
Abstract
Background:
Recent studies have suggested promising patient-reported outcomes after primary anterior cruciate ligament (ACL) repair with additional suture augmentation (SA).
Purpose:
To evaluate the risk for revision surgery and identify patient- and injury-related risk factors after ACL repair with SA in a large patient cohort subject to strict patient selection.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Included were 86 patients (61 female; 93% follow-up rate) who underwent arthroscopic ACL repair with SA between January 2017 and March 2019 by a single surgeon and had a minimum follow-up of 24 months. Patients were selected for surgery with regard to time to surgery (preferably on the day of injury), tear pattern (limited to Sherman types 1 and 2), and tissue quality (intact synovial coverage). Postoperatively, the patients who needed revision surgery were identified and compared with patients who did not undergo revision surgery, using the Mann-Whitney U test for nonparametric analysis and the Student t test for parametric analysis. A Kaplan-Meier analysis was performed to investigate the survival rate of the ACL repair.
Results:
A total of 9 patients (10%; median age, 48 years; interquartile range [IQR], 27-50 years) underwent revision surgery at 12 months postoperatively (IQR, 8-25 months). The median follow-up of patients without revision surgery was 35 months (IQR, 33-44 months). The revision-free survival rate was 97% (95% CI, 93%-100%) after 1 year, 93% (95% CI, 88%-98%) after 2 years, and 90% (95% CI, 83%-97%) after 4 years. Patient-related factors—such as sex (P = .98), age at surgery (P = .459), body mass index (P = .352), and preinjury level of sports (P = .53)—had no significant impact on the survival rate of the ACL repair. Injury-related factors—such as concomitant injuries of the medial (P = .860) and lateral menisci (P = .414) and the medial (P = .801) and lateral collateral ligaments (P = .534) or same-day surgery compared with a delay of surgery of up to 18 days (P = .277)—had no significant impact on the survival rate of the ACL repair.
Conclusion:
The revision rate of primary ACL repair with SA at a 2-year follow-up was 10%. Patient- and injury-related factors were not associated with the survival rate of the ACL repair.
Keywords
The resurgence of primary anterior cruciate ligament (ACL) repair has led to controversy and debates. Although proponents emphasize ligament preservation with decreased surgical morbidity, quicker recovery, and lower awareness of the knee postoperatively and provide good to excellent short- to midterm patient-reported outcomes, critics argue that these findings are only temporary, with patient-reported outcome scores deteriorating and the rates of revision surgery increasing over time—reasons why the historical concept of repairing the torn ACL has previously been abandoned.10,11,15,16
Contrary to the historical concept of open ACL repair, which was seen as an all-encompassing surgical gold standard, the recently developed ligament preserving technique with additional suture augmentation (SA) requires strict patient selection because tear pattern, tissue quality, and the interval between injury and surgery have been shown to be crucial.8,9,16,18,22,25
Although numerous studies have evaluated revision rates after different types of ACL surgery, there is a paucity of this information for the recent concept of arthroscopic ACL repair with SA, and the few data available are often derived from small heterogeneous patient cohorts partly without strict preoperative patient selection applied.1,3,6,7,25 Furthermore, potential risk factors such as demographic characteristics or concomitant ligamentous, meniscal, and chondral injuries have often not been evaluated regarding their impact on the revision-free survival rate of the augmented ACL repair. 25
Thus, the aims of this study were to (1) determine the revision rate and revision-free survival rate of arthroscopic ACL repair with SA and (2) identify potential patient- and injury-related risk factors for revision surgery in a large patient cohort subject to strict patient selection.
Methods
The local ethics committee approved the study protocol, and the study was performed in accordance with the 1964 Declaration of Helsinki. All patients provided informed consent. During the study period, between January 2017 and March 2019, a total of 176 patients underwent surgical treatment for an acute traumatic ACL injury: 83 patients (47%) underwent ACL reconstruction (ACLR), and 93 patients (53%) underwent ACL repair with SA (Figure 1). Of the 93 patients, we performed a retrospective analysis of 86 patients (61 female; follow-up rate, 93%) who underwent ACL repair with SA performed by a single surgeon (G.A.) and had a minimum follow-up of 24 months.
