive value indicates that the dominant arm UCL saw a relative increase in thickness during the study period compared with the nondominant arm.
A positive value indicates a relative increase in laxity in the dominant arm over time.
Discussion
Our study represents the only research comparing relative UCL thickness and joint laxity in professional baseball pitchers from cold and warm climates. The hypothesis was only partially confirmed, as relative UCL thickness was significantly greater in the warm-climate groups. However, relative laxity was not significantly different, and there was no difference in the 3-year progression of relative thickness or relative laxity.
Climate
In warmer climate areas, baseball players could potentially participate in practices and games outdoors more often throughout the year. While this may be a theoretical benefit, the consequences of continued play throughout the year cannot be ignored. Risk factors for the UCL injury include pitching in leagues without pitch counts, pitching for multiple teams, continued pitching despite fatigue/elbow pain, increased pitching velocity/peak velocity, and pitching and catching in the same game.15,20,23,26-28,31,33,40 Although some can be avoided with load management, those playing without extended breaks throughout the year may have difficulty avoiding these risks. Fleisig et al 19 evaluated 481 youth pitchers for 10 years. They noted that those who pitched over 100 innings in 1 calendar year were 3.5 times more likely to sustain a serious shoulder or elbow injury. In a collegiate study, players who came from high schools in warmer areas or played in college at campuses in warmer weather were more likely to undergo UCLR. 41 Erickson et al 18 found similar results when studying MLB pitchers. They concluded that originating from warmer climates increased one's risk of undergoing UCLR more often and earlier in one's career. The present study revealed a greater relative UCL thickness in the dominant arm of players from warmer climates. These ultrasound changes may indicate the relationship between players being from warmer climates with the opportunity to throw year-round and exerting more strain on their UCLs.
UCL Thickness and Morphologic Changes
Within our study, there was a significant difference in relative UCL thickness for players from warm climates compared with cold climates, and on average, the dominant side UCL thickness was greater than that of the nondominant side—indicated by positive relative UCL thickness measurements in both cohorts. This is consistent with previous studies that suggest changes in thickness to tendons and ligaments are associated with continued mechanical stress.2,8,9,25,32,34,38 The increase in UCL thickness may represent the earliest anatomic change seen in response to continued overhead throwing and has been correlated with increased joint space gapping and the presence of hypoechoic foci and calcifications. 3 The adaptive response of thickening has been used to identify at-risk pitchers with abnormal adaptive responses; nonetheless, the clinical significance remains unknown since most players with thickened UCLs remain asymptomatic.2,8,12 Atanda et al 2 discovered that UCL thickness was directly correlated with pitching >67 pitches per appearance, pitching >5 innings, and those adolescents who have >5.5 years of pitching experience. This study cannot report whether the thickened UCL predisposes players to subsequent injuries. However, this knowledge can be used as a baseline for future studies to investigate any potential correlation.
UCL Laxity
Within this study, the relative laxity of the ulnohumeral joint was calculated by the difference in the distance of the ulnohumeral joint space at rest and when a valgus force was applied. When comparing the warm- and cold-climate groups, there was no significant difference in the 3-year progression of relative laxity (P = .904). Laxity of the UCL after repetitive overhead throwing is a common finding.2,8,16,36 Hattori et al 24 observed a significant increase in joint space gapping in 30 healthy high school baseball pitchers after just 60 pitches. Furthermore, after 100 pitches, the UCL had increased elasticity, leading to potential elbow valgus instability. Sasaki et al 36 compared dominant and nondominant arms of 30 collegiate athletes. They discovered that the medial joint space was significantly wider on the dominant side than the contralateral side. The proximal aspect of the ulna also appeared to shift laterally. While no statistical significance was discovered between baseline laxity of the pitcher's UCL and risk of injury, Erb et al 17 did find a direct correlation. Although previous studies have revealed the potential for increased laxity over a single outing, the present study does not support that midseason or per-outing changes persist over multiple seasons. The lack of changes observed over the 3 years may be due to limits to when these adaptive changes may occur. More research is necessary to determine whether players are more susceptible to laxity changes earlier or later in their careers, if there are limits to the degree of adaptations based on the UCL structure, or if there are confounding factors within the minor leagues (such as pitch count) that are not accounted for in this study's design and that have not been explored thoroughly before.
More extensive research controlling for common risk factors of UCL injury and including pitcher demographic characteristics and injury records would allow for clinical interpretation of these data. 10 Specifically, it would be important to understand the clinical significance of the reported findings and determine whether the adaptive changes in the UCL observed act in any protective or predictive capacity could be potentially predictive. Moreover, there are factors related to where players originate from that could not be accounted for, which should be considered in the context of these findings. Specifically, any potential lack of pitch limitations for developing athletes in Latin countries with primarily warmer climates could be to blame for different adaptive changes observed.
Limitations
Our study is not without limitations. First, this study includes ultrasound findings from only a single MLB organization and may be underpowered for comparisons throughout professional baseball as a whole. Second, the basis of this study was the assumption that players from warmer climates could throw and play in games more consistently year-round growing up; however, pitch count, total number of games played, and months per year played could not be determined. In addition, if a player is reported to be from a certain climate, this does not guarantee that the player's entire upbringing was within the designated climate. Third, while the primary focus of this study was the influence of “climate” on a player's SUS findings, there is potential that those drafted in earlier rounds may have been drafted for more desirable throwing characteristics such as velocity, which increases the risk for UCL injuries; this, however, cannot be examined with data available for this study. Demographic characteristics of players from the US were included to address this (see Table 2). Doing so allows us to highlight that a difference in draft status was still present, introducing a potential external confounding variable. Fourth, although players at the Rookie, A–, A, AA, and AAA levels were included, players at the major league level were not included because of when the ultrasounds were performed, meaning that this level of competition was not represented in the study cohort. Last, only 60 of 643 (9.3%) players were available for the 3-year side-to-side difference measurements. This reflects the fact that in professional baseball, major through minor leagues, a large percentage of players may move from team to team via trades, retirement, or release from contract, resulting in a small group of players being available for multiyear assessments.
Conclusion
Professional pitchers from warm climates had a greater side-to-side comparison in UCL thickness between dominant and nondominant arms. This may be due to the potential for year-round throwing among baseball players from warm climates. There was no difference in laxity, thickness progression, laxity progression, or the presence of additional morphologic changes. Future prospective research should evaluate any correlation between UCL thickness and risk for UCL injury in players from warmer climates.
Footnotes
Appendix
List of Cold- and Warm-Climate Locations Included in the Study

| Cold climate locations (n = 44) |
| • Countries: Canada, Czech Republic, France, Germany, Netherlands, New Zealand, Russia, and Republic of Korea. • US states and territories: Alaska, Arkansas, Colorado, Connecticut, Washington DC, Delaware, Idaho, Iowa, Illinois, Indiana, Kansas, Kentucky, Massachusetts, Maryland, Michigan, Minnesota, Missouri, Montana, North Carolina, North Dakota, Nebraska, New Hampshire, New Jersey, Nevada, New York, Ohio, Oklahoma, Oregon, Pennsylvania, South Dakota, Tennessee, Utah, Virginia, Washington, Wisconsin, and West Virginia. |
| Warm climate locations (n = 24) |
| • Countries: Australia, Brazil, Colombia, Cuba, Dominican Republic, Haiti, Mexico, Nicaragua, Panama, Taiwan, Trinidad, and Venezuela. • US states and territories: Alabama, Arizona, California, Florida, Georgia, Hawaii, Louisiana, Mississippi, New Mexico, Puerto Rico, South Carolina, and Texas. |
Final revision submitted September 14, 2023; accepted October 5, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.G.C. has received research support from Arthrex and DJO. R.A.J. has received education payments from Medinc of Texas, Liberty Surgical, Smith + Nephew and consulting fees from Zimmer Biomet. S.B.C. has received research support from Arthrex and Major League Baseball; education payments from Liberty Surgical; consulting fees from Zimmer Biomet and CONMED Linvatec; and royalties from Slack. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Thomas Jefferson University (iRISID-2022-1198).