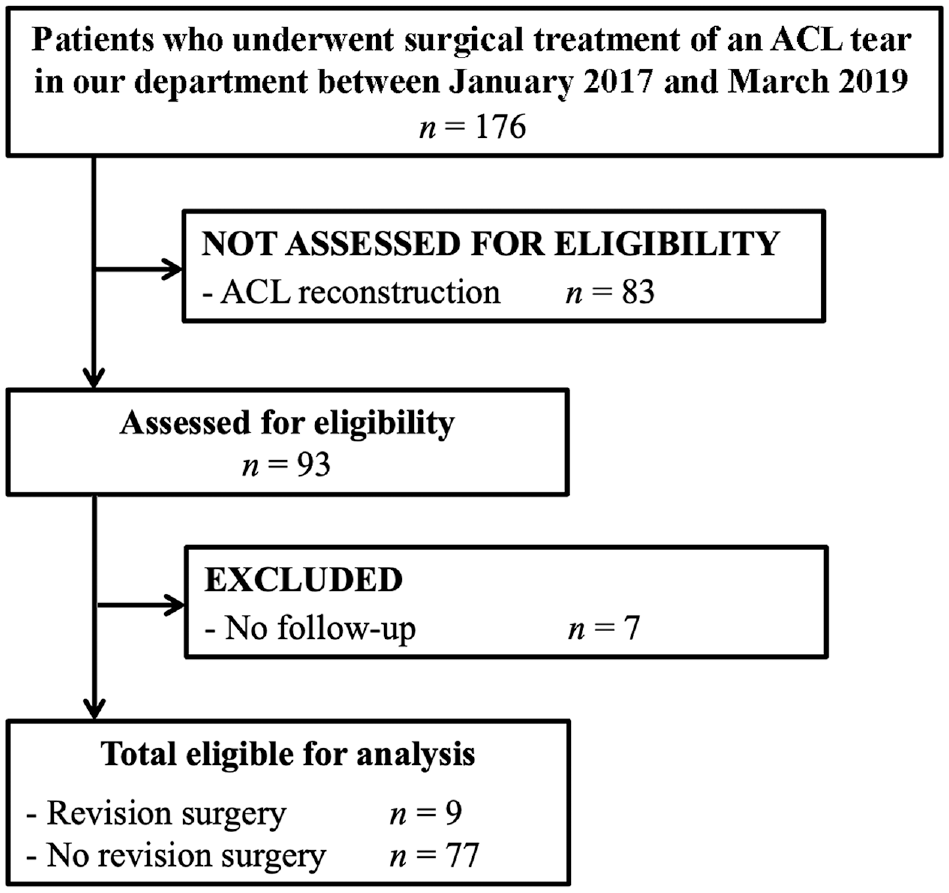
STROBE flow diagram of patient inclusion in the study. ACL, anterior cruciate ligament; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Patient Selection for ACL Repair with SA
All patients underwent magnetic resonance imaging (MRI) on the day of injury, and only patients with a proximal ACL tear pattern defined as Sherman type 1 or 2 were considered to be eligible for an arthroscopic ACL repair with SA (Figure 2).3,20,22,23, 24, 27 Patients with a midsubstance (Sherman type 3) or distal (Sherman type 4) tear pattern and/or poor intraoperative tissue quality of the ACL remnant underwent ACLR.22,20 During the study period, no patient preoperatively scheduled for an ACLR was intraoperatively eligible for an ACL repair. However, 2 patients who were preoperatively scheduled for an ACL repair showed insufficient tissue quality intraoperatively and underwent ACLR. No patient eligible for an ACL repair opted for an ACLR preoperatively. The same surgeon performed all surgeries, which were preferably performed on the day of injury (n = 37 [40%]); a delay in surgery occurred only in the case of external referrals, upon the patient's request, or due to insurance clearance issues. Concomitant injuries were diagnosed on the preoperative MRI or during arthroscopy, and they were addressed accordingly.

Proximal anterior cruciate ligament tear with good tissue quality and an intact synovial coverage.
Surgical Technique
The arthroscopic ACL repair was performed as a modification of the initially described technique by DiFelice et al 6 : A No. 2 FiberWire (Arthrex) was passed through the ACL remnant and shuttled proximally together with the SA construct (InternalBrace; Arthrex) through a femoral bone tunnel (Figure 3). In contrast to the study conducted by DiFelice et al, the present study used a flip button (TightRope; Arthrex) for proximal stabilization rather than an intra-articular femoral anchor to minimize the risk of implant irritation. Distal fixation was performed at the anteromedial tibia using a 4.75-mm anchor (SwiveLock; Arthrex). To enhance healing, a microfracture was performed around the femoral footprint. 21 Concomitant meniscal lesions were repaired when possible (RapidLoc; Mitek) or partially resected; concomitant chondral lesions were smoothened or underwent microfracture when necessary.

(A) A No. 2 FiberWire (Arthrex) was shuttled through the ACL remnant using a suture passer. (B) The ACL remnant was refixed at its anatomic origin of the femoral footprint using the suture augmentation construct. (C) Completed ACL repair with suture augmentation viewed from the anteromedial portal. ACL, anterior cruciate ligament.
Statistical Analysis
Of the 86 patients in the study cohort, those who underwent revision surgery were identified and compared with those who did not. Statistical analyses were performed with Excel 12.3.6 (Microsoft Corp) and SPSS (IBM Corp). Data distribution was determined using the Kolmogorov-Smirnov test. The median with its respective interquartile range (IQR) is given for all nonparametric values. Depending on data distribution, nonparametric analyses were performed with the Mann-Whitney U test and parametric analyses with the Student t test.
A Kaplan-Meier analysis was performed to investigate the survival rate of the ACL repair. Differences in survival rate according to patient-related factors (age, body mass index [BMI], and preinjury level of sport according to the Tegner score) and injury-related factors (concomitant medial meniscus, lateral meniscus, medial collateral ligament, and lateral collateral ligament injury and delay of surgery of up to 18 days) were assessed using the univariate log-rank test. All P values were 2-sided, and statistical significance was set at P < .05.
Results
The median follow-up of the patients without revision surgery was 35 months (IQR, 33-44 months; minimum follow-up, 29 months). In addition, the patient-reported outcome scores of the 77 patients without revision surgery were promising, with a median International Knee Documentation Committee score of 92 (IQR, 86-99), a median Lysholm score of 95 (IQR, 86-100), a median Forgotten Joint Score of 95 (IQR, 78-98), and a median preinjury Tegner score 19 of 6 (IQR, 5-7). A total of 9 patients (10%) underwent revision surgery after a median of 12 months (IQR, 8-25 months). There was no difference between patients with and without revision surgery in terms of age, BMI, or preinjury level of sport (Table 1). Of the 9 patients who underwent revision surgery, 4 patients experienced a traumatic retear, and 5 patients exhibited chronic knee instability with a positive pivot-shift test. The details of these patients are summarized in Table 2.
Median Age at Surgery, BMI, and Preinjury Level of Sports of Patients With and Without Revision Surgery a

Data are reported as median (IQR). BMI, body mass index; IQR, interquartile range.
Demographic, Injury- and Surgery-Related Data of the 9 Patients Who Underwent Revision Surgery a

BMI, body mass index; F, female; M, male; MCL, medial collateral ligament.
The revision-free survival rate of the ACL repair with SA was 97% (95% CI, 93%-100%) after 1 year, 93% (95% CI, 88%-98%) after 2 years, and 90% (95% CI, 83%-97%) after 4 years (Figure 4).

A Kaplan-Meier survival curve of arthroscopic anterior cruciate ligament repair with suture augmentation.
Patient-Related Factors Affecting Survival Rate
Patient sex (P = .98), age at surgery (P = .459), BMI (P = .352), and preinjury level of sports (P = .53) had no statistically significant impact on the revision-free survival rate. Before injury, 51 of 77 patients (66%) had a Tegner score of ≥7, participating in competitive sports. Of these 51 patients, a total of 6 patients (12%) underwent revision surgery compared with 3 of 26 patients (12%) with a Tegner score of <7.
Injury-Related Factors Affecting Survival Rate
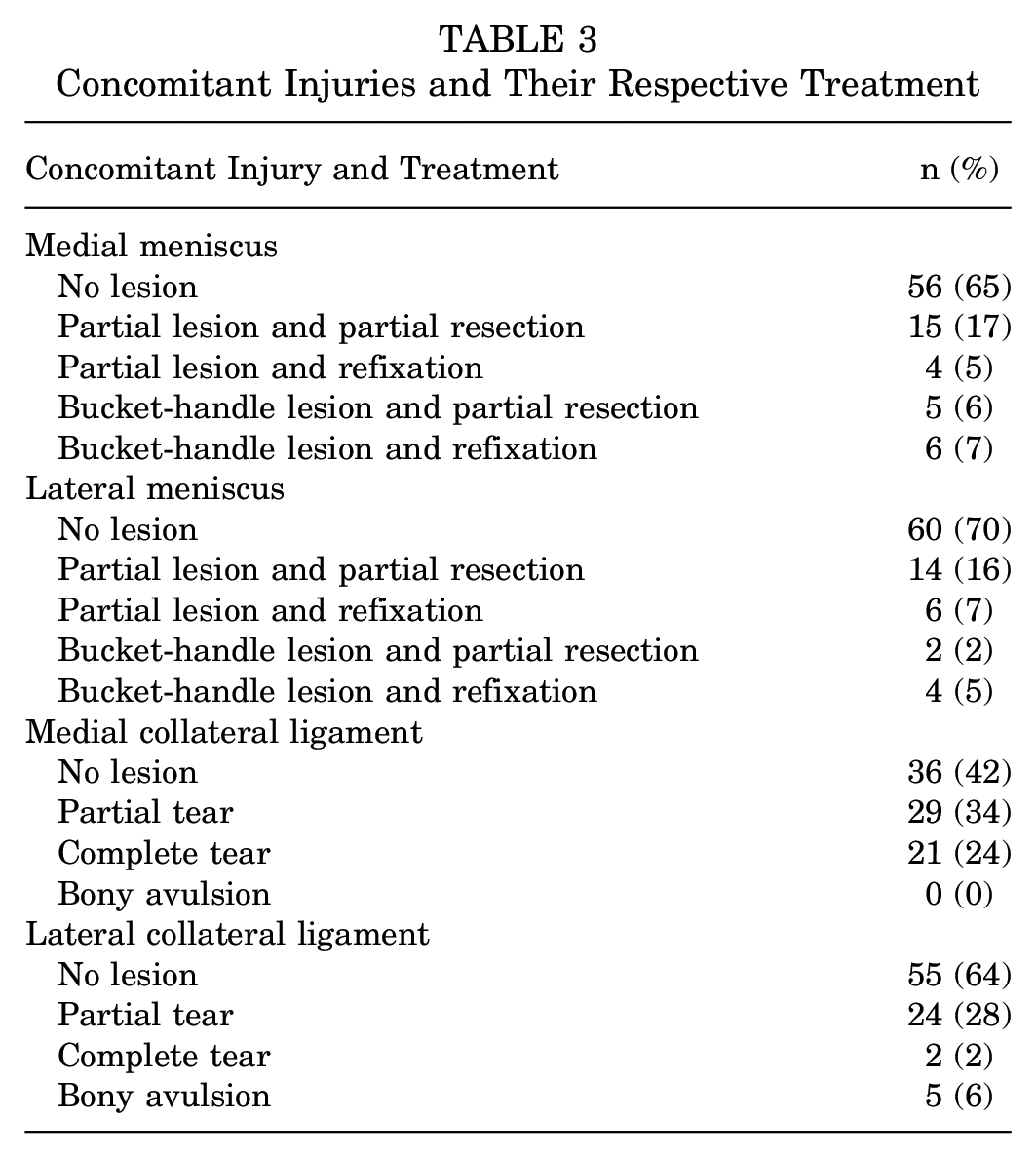
Concomitant injuries (Table 3) of the medial meniscus (P = .860), the lateral meniscus (P = .414), the medial collateral ligament (P = .801), and the lateral collateral ligament (P = .534) had no statistically significant impact on the revision-free survival rate. The median delay from injury to surgery was 1 day (IQR, 0-1 day), with a maximum delay of 18 days, and similar to concomitant injuries, a delay in surgery had no statistically significant impact on the revision-free survival rate of the ACL repair (P = .277).
Concomitant Injuries and Their Respective Treatment
Discussion
The main findings of our study were as follows: (1) The revision rate at the 2-year follow-up after ACL repair with SA was 10%. (2) Patient-related factors—such as sex, age, and BMI—as well as (3) injury-related factors—such as concomitant ligamentous and meniscal injuries or a delay in surgery—were not associated with a lower revision-free survival rate.
The revision rate of 10% at the 2-year follow-up is slightly lower or similar to that of previously described cohorts in ACL repair with SA. Within the cohort of the first 11 patients treated with this surgical technique, DiFelice et al 6 reported 2 revision surgeries (18%) at a mean follow-up of 6 ± 1.5 years. While one patient sustained an atraumatic rerupture 3 months postoperatively and was admittedly noncompliant with the postoperative rehabilitation protocol, the other patient sustained a traumatic twisting injury playing football 2.5 years postoperatively and sustained a medial meniscus lesion and a partial retear of the ACL. 6 Jonkergouw et al 12 studied 27 patients who underwent ACL repair with SA, and they observed 2 traumatic ACL retears at a mean follow-up of 3.2 ± 1.7 years; 1 in a football player 1.4 years postoperatively and 1 in a gymnastics athlete 1.1 years postoperatively, respectively, as well as 2 irritating tibial anchors that required partial anchor removal, led to an overall revision rate of 15%. Interestingly, although the same tibial anchor fixation was used in the present cohort, and despite a nearly 4-fold number of treated patients, we did not experience a single patient with tibial anchor irritation. It remains unclear whether the different technique of femoral fixation with an intra-articular anchor used by Jonkergouw et al 12 and DiFelice et al 6 might play a role in these tibial anchor irritations due to higher/lower tension of the SA construct. Future follow-up examinations will show whether these problems are unique or will occur more frequently regardless of the femoral and tibial fixation technique.
Cruz et al 4 reported the highest revision rate after ACL repair with SA in a high-demand military cohort of 46 patients. At the 2-year follow-up, they found a revision rate of 26.1%. Nonetheless, with a mean time from injury to surgery of 96.8 ±77.4 days, the degree of strictness with which this cohort's patients were selected remains to be questioned, as the shortest injury-to-surgery interval was still longer than the longest interval within the presented cohort. 4 In a prospective cohort study, Douoguih et al 7 reported a revision rate of 10% in 30 patients undergoing ACL repair with SA. All 3 patients undergoing revision surgery sustained a traumatic retear: playing volleyball (17 months postoperatively), playing soccer in an Olympic development team (11 months after surgery), and playing competitive recreational soccer (12 months after surgery), respectively. 7
In ACL research, retear rates should not be considered and interpreted as a stern parameter. Surgical techniques that lead to high rates of return to competitive sports inevitably will have higher retear rates than an approach with only a limited resumption of sporting activities. Thus, ACL retear rates should always be further itemized as traumatic versus atraumatic retear and adequate major or minor trauma and interpretated in combination with other clinical parameters such as the level of pre- and postoperatively performed sports.
Patient-related factors—such as sex, age, BMI, and the preinjury level of sport—were not associated with a lower survival rate of ACL repair with SA. However, previous studies have described a younger patient age and a higher level of performed sports before injury as risk factors for a retear. Cruz et al 4 found that ages ≤17 and ≥35 years and performing sports at an elite level are independent patient-related risk factors for failure of the ACL repair with SA. However, in their systematic review, van Eck et al 8 reported contrary findings regarding patient age and concluded that ACL repair has “a better outcome in younger patients, specifically in the skeletally immature.” These findings are backed by porcine studies that observed improved structural properties of the ACL remnant and a better healing potential in the skeletally immature, and they are also supported by clinical studies and the findings of the presented cohort, which saw favorable or equivalent results in underage patients.2,5,8,14,26
We also could not determine that a higher level of sports performed before injury was a risk factor for revision surgery, despite several elite athletes included in our cohort and a previous report of successful ACL repair with SA in an Olympic sportsman. 17 Furthermore, injury-related factors— such as concomitant injuries or a delay of surgery of up to 18 days—were not associated with a higher risk for revision surgery in our cohort. Concomitant injuries were initially seen as a contraindication to performing an ACL repair with SA 6 ; however, studies have included patients with concomitant ligamentous, meniscal, and chondral lesions with an ACL injury but have not assessed them as potential risk factors for revision surgery.7,12 In their analysis, Cruz et al 4 were not able to identify meniscal or chondral concomitant injuries as a risk for revision surgery after ACL repair with SA.
Cruz et al 4 reported a significantly higher mean interval between injury and surgery in the failure group (164 ± 59 days compared with 107 ± 98 days in the nonfailure group). These long intervals between injury and surgery are no rarity in the literature, as Jonkergouw et al 12 reported a median time to surgery of 26 days with a maximum delay of 155 days and DiFelice et al 6 reported a mean delay of 39 days. Previous studies have emphasized that a delay of even 2 or 6 weeks of ACL repair may lead to histological changes compromising tissue quality, leading to retraction of the ACL remnant and possibly affecting the healing and postoperative functional outcome of the augmented ACL repair.13,15,22 Thus, the infrastructure in our clinic was organized so that the delay of surgery was kept short. It remains unclear whether, in the aforementioned cohorts, the intraoperative tissue quality was still sufficient enough for ligament preservation or whether histological changes had already begun to compromise the healing potential.
Limitations
We should acknowledge several limitations: (1) This was a retrospective study; thus, patients undergoing revision surgery elsewhere may have been lost to follow-up. In addition, not all patients with a retear or residual functional instability will choose to have revision surgery. Thus, the presented results need to be interpreted as low-end estimates. However, the follow-up regarding required revision surgeries was available for 86 of 93 patients (92.5%), a higher follow-up rate than in most comparable studies. 7 (2) An analysis of risk factors depends on a sufficient distribution of these risk factors. While we were not able to detect a delay of surgery to be a risk factor for revision surgery, we must acknowledge that with a median delay of 1 day and a maximum delay of only 18 days, the delay in surgery of our cohort might have been too short to sufficiently detect the tipping point at which the tissue quality began to decline and retraction of the ACL remnant became crucial. (3) The patient cohort lacked an objective measure of postoperative integrity and healing of the ACL. A postoperative MRI was only performed in symptomatic patients suspicious of an ACL retear or exhibiting functional instability. Thus, the given results should again be interpreted as low-end estimates. (4) All but 2 patients in the cohort sustained their acute ACL tear in winter sports. Weaver et al 28 pointed out that skiing injuries predominantly lead to proximal ACL tear patterns, pivotal for patient selection for ACL repair with SA. Thus, it remains unclear whether the findings of this study are equally valid for ACL injuries outside winter sports. (5) Finally, we must acknowledge a sparse data bias for some risk factors and events.
Conclusion
The revision-free survival rate of ACL repair with SA was 93% at the 2-year-follow-up. When strict patient selection regarding tear pattern and tissue quality were applied, patient-related factors—such as sex, age, BMI or preinjury level of sports—as well as injury-related factors—such as concomitant meniscal and ligamentous injuries or a delay in surgery of up to 18 days—were not associated with a higher risk for revision surgery.
Footnotes
Acknowledgements
The authors thank Anita Baschung, Iris Pellegrinelli, Katrin Spieske, and Michael Bauer for their help with data collection, data management, and statistical analysis.
Final revision submitted December 14, 2023; accepted February 2, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Verfügung der Kanotonalen Ethikkommission Zürich (ref No. 2019-00758).